Download as docx, pdf, or txt
You might also like
- ATI Pharmacology Study Guide 2021Document41 pagesATI Pharmacology Study Guide 2021Jennifer Weeks100% (2)
- Flowchart TB DOTSDocument11 pagesFlowchart TB DOTSalfredtan6288No ratings yet
- 5.ocd Case PresentationDocument31 pages5.ocd Case Presentationpravallika vanguru100% (1)
- Pharm 2013Document13 pagesPharm 2013Shae Thomas100% (6)
- Ondansetron - Cahulogan, JPDocument9 pagesOndansetron - Cahulogan, JPpearl japsonNo ratings yet
- Quiz 5Document28 pagesQuiz 5YNo ratings yet
- Prescriptions 4 MoDocument68 pagesPrescriptions 4 MoViraaj SinghNo ratings yet
- Palliative Care FormularyDocument12 pagesPalliative Care FormularyRicardo FernandesNo ratings yet
- About The MedicinesDocument35 pagesAbout The Medicinesrohan NathNo ratings yet
- Drug Study CardinalDocument21 pagesDrug Study CardinalDrei LanuzoNo ratings yet
- Drug Study of SchizophreniaDocument17 pagesDrug Study of SchizophreniaCLOYD MARVINNo ratings yet
- Symph A To Mimetic SDocument27 pagesSymph A To Mimetic Sjl frusaNo ratings yet
- Corticosteroid Guidelines PDFDocument6 pagesCorticosteroid Guidelines PDFMariskaNo ratings yet
- Neuropathic Pain Guidance April 2023 v1.2Document6 pagesNeuropathic Pain Guidance April 2023 v1.2Germán Bernate ObandoNo ratings yet
- Managing Patients With Chronic AnginaDocument10 pagesManaging Patients With Chronic Anginacindyfuller68No ratings yet
- Steroid Guidelines Summary 2008Document2 pagesSteroid Guidelines Summary 2008Iniya RajendranNo ratings yet
- Medication CardsDocument5 pagesMedication CardsAndrew Harrison Lewis0% (1)
- Case Study (20%) : Know Your MedicineDocument11 pagesCase Study (20%) : Know Your MedicineMOHD MU'IZZ BIN MOHD SHUKRINo ratings yet
- Management of Reactions in Leprosy: How Should Lepra Reactions Be Managed?Document2 pagesManagement of Reactions in Leprosy: How Should Lepra Reactions Be Managed?Echa AdityaNo ratings yet
- Pharma Midterm ExamDocument16 pagesPharma Midterm ExamChriscel Ann EspirituNo ratings yet
- Tanzania STG 052013-Copy 1544379670122Document220 pagesTanzania STG 052013-Copy 1544379670122Waqar WikiNo ratings yet
- OndansetronDocument11 pagesOndansetronIlyes FerenczNo ratings yet
- Treatment of Leprosy ReactionsDocument2 pagesTreatment of Leprosy ReactionsMaria lestari harianjaNo ratings yet
- XII Discharge PlanningDocument1 pageXII Discharge PlanningkristineNo ratings yet
- Tramadol HydrochlorideDocument5 pagesTramadol HydrochlorideSebastian CruzNo ratings yet
- Pediatric Pain and Symptom Management Guidelines: Dana Farber Cancer Institute/Boston Children's HospitalDocument27 pagesPediatric Pain and Symptom Management Guidelines: Dana Farber Cancer Institute/Boston Children's HospitalDaeng Anggit AdirahmanNo ratings yet
- PrescribingDocument31 pagesPrescribingYavani KulasinghamNo ratings yet
- JDH Pocket Pain GuideDocument2 pagesJDH Pocket Pain Guidesgod34100% (1)
- Core Safety ProfileDocument13 pagesCore Safety ProfileneleatucicovshiiNo ratings yet
- Acetaminophen Drug StudyDocument7 pagesAcetaminophen Drug StudyHugh Klied ItuhatNo ratings yet
- Pain ManagementDocument32 pagesPain ManagementShania CandaNo ratings yet
- M. Gilang H - TOPIK 7Document10 pagesM. Gilang H - TOPIK 7Givani MaqilaNo ratings yet
- V. Atypical AntipsychoticsDocument2 pagesV. Atypical AntipsychoticsChristine Pialan SalimbagatNo ratings yet
- Integrated Therapeutics IiiDocument15 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Weekly Drug CardsDocument43 pagesWeekly Drug CardsErica SanchezNo ratings yet
- Neuropathic Pain TreatmentDocument8 pagesNeuropathic Pain TreatmentIrimes MariaNo ratings yet
- Drug Study 1Document10 pagesDrug Study 1neeraj chauhanNo ratings yet
- Check Your English Vocabulary For IELTS 4thDocument5 pagesCheck Your English Vocabulary For IELTS 4thSeema RaniNo ratings yet
- Lisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationDocument6 pagesLisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationCliff by the seaNo ratings yet
- Kaka Reading and Ds 2Document17 pagesKaka Reading and Ds 2Suzanne AndresNo ratings yet
- Care Plan:, Wrong, Wrong, Wrong, WrongDocument8 pagesCare Plan:, Wrong, Wrong, Wrong, Wronglovelylife theNo ratings yet
- Lisinopril PDFDocument3 pagesLisinopril PDFHannaNo ratings yet
- Status Epilepticus and ICPDocument9 pagesStatus Epilepticus and ICPjoomds51No ratings yet
- Pharmacology: Drug MonitoringDocument43 pagesPharmacology: Drug MonitoringMa GynNo ratings yet
- BOOST Pharm Exam 2 Review - BLANKDocument20 pagesBOOST Pharm Exam 2 Review - BLANKHwi GNDCNo ratings yet
- Lo Week 4-2Document4 pagesLo Week 4-2Martien Silviandy SetiawanNo ratings yet
- WHO Step Ladder For PainDocument5 pagesWHO Step Ladder For PainRizKyImanSariNo ratings yet
- Sedation Protocols For DogsDocument2 pagesSedation Protocols For DogsSk LoonaNo ratings yet
- Rishum 3 03821017Document22 pagesRishum 3 03821017moiseancuta87No ratings yet
- OpioidsDocument3 pagesOpioidsEva K. Al KaryNo ratings yet
- Medications: Medication Name Generic/Trade Classification Pregnancy CategoryDocument8 pagesMedications: Medication Name Generic/Trade Classification Pregnancy CategoryapalestiNo ratings yet
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakNo ratings yet
- Otezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductDocument22 pagesOtezla 10 MG Film-Coated Tablets: 1. Name of The Medicinal ProductSunil SewakNo ratings yet
- Palliative Pain Management in The Er: UBC EM Palliative Medicine Day Lindsay Cohen July 27, 2016Document31 pagesPalliative Pain Management in The Er: UBC EM Palliative Medicine Day Lindsay Cohen July 27, 2016b BNo ratings yet
- Symptom Control and Caring For The Dying Patient 4th EditionDocument26 pagesSymptom Control and Caring For The Dying Patient 4th EditionLaurencia LenyNo ratings yet
- 6 Palliative CareDocument4 pages6 Palliative CareDiana VillanuevaNo ratings yet
- Indever PDFDocument4 pagesIndever PDFbiddut95No ratings yet
- Drug StudyDocument7 pagesDrug Studykristen_ramos_3No ratings yet
- Medications Sheet PreopDocument37 pagesMedications Sheet Preopapi-503879428No ratings yet
- Drug Study For AMCDocument3 pagesDrug Study For AMCTrixia RiveraNo ratings yet
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcFrom EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcNo ratings yet
- Herbs Ni TatayDocument39 pagesHerbs Ni TatayI-Reen FrancisquiteNo ratings yet
- Tiki Taka CK SurgeryDocument50 pagesTiki Taka CK SurgeryEmad MerganNo ratings yet
- HAB ManualDocument102 pagesHAB ManualSven OrdanzaNo ratings yet
- 2020 06 18 Coronavirus Covid 19 Infection in PregnancyDocument61 pages2020 06 18 Coronavirus Covid 19 Infection in PregnancyIndah AulliaNo ratings yet
- 50 One Liners - Neet PG PDFDocument3 pages50 One Liners - Neet PG PDFNivya Mary0% (1)
- Jurnal Forensik 1 (Kelompok 2)Document6 pagesJurnal Forensik 1 (Kelompok 2)Rifqi UlilNo ratings yet
- ValsartanDocument12 pagesValsartanAS RifathNo ratings yet
- Latest MAPEH Reviewer 7 LET EXAM Questions AnswersDocument6 pagesLatest MAPEH Reviewer 7 LET EXAM Questions Answers荷花No ratings yet
- Continue Medical Care-Anand YncDocument18 pagesContinue Medical Care-Anand YncAnand gowda89% (9)
- Lung Function TestingDocument217 pagesLung Function TestingMazurencoIana100% (2)
- Polycythemia VeraDocument22 pagesPolycythemia VeraMelisande Rae CiruelaNo ratings yet
- contentdamcenteneSunshinepdfsMMA Reg4 PDFDocument501 pagescontentdamcenteneSunshinepdfsMMA Reg4 PDFShawn SherwoodNo ratings yet
- List of Programs Applied To PDFDocument10 pagesList of Programs Applied To PDFRamanpreet Kaur Maan100% (1)
- Tobradex Eye Drops: Consumer Medicine InformationDocument5 pagesTobradex Eye Drops: Consumer Medicine InformationFranc VenturaNo ratings yet
- UntitledDocument10 pagesUntitledMitsury Jacqueline Flores C.No ratings yet
- Pharmacy ListDocument115 pagesPharmacy ListacroxmassNo ratings yet
- Report On AmoebiasisDocument36 pagesReport On Amoebiasisrhimineecat71No ratings yet
- A Patient With Pancytopenia: Section I: HistoryDocument12 pagesA Patient With Pancytopenia: Section I: HistoryHadia AamirNo ratings yet
- GGP - Six StepsDocument28 pagesGGP - Six StepsDina SeptianaNo ratings yet
- Cues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentDocument2 pagesCues/Needs Nursing Diagnosis Rationale Goals and Objectives Interventions Rationale Evaluation Subjective Data: IndependentArabelle GONo ratings yet
- Physiotherapy After Traumatic Brain Injury: A Systematic Review of The LiteratureDocument9 pagesPhysiotherapy After Traumatic Brain Injury: A Systematic Review of The LiteratureVeronika AtaNo ratings yet
- Thornwaldt Cyst - A Disease or AnomalyDocument4 pagesThornwaldt Cyst - A Disease or AnomalyresearchparksNo ratings yet
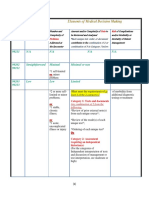
- 3-Level of MDMDocument3 pages3-Level of MDMmedical codingNo ratings yet
- Benign Paroxysmal Positional Vertigo Diagnosis and Treatment PDFDocument11 pagesBenign Paroxysmal Positional Vertigo Diagnosis and Treatment PDFholly theressaNo ratings yet
- CV AgtDocument6 pagesCV AgtHafzhy TravelNo ratings yet
- The Pathophysiology & Practical Management of Diabetic KetoacidosisDocument45 pagesThe Pathophysiology & Practical Management of Diabetic KetoacidosisPreetibah PatelNo ratings yet
- Study Guide Chest Tube DrainageDocument5 pagesStudy Guide Chest Tube DrainageDan Dan ManaoisNo ratings yet
- Vastarel MR From Decades of Clinical Experience inDocument6 pagesVastarel MR From Decades of Clinical Experience inJonathan Ian ArinsolNo ratings yet
- PPT Case NephrolithiasisDocument45 pagesPPT Case NephrolithiasisRifka Anisa0% (1)