Professional Documents
Culture Documents
Health Expectations - 2014 - Greenfield - Analysing Big Picture Policy Reform Mechanisms The Australian Health Service
Health Expectations - 2014 - Greenfield - Analysing Big Picture Policy Reform Mechanisms The Australian Health Service
Uploaded by
Hellen MunetsiOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Health Expectations - 2014 - Greenfield - Analysing Big Picture Policy Reform Mechanisms The Australian Health Service
Health Expectations - 2014 - Greenfield - Analysing Big Picture Policy Reform Mechanisms The Australian Health Service
Uploaded by
Hellen MunetsiCopyright:
Available Formats
doi: 10.1111/hex.
12300
Analysing ‘big picture’ policy reform mechanisms:
the Australian health service safety and quality
accreditation scheme
David Greenfield PhD,* Reece Hinchcliff PhD,† Margaret Banks MHA,‡ Virginia Mumford
MBBS,§ Anne Hogden PhD,¶ Deborah Debono BA (Psych Hons),** Marjorie Pawsey
MBBS,† Johanna Westbrook PhD†† and Jeffrey Braithwaite PhD‡‡
*Associate Professor, †Visiting Research Fellow, §Doctoral Scholar, ¶Research Fellow, **Research Officer, ‡‡Professor and
Director, Centre for Clinical Governance Research, Australian Institute of Health Innovation, University of New South Wales,
Sydney, NSW, ‡Senior Program Director, Australian Commission on Safety and Quality in Health Care, Sydney, NSW and
††Professor and Director, Centre for Health Systems and Safety Research, Australian Institute of Health Innovation, University
of New South Wales, Sydney, NSW, Australia
Abstract
Correspondence Background Agencies promoting national health-care accreditation
David Greenfield PhD
Associate Professor
reform to improve the quality of care and safety of patients are
Faculty of Medicine largely working without specific blueprints that can increase the
Australian Institute of Health likelihood of success.
Innovation
University of New South Wales Objective This study investigated the development and implemen-
AGSM Building
tation of the Australian Health Service Safety and Quality Accred-
Sydney
NSW 2052 itation Scheme and National Safety and Quality Health Service
Australia Standards (the Scheme), their expected benefits, and challenges
E-mail: d.greenfield@unsw.edu.au and facilitators to implementation.
Accepted for publication
9 October 2014 Methods A multimethod study was conducted using document
Keywords: accreditation, health
analysis, observation and interviews. Data sources were eight gov-
policy, healthcare quality assurance, ernment reports, 25 h of observation and 34 interviews with 197
healthcare reform, policy development diverse stakeholders.
Results Development of the Scheme was achieved through exten-
sive consultation conducted over a prolonged period, that is, from
2000 onwards. Participants, prior to implementation, believed the
Scheme would produce benefits at multiple levels of the health sys-
tem. The Scheme offered a national framework to promote patient-
centred care, allowing organizations to engage and coordinate
professionals’ quality improvement activities. Significant challenges
are apparent, including developing and maintaining stakeholder
understanding of the Scheme’s requirements. Risks must also be
addressed. The standardized application of, and reliable assessment
against, the standards must be achieved to maintain credibility with
the Scheme. Government employment of effective stakeholder
engagement strategies, such as structured consultation processes,
was viewed as necessary for successful, sustainable implementation.
3110 ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Analysing health policy reform mechanisms, D Greenfield et al. 3111
Conclusion The Australian experience demonstrates that national
accreditation reform can engender widespread stakeholder support,
but implementation challenges must be overcome. In particular,
the fundamental role of continued stakeholder engagement
increases the likelihood that such reforms are taken up and spread
across health systems.
set of criteria, and for each criteria, a series of
Introduction
actions are required to be fulfilled. Each action
Despite international efforts and investments is designated as either core, and critical for
over several decades, health care causes signifi- safety and quality, or developmental, denoting
cant preventable harm to patients, worldwide.1–3 aspirational targets.12 The NSQHS Standards
Health professionals, including clinicians, are assessed against a three-point rating scale:
managers and researchers, are increasingly ‘not met’ – the actions required have not been
applying ideas, strategies and initiatives, the achieved; ‘satisfactorily met’ – the actions
purpose of which is to reduce harm and required have been achieved; and ‘met with
improve efficiency and the delivery of care.4 merit’ – in addition to achieving the actions
This orientation is reinforced by consumer required, measures of good-quality and a
demands for improved safety and quality in higher level of achievement are evident. In
health care. At times, governments respond exceptional circumstances, an action may be
using policy levers.5,6 Introducing or revamp- rated as ‘not applicable’ in a specific context.13
ing national accreditation reform is one type To achieve accreditation, all core actions (209
of common policy response.7,8 Accreditation for hospitals and 208 for day procedure cen-
programmes are reputed to stimulate systems- tres) must be demonstrated by health services,
level improvement by promoting uptake of and in doing so, each standard satisfied.
optimal, evidence-based governance and clini- The impact of this national reform is signifi-
cal standards.9,10 cant and on-going. At present, there is limited
In Australia, in 2013, systems-level accredita- publicly available international research evi-
tion reform recently occurred with the imple- dence to guide agencies responsible for devel-
mentation of the Australian Health Service oping and implementing such programmes.14,15
Safety and Quality Accreditation (AHSSQA) This knowledge gap compels policymakers to
Scheme (the Scheme). The effectiveness of the rely on their own unfolding experience, expert
Scheme, overseen by the Australian Commis- opinion and small-scale pilot evaluations when
sion on Safety and Quality in Health Care undertaking national accreditation reforms.16
(ACSQHC), was dependent on five inter- Our study examined the Australian experience
related stakeholder groupings with assigned of national reform involving the new accredita-
roles (Table 1). tion system being applied to all acute care
Central to the reform has been the develop- health services. This multimethod qualitative
ment and application of National Safety and study investigated stakeholder perceptions of
Quality Health Service (NSQHS) Standards. the development, expected benefits, challenges
The NSQHS Standards are a set of 10 evi- and enablers of the Scheme. Challenges and
dence-based improvement strategies for health facilitation factors arising from the Australian
service organizations, which focused on areas experience are outlined. The key findings can
considered essential to improving patient care, inform strategic design and implementation of
such as promoting consumer engagement comparable international reforms, increasing
(Standard 2) and reducing infection rates their potential to achieve patient safety
(Standard 3) (Table 2).11 Each Standard has a benefits.
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
3112 Analysing health policy reform mechanisms, D Greenfield et al.
Table 1 Stakeholders involved in, and activities undertaken for, key elements of the AHSSQA Scheme42
Stakeholders Element Activities
Health Ministers Overall responsibility for the Endorse the NSQHS Standards
governance of the Scheme Receive regular information on the health system’s
performance against the Standards
ACSQHC Body charged with the task of A National Coordination Program undertakes the
implementing and managing following: development and maintenance of the NSQHS
the Scheme Standards (revision due in 2015); advising Health
Ministers on the scope of the Scheme; approval of
accrediting agencies to assess against the NSQHS
Standards; on-going liaison with regulators and
approved accrediting agencies to promote improvement
to the Scheme; and annual reporting to Health
Ministers on safety and quality across the health
system.
State, territory and Manage the operation of the The regulators adopt the NSQHS Standards and
Commonwealth accreditation process for their determine which health services are to be accredited.
regulatory agencies jurisdiction They receive relevant accreditation data, sensitive to
(regulators) operational context, as a performance measure of
health services. Where the Standards are not met,
regulators commence a series of escalating actions to
remediate the service and ensure the NSQHS Standards
are eventually met.
Health services Provide health care to individuals Health services assess against the NSQHS Standards
and the community and select an approved accrediting agency to assess
their compliance.
Approved accreditation Assess health services against the Accrediting agencies apply and are granted approval if they
agencies NSQHS Standards meet ACSQHC criteria. As a minimum, this involves being
accredited by an internationally recognized certification
body. Approved accrediting agencies assess health services
against the NSQHS Standards. They provide accreditation
information to the health services, regulators and the
ACSQHC and agree to work with the ACSQHC to ensure
national consistency in the interpretation of the NSQHS
Standards and assessment processes.
Standards and Accreditation Agency). Federal
Methods
and State Government safety and quality agen-
This study forms one part of the ACCREDIT cies are also represented, including the ACS-
(Accreditation Collaborative for the Conduct QHC and the New South Wales Clinical
of Research, Evaluation and Designated Inves- Excellence Commission. The UNSW Human
tigations through Teamwork) Project, led by Research Ethics Committee approved the study
researchers at the Australian Institute of (HREC Approval No: 10274). Written consent
Health Innovation, University of New South was gained from participants prior to partici-
Wales (UNSW).17–20 Collaborators include pation in the study.
prominent accreditation agencies from the A multimethod investigation was conducted
Australian acute, primary and aged care sec- of the implementation, enabling triangulation
tors: The Australian Council on Healthcare of findings.21 Semi-structured interviews were
Standards; Australian General Practice Accred- employed, accompanied by document analysis
itation Limited; and the Australian Aged Care and observational research (Table 3). The util-
Quality Agency (formerly the Aged Care ity of mixed qualitative methods for examining
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Analysing health policy reform mechanisms, D Greenfield et al. 3113
Table 2 Summary of the NSQHS Standards32
Standard Descriptions
1. Governance for safety and quality in The quality framework used by organizations to implement safe systems.
health service organizations
2. Partnering with consumers Systems and strategies used to create a consumer-centred health system
by including consumers in the development and design of quality health care.
3. Preventing and controlling Systems and strategies used to prevent infection of patients within the
health-care-associated infections health-care system and to manage infections effectively when they occur
to minimize the consequences.
4. Medication safety Systems and strategies to ensure clinicians safely prescribe, dispense and
administer appropriate medicines to informed patients.
5. Patient identification and Systems and strategies used to identify patients and correctly match their
procedure matching identity with the correct treatment.
6. Clinical handover Systems and strategies used for effective clinical communication whenever
accountability and responsibility for a patient’s care is transferred.
7. Blood and blood products Systems and strategies for the safe, effective and appropriate management
of blood and blood products so that patients receiving blood are safe.
8. Preventing and managing Systems and strategies used to prevent patients developing pressure injuries,
pressure injuries and employment of best practice management when pressure injuries occur.
9. Recognizing and responding to clinical Systems and processes to be implemented by health services to respond
deterioration in acute health care effectively when patients’ clinical condition deteriorates.
10. Preventing falls and harm from falls Systems and strategies used to reduce the incidence of patient falls in
health services, and employment of best practice management when
falls do occur.
health policy reform processes has been estab- in particular, key issues regarding implementa-
lished.22 Data collection focused on three tion challenges and facilitators were noted. The
issues: how the Scheme was developed; expec- observational research was conducted by two
tations regarding its benefits; and perceptions researchers with experience applying ethno-
of key implementation challenges and facilita- graphic methods in health care.23–25
tion factors. The ACSQHC website was Interviews were undertaken with a cross
reviewed for publicly available information section of Australian health-care accreditation
concerning the Scheme. Eight reports were stakeholders. In late 2011, management teams of
analysed to identify relevant information accreditation agencies involved in ACCREDIT
regarding the main study foci. provided the contact details of representatives
Twenty-five hours were allocated to observing from organizations they viewed as key stake-
the operation of two committees, the ‘Regulators holder groups, such as government quality
Working Group’ and the ‘Accrediting Agencies improvement agencies, accreditation agencies
Working Group’, convened by the ACSQHC, and health-care professional associations. Invita-
which led the design of the Scheme and facilitated tions were emailed to the representatives inviting
its implementation. The ‘Regulators Working them to participate in the study. A convenience
Group’ comprised 20 representatives of agencies sample of health-care professionals was recruited
responsible for the coordination of acute public at accreditation educational workshops held in
and private health services in each Australian every Australian state and territory during early
state and territory. The ‘Accrediting Agencies 2012. Also arranged at this time was a group
Working Group’ involved representatives of 16 interview with consumer representatives from a
accreditation agencies operating in Australia. In peak national organization representing the
all, five committee meetings were observed, and rights, needs and interests of older Australians.
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
3114
Table 3 Overview of methods, participants and data
Data sources
Study methods Reports
Document analysis Australian Commission on Safety and Quality in Health Care (ACSQHC) (2006). Discussion paper:
national safety and quality accreditation standards. Sydney, Australia, ACSQHC.
Australian Commission on Safety and Quality in Health Care (ACSQHC) (2010). National safety
and quality health service standards and their use in a model national accreditation scheme:
decision regulatory impact statement. Sydney, Australia, ACSQHC.
Australian Commission on Safety and Quality in Health Care (ACSQHC) (2011). National safety
and quality health service standards. ACSQHC. Sydney, Australia, Commonwealth of Australia.
Australian Commission on Safety and Quality in Health Care (ACSQHC) (2012). Accreditation
outcome results and evidence of implementation of the National Safety and Quality Health
Service (NSQHS) Standards. Sydney, Australia, ACSQHC.
Australian Commission on Safety and Quality in Health Care (ACSQHC). (2013). ‘Development
of the national safety and quality health service standards’. Retrieved 13 May,
from http://www.safetyandquality.gov.au/our-work/accreditation/development-of-the-standards-
and-model-national-accreditation-scheme/.
Australian Commission on Safety and Quality in Health Care (ACSQHC) (2013). Hospitals: core
Analysing health policy reform mechanisms, D Greenfield et al.
and developmental actions. National Safety and Quality Health Service Standards. Sydney, Australia.
Australian Council for Safety and Quality in Health Care (ACSQHC) (2003). Standards setting and
accreditation literature review and report. ACSQHC. Canberra, Australia.
Australian Council for Safety and Quality in Health Care (ACSQHC) (2003). Standards setting and
accreditation systems in health: consultation paper. ACSQHC. Canberra, Australia.
Activities
Observations ACSQHC Regulators Working Group: 20 representatives 25 h of non-participant observations
ACSQHC Accrediting Agencies Working Group: 16 representatives
Stakeholder categories Interviews and participants (n)
Interviews Health-care professionals 10 (51)
Accreditation agency management groups 4 (47)
Professional colleges and associations 6 (38)
Government health-care agency representatives 9 (35)
Accreditation agency surveyors/assessors 4 (18)
Health-care consumers 1 (8)
Totals 34 (197)
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Analysing health policy reform mechanisms, D Greenfield et al. 3115
This organization, with bodies in each state and
Policy agenda setting: 2000–2006
territory in Australia, undertakes national policy
The former Australian Council for Safety and
and advocacy from the perspective of older peo-
Quality in Health Care initiated a detailed
ple as citizens and consumers. Group interviews
review of standards setting and accreditation in
were preferred for their ability to elicit commu-
2000.27–29 On the basis of the findings, the
nication between participants, which helped
Australian Health Minister’s Council estab-
generate comparative as well as individual per-
lished a Review of Future Governance Arrange-
spectives.26 Only where potential participants
ments for Safety and Quality in 2004,30 which
could not attend group sessions were individual
proposed designing a new accreditation system
interviews presented as an option. Interviews
capable of ensuring on-going, national replica-
lasted between 30 and 90 min, were digitally
tion of evidence-based processes associated
recorded and professionally transcribed. In total,
with safety and quality.11 The ACSQHC was
there were 34 interviews (31 groups and three
established in 2006 and was charged with
individual) with 197 participants, who collec-
coordinating this reform, with three specific
tively represented the diversity of stakeholders
objectives: outline potential evidence-based
influencing the development and implementation
improvements to existing systems; develop a
of the reform.
national set of accreditation standards against
Transcripts were thematically analysed21
which health services could be assessed; and
using textual grouping software, NVivo v.9,25
provide recommendations to guide implemen-
to facilitate systematic classification of data.
tation processes.31
Similarly, reports and observation notes were
subject to analysis using the three predeter-
mined study issues to guide data classification. Stakeholder consultation and impact assessment:
As the aim was to uncover participants’ views 2006–2011
and ideas, there were no size limits placed on Between 2006 and 2011, the ACSQHC engaged
segments of coded text.21 Systematic coding of in extensive, nationwide consultation of health-
data was completed by one researcher, and the care stakeholder groups and individuals to gain
research team collaboratively reviewed the cod- input to the review, including Federal and
ing and iteratively developed the findings State Government regulators, accreditation
through on-going discussions. agencies, insurers, health services, research
experts and consumers.32 Diverse consultation
mechanisms were employed,31,32 including the
Results development of technical and expert working
The results are structured according to the groups; the release of public consultation
three aims of the study. The three sections papers outlining proposed reforms; piloting of
report stakeholder perceptions about how the the proposed scheme; and on-going reporting
Scheme developed, expected benefits, and key to Australian Health Ministers. Study partici-
implementation challenges and facilitators of pants indicated that extensive consultation was
the Scheme. necessary due to the critical or cynical percep-
tions of the reform measures initially held by
many prominent accreditation stakeholders
Stakeholder perceptions about how the and State Government health departments.
Scheme developed
The Commission is an extension of the executive
Reform of accreditation commenced a decade of government and it’s very dangerous because
before implementation. Three interlinked phases they are funded by government. And if the
were involved: policy agenda setting, stake- standards start getting diluted, watered down
there will be healthcare implications. (Accredita-
holder consultation and impact assessment, and
tion agency representative, Focus group #26)
policy finalization and introduction.
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
3116 Analysing health policy reform mechanisms, D Greenfield et al.
In total, the ACSQHC arranged 227 separate procedure centres. The ACSQHC continues to
consultation activities involving over 1000 undertake wide-ranging activities, including on-
stakeholders spanning the breadth of the Aus- going consultation with health services, to facili-
tralian health system.32 When asked to assess tate effective implementation of the Scheme. A
the Scheme’s development, participants empha- revision of the NSQHS Standards is scheduled
sized the influential role of the ACSQHC in for 2015 to assess their continued relevance,
effectively coordinating the reform by aligning explanation and application.32
stakeholder interests.
It’s probably been one of the best processes that Expected benefits
I’ve been involved with, in terms of real consulta-
tion. . . just the constant feedback of opinions and Participants expected the Scheme to enhance
the clarification. . . All of the people [ACSQHC] patient-centred care at each level of the health
have been extremely respectful of difference, system, that is, to promote the engagement of
because if you’re talking about a regulatory envi- clinicians in patient quality improvement
ronment, we’ve got every State and Territory who
activities, assist health services to improve sys-
organises everything in such a disparate way, and
they’ve all got their focus areas, but just the tems used to identify and respond to patient
amount of respect that’s been shown, but still safety problems and implement standardiza-
coming to some decision about things and trying tion, integration and transparency for the
to push a national agenda. . . I thought it was health system through a national safety and
impressive. (State Government health department
quality framework.
representative, Focus group #19)
The NSQHS Standards are evidence-based
In addition to consultation activities, a regu- and largely clinically focused, which was con-
latory impact statement was produced by the sidered crucial for potentially increasing the
ACSQHC to outline the Scheme’s likely finan- engagement of health professionals and board
cial consequences.31 The methodology used was members in safety and quality improvement
based on programme budgeting and marginal activities. Additionally, at the health services
analysis guidelines.33 The report concluded that level, the NSQHS Standards provide an explicit
an initial investment of approximately AU$1 framework that directs organizations to
million was required by accreditation agencies improve their systems for understanding and
to initialize the Scheme.31 Financial impacts on addressing patient safety and quality issues.
government regulators, health services and Institutions can use the NSQHS Standards to
other stakeholders were not specified. engage health-care professionals and coordi-
nate their actions in improvement activities
Policy finalization and initial implementation: directed at high-quality patient care.
2011–2013
If you have a look at the 10 National Standards,
The NSQHS Standards were approved by the at one end they’ve got governance. At the other
Australian Health Ministers’ Council in Sep- end, they’ve got the management of pressure
tember 2011. In the ensuing year, regulatory ulcers and you think, ‘well, that seems really
mechanisms and surveying processes necessary weird.’ But we know pressure ulceration is man-
to effectively apply the Standards were final- aged badly, okay. We know governance is very,
very variable. So by putting some National Stan-
ized. The Private Hospital Sector Committee,
dards together, we say, ‘well, we’re going to lift
ACSQHC Board, Inter-Jurisdictional Commit- those two things. (Quality improvement agency
tee, Regulators Working Group and Accredi- representative, Focus group #13)
ting Agencies Working Group were key forums
through which operational details were negoti- At the health system level, participants pro-
posed that the NSQHS Standards provided,
ated and decided. The Scheme was introduced
for the first time, a clearly evidenced-based,
on 1 January 2013 and is now compulsory for
coherent and integrated national framework.
all public and private hospitals and day-
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Analysing health policy reform mechanisms, D Greenfield et al. 3117
The Scheme separated and clarified responsibil- At the health service level, an identified chal-
ity for different actors for accreditation stan- lenge was reliably assessing the compliance of
dards development, surveying processes and individual institutions with clinical performance
decisions, and regulation and policy matters. measures and their continuous quality improve-
As a result, the Scheme standardizes expecta- ment of organizational systems and processes.
tions, integrates roles and responsibilities, and Several stakeholders argued that there is
promotes transparency at all levels. insufficient focus on promoting on-going
improvements within the NSQHS Standards.
I think people will be held accountable much
more easily. . . a much clearer level of account- Countering this view somewhat, other partici-
ability across the system that didn’t previously pants suggested that as has occurred in respect
exist. . . it isn’t just the hospital’s fault or the to other prominent Australian health-care
CEO’s fault or you can’t just blame the accredi- accreditation programmes, future iterations are
ting agency because the system failed. You know, likely to shift greater emphasis towards this
the regulator’s got a role in this and they can’t
requirement. Also, concerns were raised by
adjust it. So each party’s role is much clearer. . .
It’s about making sure that the relationships and participants that focusing solely on the new
the framework gives everybody a buy in to hav- standards would come at the expense of other
ing. . . an unambiguous role. (Senior manager, organization process and initiatives.
healthcare professional representative organisa-
tion, Interview #15) . . . the 10 National Standards is great, but I
would hate to think that we lose sight of all the
non-clinical stuff that actually supports the clini-
cians to do what they’re doing. (Healthcare pro-
Current and future implementation challenges fessional, Focus group #7)
In addition to the significant potential benefits In particular, two potential risks to the cred-
identified, participants noted challenges that ibility of and satisfaction with the Scheme at
could, or may already, be impeding the imple- the health system level were raised. That is,
mentation of the Scheme. At the individual first, the application of the NSQHS Standards
level, stakeholders emphasized the difficulty of across settings and the second risk is the reli-
developing and maintaining consistent expecta- ability of assessments by different accrediting
tions amongst frontline clinicians regarding the agencies. The application of the NSQHS Stan-
aims and requirements of the reform. Corrobo- dards across settings was discussed as a point
rating this assertion, participating stakeholders of credibility. That the same expectations
often voiced confusion concerning key aspects would be applied to different health services, in
of the Scheme. different settings, was considered vital to con-
I actually think it’s a very confused area of pol- tinued engagement with the Scheme. That the
icy making. And the classic for me is that it ACSQHC would continue to maintain strong
depends on whether it’s driven by politicians, dri- expectations for high performance against
ven by the bureaucracy or driven by the industry. the NSQHS Standards was yet to be tested.
Driven by the bureaucracy, as we’re seeing with
The issue was particularly stressed in regard to
the NSQHS Standards from the Commission, it’s
– the program, to me, has been developed with- the NSQHS Standard focused on promoting
out proper thought being given to what are the consumer engagement in health care.
consequences of this program and how will that
. . . there are going to be a few shocks because
be managed? So now we’ve got a program that’s
where they [health services] meet accreditation
been launched which has got potentially very sig-
easily now. . . they may not meet it quite so easily
nificant political consequences and people are
with the Standards because the Standards are
now not sure how that’s going to be managed.
much more prescriptive. (Government policy rep-
(Accreditation agency management representa-
resentative, Focus group #17)
tive, Focus group #27)
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
3118 Analysing health policy reform mechanisms, D Greenfield et al.
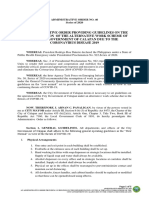
Similarly, satisfaction with the Scheme was Strategies to facilitate implementation
perceived to rest upon the reliability of assess-
Four strategies to facilitate implementation, to
ments, within and across accrediting agencies.
reinforce the potential benefits and to over-
The need for mechanisms to ensure consistent
come the substantial challenges facing the
surveying methods and outcomes across diverse
Scheme emerged and are presented in Fig. 1
accreditation agencies was discussed. Partici-
and discussed below. Participant’s explanations
pants maintained that inconsistency, that is,
revealed them to be inter-related and to inform
low inter-rater reliability,34 was highly likely,
one another.
and this could undermine the Scheme’s credi-
Regular and diverse ACSQHC consultation
bility. There was debate about whether the
activities were seen to facilitate implementation
government agencies had taken sufficient
by providing a platform for knowledge transfer,
actions to ensure survey reliability. It was
encouraging widespread stakeholder engage-
noted that the regulator of the system, the
ment. Aligned to this issue was the necessity for
ACSQHC, was aware of, and was developing
the forthcoming governmental educative activi-
training activities for accreditation agencies to
ties and materials to assist health services’
address, this issue. Some participants perceived
understanding of the Scheme. Participants
the Scheme to be flawed as these activities were
emphasized the importance of disseminating
not in place prior to commencing the use of
educative materials that are both informative
the NSQHS Standards.
and easily accessible to different stakeholders.
One of the challenges we talked about earlier
The devil is in the detail and it [effective imple-
was the limited, if any, training that current
mentation] will depend on how clear the guides
surveyors have had in relation to surveying
that support the Standards are, and the decision-
against the [NSQHS) Standards. (Healthcare
making tools which decide whether or not you
professional representative organisation, Focus
meet that Standard. (Healthcare professional,
group #16)
Focus group #2)
Consultation activities
Outcome data used to
inform Scheme
Educational activities
operations and ongoing
and materials
quality improvement
actions of health services
Consistent administration
of, and ongoing review
and improvements to
promote reliability and
accountability Figure 1 Strategies facilitating
implementation.
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Analysing health policy reform mechanisms, D Greenfield et al. 3119
The consistent administration of, on-going implementation of systems-level reforms.4 Study
review, and improvements to the Scheme were participants noted that this complexity may pre-
together identified as a further implementation vent the Scheme from achieving its goals.
strategy. The transparent and critical evaluation To respond to this challenging environment,
of accreditation agencies’ survey methods and the responsible agency for implementing the
decisions was commonly argued as necessary to Scheme undertook extensive consultation activ-
justify and maintain the Scheme’s ethos of pro- ities. The findings indicate that their aim was
moting greater regulatory accountability. The to determine appropriate methods of utilizing
Regulators Working Group and Accrediting existing government legislative powers to sup-
Agencies Working Group were seen to have port the reform, align the views and actions of
important roles in this regard. Furthermore, diverse groups and foster distributed leadership
participants considered it necessary for accredi- over the reform.36 The perceived importance of
tation outcome data, indicating health service these activities for maximizing the chance of
deficiencies and malpractices, to be systemati- achieving positive outcomes reinforces the fun-
cally processed by regulators, with consequences damental role of continued stakeholder engage-
enforced. To achieve this, the importance of ment as a necessary facilitator of national
leveraging government legislative powers, at accreditation reform. The importance of effec-
state and federal levels, was emphasized. tive stakeholder engagement has also been
identified in relation to other systems-level
health-care reforms internationally.37–40
Discussion
The study highlights three elements of
The AHSSQA Scheme is characteristic of the effective stakeholder engagement that can
increasing global trend towards government-led facilitate the development and implementation
accreditation reforms aiming to address con- of national accreditation reforms. First, the
sumer and health stakeholders’ demands for establishment of concrete mechanisms, such as
improved safety and quality in health care.8 government-convened committees, which enable
Likely benefits arising from the Scheme are regular, open and transparent communication
anticipated to be realized at multiple levels of flows between different stakeholders. Second,
the Australian health system, from potentially the credibility of government agencies dissemi-
increasing the involvement of professionals in nating reform-related information is paramount
quality improvement activities to providing a and can be promoted by authentic consultation
nationally consistent framework specifying practices. Third, while the aims and require-
safety and quality measures and requirements. ments of reforms should be conceptually unified,
The perceived benefits stakeholders identified the formats and language used to disseminate
illustrate the potential value of such reforms policy information should be strategically
and the key role of accreditation programmes designed to appeal to the varied normative prac-
in supporting improved quality and safety in tices of different stakeholders. Targeting of these
health care. This is the positive view of stake- three elements may allow agencies responsible
holders embedded within a system that has a for implementing national accreditation reforms
long history with accreditation in health care. to harness stakeholder engagement more effec-
However, the Scheme will be enacted within the tively as a critical facilitator.
complex adaptive system of health care,35 While such activities characterized the design
dynamically modified in response to multifari- and implementation of the Scheme, there is no
ous and interlinked institutions, groups and guarantee that it will realize the sum of its
structural arrangements that can hinder or facil- intended benefits. This view was stressed by a
itate implementation. International experience limited number of participants who remained
shows the inherent complexity of health care, sceptical of its value. National accreditation
regardless of country, is an impediment to programmes in other settings have produced
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
3120 Analysing health policy reform mechanisms, D Greenfield et al.
variable results,10,14,16 and standards-based funding scheme (project number LP100200586),
measurement and reporting systems are prone and a National Health and Medical Research
to unanticipated consequences.41 To empiri- Council Program Grant (project number
cally evaluate the health system and patient 568612).
outcomes resulting from the Scheme, high-
quality formative and summative evaluation
Competing interests
studies are necessary. Longitudinal study
designs should be able to detect effects at mul- Margaret Banks is a Senior Program Director
tiple health system levels, for example individ- at the Australian Commission on Safety and
ual, organizational and system changes over Quality in Health Care, and is centrally
time, to address issues of sustainability. involved in the implementation of the Austra-
Regarding study limitations, despite the large lian Health Service Safety and Quality Accredi-
numbers of participants, the interview samples tation Scheme. The other authors declare that
were not randomized or statistically representa- they have no competing interests.
tive. Furthermore, while rigorous methods were
used to codify the views of a diverse, nationwide
References
range of health-care stakeholders and profes-
sionals, these remain participants’ perceptions 1 Øvretveit J, Tolf S. The Costs of Poor Quality and
rather than objective information regarding the Adverse Events in Health Care - A Review of
AHSSQA Scheme’s development and imple- Research for the Swedish Healthcare Compensation
Insurance Company (Landstingens Omsesidiga
mentation. Mitigating these limitations, the tri-
Forsakringsbolag (LoF)). Stockholm: The Medical
angulated design helped illuminate multiple Management Centre, The Karolinska Institutet,
perspectives and converged on a common view. 2009.
2 Jha AK, Prasopa-Plaizier N, Larizgoitia I, Bates DW.
Patient safety research: an overview of the global
Conclusions evidence. Quality and Safety in Health Care, 2010; 19:
42–47.
Governments are increasingly undertaking 3 Braithwaite J, Coiera E. Beyond patient safety
national accreditation reforms to improve the Flatland. Journal of the Royal Society of Medicine,
safety and quality of health care. While engen- 2010; 2010: 219–225.
dering significant stakeholder support, diverse 4 Benn J, Burnett S, Parand A, Pinto A, Iskander S,
and complex implementation challenges must Vincent C. Studying large-scale programmes to
improve patient safety in whole care systems:
be overcome to obtain the considerable poten-
challenges for research. Social Science & Medicine,
tial benefits. Drawing on Australia’s recent 2009; 69: 1767–1776.
experience in developing and implementing the 5 Millenson ML. Pushing the profession: how the
AHSSQA Scheme, important facilitation mech- news media turned patient safety into a priority.
anisms identified in this study, including key Quality and Safety in Health Care, 2002; 11: 57–63.
6 Palmer C, Murcott T. All news is bad news: patient
components of effective stakeholder engage-
safety in the news media. In: Rowley E, Waring J
ment, can inform strategic planning for similar (eds) A Socio-cultural Perspective on Patient Safety.
reforms internationally. Burlington, VT: Ashgate, 2011: 13–28.
7 Small SD, Barach P. Patient safety and health
policy: a history and review. Hematology/oncology
Acknowledgements Clinics of North America, 2002; 16: 1463–1482.
8 Touati N, Pomey MP. Accreditation at a
None.
crossroads: are we on the right track? Health Policy,
2009; 90: 156–165.
9 Braithwaite J, Westbrook J, Pawsey M et al. A
Funding
prospective, multi-method, multi-disciplinary, multi-
The research was supported under the Austra- level, collaborative, social-organisational design for
lian Research Council’s Linkage Projects
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Analysing health policy reform mechanisms, D Greenfield et al. 3121
researching health sector accreditation [LP0560737]. 22 Øvretveit J. The contribution of new social science
BMC Health Services Research, 2006; 6: 113–123. research to patient safety. Social Science &
10 Greenfield D, Braithwaite J. Health sector Medicine, 2009; 69: 1780–1783.
accreditation research: a systematic review. 23 Greenfield D, Pawsey M, Naylor J, Braithwaite J.
International Journal for Quality in Health Care, Are accreditation surveys reliable? International
2008; 20: 172–183. Journal of Health Care Quality Assurance, 2009; 22:
11 Australian Commission on Safety and Quality in 105–116.
Health Care (ACSQHC). Discussion Paper: National 24 Hinchcliff R, Greenfield D, Braithwaite J. Is it
Safety and Quality Accreditation Standards. Sydney, worth engaging in multi-stakeholder health services
NSW: ACSQHC, 2006. research collaborations? Reflections on key benefits,
12 Australian Commission on Safety and Quality in challenges and enabling mechanisms. International
Health Care (ACSQHC). Hospitals: Core and Journal for Quality in Health Care, 2014;
Developmental Actions: National Safety and Quality 26: 124–128.
Health Service Standards. Sydney, NSW: ACSQHC, 25 International. Q. NVivo9: QSR International.
2013. Available from: Available at: http://www.
13 Australian Commission on Safety and Quality in qsrinternational.com/products_nvivo.aspx, accessed
Health Care (ACSQHC). National Safety and 8 September 2011.
Quality Health Service Standards. Sydney, NSW: 26 Kitzinger J. Qualitative research: introducing
Commonwealth of Australia, 2011. focus groups. British Medical Journal, 1995; 311:
14 Hinchcliff R, Greenfield D, Westbrook J et al. 299–302.
Narrative synthesis of health service accreditation 27 Australian Council for Safety and Quality in Health
literature. BMJ Quality and Safety, 2012; 21: Care (ACSQHC). Standards Setting and
979–991. Accreditation Literature Review and Report.
15 Greenfield D, Pawsey M, Hinchcliff R, Moldovan M, Canberra, ACT: ACSQHC, 2003.
Braithwaite J. The standard of healthcare 28 Australian Council for Safety and Quality in Health
accreditation standards: a review of empirical Care (ACSQHC). Standards Setting and
research underpinning their development and Accreditation Systems in Health: Consultation Paper.
impact. BMC Health Services Research, 2012; Canberra, ACT: ACSQHC, 2003.
12: 329. 29 Australian Council for Safety and Quality in Health
16 Hinchcliff R, Boxall A, Partel K, Greenfield D, Care (ACSQHC). Standards Setting and
Braithwaite J. Accreditation of health services: is it Accreditation Systems in Health Consultation: A
money and time well spent? Health Policy Evidence Marketing Research Report. Canberra, ACT:
Brief, Deeble Institute for Health Policy Research, ACSQHC, 2003.
2013; 9: 1–8. 30 Paterson R, The Review Team for the Review of
17 Braithwaite J, Westbrook J, Johnston B et al. Future Governance Arrangements for Safety and
Strengthening organizational performance through Quality in Health Care. National Arrangements for
accreditation research: the ACCREDIT project. Safety and Quality of Health Care in Australia:
BMC Research Notes, 2011; 4: 390. The Report of the Review of Future Governance
18 Greenfield D, Hinchcliff R, Moldovan M et al. A Arrangements for Safety and Quality in Health Care.
multimethod research investigation of consumer Canberra, ACT: Australian Health Ministers’
involvement in Australian health service Conference, 2005.
accreditation programmes: the ACCREDIT-SCI 31 Australian Commission on Safety and Quality in
study protocol. BMJ Open, 2012; 2: e002024. Health Care (ACSQHC). National Safety and
19 Hinchcliff R, Greenfield D, Moldovan M et al. Quality Health Service Standards and Their Use in a
Evaluation of current Australian health service Model National Accreditation Scheme: Decision
accreditation processes (ACCREDIT-CAP): Regulatory Impact Statement. Sydney, NSW:
protocol for a mixed-method research project. BMJ ACSQHC, 2010.
Open, 2012; 2: e001726. 32 Australian Commission on Safety and Quality in
20 Mumford V, Greenfield D, Hinchcliff R et al. Health Care (ACSQHC). Development of the
Economic evaluation of Australian acute care National Safety and Quality Health Service
accreditation (ACCREDIT-CBA (Acute)): study Standards. ACSQHC, 2013 [13 May]. Available at:
protocol for a mixed-method research project. BMJ http://www.safetyandquality.gov.au/our-work/
Open, 2013; 3: e002381. accreditation/development-of-the-standards-
21 Liamputtong P. Qualitative Research Methods, 3rd and-model-national-accreditation-scheme/, Accessed
edn. Melbourne, Vic.: Oxford University Press, 13 May 2014.
2009.
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
13697625, 2015, 6, Downloaded from https://onlinelibrary.wiley.com/doi/10.1111/hex.12300 by EBMG ACCESS - ZIMBABWE, Wiley Online Library on [17/11/2023]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
3122 Analysing health policy reform mechanisms, D Greenfield et al.
33 Mitton C, Donaldson C. Priority Setting Toolkit: A 39 Hinchcliff R, Ivers RQ, Poulos R, Senserrick T.
Guide to the Use of Economics in Healthcare Utilization of research in policymaking for
Decision Making. London: BMJ Publishing Group, graduated driver licensing. American Journal of
2004. Public Health, 2010; 100: 2052–2058.
34 Greenfield D, Hinchcliff R, Westbrook M et al. An 40 Best A, Greenhalgh T, Lewis S, Saul JE, Carroll S,
empirical test of accreditation patient journey Bitz J. Large-system transformation in health care:
surveys: randomised trial. International Journal for a realist review. The Milbank Quarterly, 2012; 90:
Quality in Health Care, 2012; 24: 495–500. 421–456.
35 Braithwaite J, Clay-Williams R, Nugus P, Plumb J. 41 Mannion R, Braithwaite J. Unintended
Health care as a complex adaptive system. In: consequences of performance measurement in
Hollnagel E, Braithwaite J, Wears R (eds) Resilient healthcare: 20 salutary lessons from the English
Health Care. London: Ashgate, 2013: 57–73. National Health Service. Internal Medicine Journal,
36 Greenfield D, Braithwaite J, Pawsey M, Johnson B, 2012; 42: 569–574.
Robinson M. Distributed leadership to mobilise 42 Australian Commission on Safety and Quality in
capacity for accreditation research. Journal of Health Care (ACSQHC). Accreditation Outcome
Health Organisation and Management, 2009; 23: Results and Evidence of Implementation of the
255–267. National Safety and Quality Health Service
37 Weiner B. A theory of organizational readiness for (NSQHS) Standards. Sydney, Australia: ACSQHC,
change. Implementation Science, 2009; 4: 67. 2012.
38 Scott SD, Albrecht L, O’Leary K et al. Systematic
review of knowledge translation strategies in the
allied health professions. Implementation Science,
2012; 7: 70.
ª 2014 John Wiley & Sons Ltd
Health Expectations, 18, pp.3110–3122
You might also like
- Margaret McWilliams-Fundamentals of Meal ManagementDocument361 pagesMargaret McWilliams-Fundamentals of Meal ManagementSaher Yasin89% (9)
- Why Adopt ISO 9001 Certification in Hospitals? A Case Study of External Triggers and Sensemaking in An Emergency Department in NorwayDocument14 pagesWhy Adopt ISO 9001 Certification in Hospitals? A Case Study of External Triggers and Sensemaking in An Emergency Department in NorwayVishal PrajapatiNo ratings yet
- Icu QualityDocument10 pagesIcu Qualitymahbub alamNo ratings yet
- GSK Public Policy Brief - QualityDocument2 pagesGSK Public Policy Brief - QualityAnna HerreraNo ratings yet
- International Journal of Nursing SciencesDocument8 pagesInternational Journal of Nursing SciencesjihaanNo ratings yet
- Cg4 - Bmjopen 2014 006157Document7 pagesCg4 - Bmjopen 2014 006157Mihalache Dan StefanNo ratings yet
- Advantages and Disadvantages of Health Care AccredDocument32 pagesAdvantages and Disadvantages of Health Care Accredgiuliano moralesNo ratings yet
- Advances-Meyer 41 PDFDocument13 pagesAdvances-Meyer 41 PDFNenny Puji LestariNo ratings yet
- Value Based HealthcareDocument48 pagesValue Based HealthcareAsem Shadid100% (1)
- 248-Article Text-729-1-10-20200125Document12 pages248-Article Text-729-1-10-20200125InderawatiNo ratings yet
- JCI Whitepaper Cpgs Closing The GapDocument12 pagesJCI Whitepaper Cpgs Closing The GapMathilda UllyNo ratings yet
- Jurnal Quality ImprovementDocument10 pagesJurnal Quality ImprovementbeungsyifaNo ratings yet
- 119 FullDocument13 pages119 FullLaras FirdausNo ratings yet
- Issues in The Assessment of Continuous Quality Improvement Implementation in Health Care OrganizationsDocument11 pagesIssues in The Assessment of Continuous Quality Improvement Implementation in Health Care OrganizationsLinda AliNo ratings yet
- MX and Medico Legal AssignDocument14 pagesMX and Medico Legal AssignyeapgyNo ratings yet
- A Framework For Evaluating Health Promotion ProgramsDocument24 pagesA Framework For Evaluating Health Promotion ProgramsKarla Monique PadrelananNo ratings yet
- The Impact of ISO Certification of Healthcare ServicesDocument9 pagesThe Impact of ISO Certification of Healthcare ServicesMintesinotNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument7 pagesBest Practice & Research Clinical Obstetrics and GynaecologyEko TulusNo ratings yet
- Quality in EndosDocument27 pagesQuality in EndosServio CordovaNo ratings yet
- 10 1016@j Healthpol 2019 04 006Document5 pages10 1016@j Healthpol 2019 04 006djebedemariusNo ratings yet
- Lean and Six Sigma in Healthcare: Examining The Impact On Patient Safety and Quality of CareDocument17 pagesLean and Six Sigma in Healthcare: Examining The Impact On Patient Safety and Quality of Careejay einzNo ratings yet
- Patient Education and Counseling: Juliana Chen, Luke Gemming, Rhona Hanning, Margaret Allman-FarinelliDocument8 pagesPatient Education and Counseling: Juliana Chen, Luke Gemming, Rhona Hanning, Margaret Allman-FarinelliAlvaro PalominoNo ratings yet
- Macam-Macam GuidelineDocument17 pagesMacam-Macam GuidelineFrederickSuryaNo ratings yet
- AH RI Quality Improvement UASDocument5 pagesAH RI Quality Improvement UASSrikit NurkamidenNo ratings yet
- Lizarondo 2014 PerformanceEvalDocument13 pagesLizarondo 2014 PerformanceEvalKamila AmmarNo ratings yet
- ACGME Outcome ProjectDocument8 pagesACGME Outcome ProjectsrisetyaNo ratings yet
- Bmjopen 2014 005284Document8 pagesBmjopen 2014 005284Cesar GarciaNo ratings yet
- NSQHS StandardsDocument80 pagesNSQHS StandardsDwi Suranto100% (1)
- The Impact of Accreditation On The Quality of Australian Health ServicesDocument8 pagesThe Impact of Accreditation On The Quality of Australian Health Servicesdlwlgus1008No ratings yet
- Standard5 Oct 2012 WEBDocument31 pagesStandard5 Oct 2012 WEBlefgo1989No ratings yet
- QA PAFP Journal July December 59-2-2021 Pages 115 126Document12 pagesQA PAFP Journal July December 59-2-2021 Pages 115 126Norjetalexis Maningo CabreraNo ratings yet
- Continuous Quality Improvement and Accreditation - EditedDocument5 pagesContinuous Quality Improvement and Accreditation - EditedBandah Mwiti Joseph100% (1)
- Continuous Quality Improvement and Accreditation - EditedDocument5 pagesContinuous Quality Improvement and Accreditation - EditedBandah Mwiti JosephNo ratings yet
- J of Nursing Scholarship - 2019 - Flynn - Understanding Determinants of Sustainability Through A Realist Investigation of ADocument10 pagesJ of Nursing Scholarship - 2019 - Flynn - Understanding Determinants of Sustainability Through A Realist Investigation of APaulo LemeNo ratings yet
- NSQHS Standards Sept2011Document80 pagesNSQHS Standards Sept2011Poonam Anala YeldandiNo ratings yet
- 1 s2.0 S1521691811000539 MainDocument11 pages1 s2.0 S1521691811000539 Mainnunki aprillitaNo ratings yet
- Standard3 Oct 2012 WEBDocument63 pagesStandard3 Oct 2012 WEBAA BBNo ratings yet
- Module 5 Publication Review ArticleDocument12 pagesModule 5 Publication Review ArticleomaNo ratings yet
- C11 - Basics of Quality in HSDocument6 pagesC11 - Basics of Quality in HSCoordinacion aNo ratings yet
- Narrow Health Cares Quality PDFDocument8 pagesNarrow Health Cares Quality PDFakram75zaaraNo ratings yet
- ISQua Webinar - Nick Sevdalis - September 2017Document39 pagesISQua Webinar - Nick Sevdalis - September 2017utari dewiNo ratings yet
- 2020 Model and Process For Nutrition and Dietetic Practice 1Document20 pages2020 Model and Process For Nutrition and Dietetic Practice 1Saba TanveerNo ratings yet
- OM AssignmentDocument18 pagesOM AssignmentYoosuf Mohamed IrsathNo ratings yet
- s6 Clinical HandoverDocument26 pagess6 Clinical HandoverirenediahjNo ratings yet
- E94296 PDFDocument54 pagesE94296 PDFowusuesselNo ratings yet
- Analysis: Adapting Lean Methods To Facilitate Stakeholder Engagement and Co-Design in HealthcareDocument4 pagesAnalysis: Adapting Lean Methods To Facilitate Stakeholder Engagement and Co-Design in HealthcareGuillermo Luis AcostaNo ratings yet
- National Model Clinical Governance FrameworkDocument44 pagesNational Model Clinical Governance Frameworkwenhal100% (1)
- Guide Developing and Assessing A Quality PlanDocument50 pagesGuide Developing and Assessing A Quality PlanesamNo ratings yet
- Interventions To Drive Uptake of VoluntaDocument6 pagesInterventions To Drive Uptake of VoluntaMalkit SinghNo ratings yet
- NABH 5th EDITION REPORTDocument58 pagesNABH 5th EDITION REPORTbrajeshb.railwayNo ratings yet
- Person-Centred Value-Based Health CareDocument58 pagesPerson-Centred Value-Based Health CarercabaNo ratings yet
- Clinical Governance ArticleDocument9 pagesClinical Governance ArticleJonathanNgNo ratings yet
- 2020 - Quality Improvement Into PracticeDocument6 pages2020 - Quality Improvement Into PracticeMORADOMIANo ratings yet
- FinalDocument8 pagesFinalxcgfxgvxNo ratings yet
- DI Virtual Health AcceleratedDocument20 pagesDI Virtual Health Acceleratedchetan NNo ratings yet
- Idea To Impact - Jan 2015 508 PDFDocument80 pagesIdea To Impact - Jan 2015 508 PDFAprilya LestariNo ratings yet
- Accreditation and ISO Certification DoDocument7 pagesAccreditation and ISO Certification DoMintesinotNo ratings yet
- Licensure Accreditation and CertificationDocument63 pagesLicensure Accreditation and Certificationradomir.boskovicNo ratings yet
- 2019 - Health Service Accreditation Stimulating Change in Clinical Care and Human Resource Management Processes A Study of 311 Australian HospitalsDocument19 pages2019 - Health Service Accreditation Stimulating Change in Clinical Care and Human Resource Management Processes A Study of 311 Australian Hospitalsirma firnandarNo ratings yet
- Develop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenDocument8 pagesDevelop Med Child Neuro - 2021 - Ogourtsova - Patient Engagement in An Online Coaching Intervention For Parents of ChildrenpsicoterapiavaldiviaNo ratings yet
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- Colorectal CancerDocument23 pagesColorectal Cancerralph_gail100% (1)
- Hyperemesis Gravidarum ProtocolDocument6 pagesHyperemesis Gravidarum ProtocolArumDesiPratiwi0% (1)
- Personalized Medicine of Monoclonal Antibodies in in Ammatory Bowel Disease: Pharmacogenetics, Therapeutic Drug Monitoring, and BeyondDocument15 pagesPersonalized Medicine of Monoclonal Antibodies in in Ammatory Bowel Disease: Pharmacogenetics, Therapeutic Drug Monitoring, and BeyondJessica Asitimbay ZuritaNo ratings yet
- Essentials For The Medical ImagingDocument2 pagesEssentials For The Medical ImagingscepanNo ratings yet
- CSB BookletDocument36 pagesCSB BookletHitesh Parmar100% (2)
- Scrub Suit BrochureDocument9 pagesScrub Suit Brochurehendra cahyaditaNo ratings yet
- Short Essay 5Document2 pagesShort Essay 5api-550568986No ratings yet
- English For Hospital StaffDocument6 pagesEnglish For Hospital StaffВолодимир ТатарінNo ratings yet
- Academic Essay For Brighton University.Document4 pagesAcademic Essay For Brighton University.omelle AbubakarNo ratings yet
- Which Career Pathway Is Right For You?Document6 pagesWhich Career Pathway Is Right For You?Kinelyn BaguioNo ratings yet
- Correlation Between Pregnancy Outcome and PlacentalDocument5 pagesCorrelation Between Pregnancy Outcome and PlacentalnskhldNo ratings yet
- Jurnal HipertiroidDocument6 pagesJurnal HipertiroidUmmulAklaNo ratings yet
- 1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeDocument15 pages1.pfizer Documents Reveal at Least 800 People Never Finished The COVID Vaccine Trial Due To Death, Injury or Withdrawn Consent - The ExposeElvaNo ratings yet
- Psychosis: Is It A Medical Problem?: Dowden Health MediaDocument6 pagesPsychosis: Is It A Medical Problem?: Dowden Health MediaJagdishVankarNo ratings yet
- Acute and Chronic WoundDocument69 pagesAcute and Chronic Woundaufar isytaharNo ratings yet
- Q2 PPT HEALTH9 Lesson 1 Drug Scenario in The PhilippinesDocument38 pagesQ2 PPT HEALTH9 Lesson 1 Drug Scenario in The PhilippinesKobie Loraine Ponio100% (2)
- BOSH D1 FinalDocument189 pagesBOSH D1 Finaljoe GregNo ratings yet
- Fit Over 40 Free ChapterDocument24 pagesFit Over 40 Free Chapterheather_581065043100% (1)
- Acker Lawrence 2009 Social Work and Managed Care Measuring Competence Burnout and Role Stress of Workers ProvidingDocument15 pagesAcker Lawrence 2009 Social Work and Managed Care Measuring Competence Burnout and Role Stress of Workers ProvidingLina Marcela Rincón BarónNo ratings yet
- Myanmar IBBS and Population Size Estimates Among PWID 2017-2018Document68 pagesMyanmar IBBS and Population Size Estimates Among PWID 2017-2018Murali ShunmugamNo ratings yet
- AO New Normal FinalDocument5 pagesAO New Normal FinalTumasitoe Bautista LasquiteNo ratings yet
- Theoretical Approaches To Multicultural Positive Psychological I 2019 PDFDocument549 pagesTheoretical Approaches To Multicultural Positive Psychological I 2019 PDFBonifar Jr BarluadoNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka.: 4th ' T ' Block, Jayanagar, Banglore-560 041Document10 pagesRajiv Gandhi University of Health Sciences, Karnataka.: 4th ' T ' Block, Jayanagar, Banglore-560 041JubinNo ratings yet
- Abortion Preparation Checklist PDFDocument2 pagesAbortion Preparation Checklist PDFapi-535810682No ratings yet
- Ayuno Intermitente y Diabeticos 2Document10 pagesAyuno Intermitente y Diabeticos 2vicenteNo ratings yet
- Isd 110 TsesDocument23 pagesIsd 110 Tsesapi-372339051No ratings yet
- Guide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Document2 pagesGuide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Devs AbdouNo ratings yet
- Alcohol Withdrawal Care PlanDocument1 pageAlcohol Withdrawal Care PlanVanessaMUellerNo ratings yet
- Prabhat Shinde CVDocument2 pagesPrabhat Shinde CVranaware ajinkyaNo ratings yet