
URO 3 - Neoplasm in The Genitourinary Tract
URO 3 - Neoplasm in The Genitourinary Tract
You might also like
- NMAT Inductive Reasoning Module 6Document3 pagesNMAT Inductive Reasoning Module 6Ha Jae kyeong0% (1)
- SK FUND UTILIZATION ReportDocument1 pageSK FUND UTILIZATION ReportMary Grace Villacote100% (3)
- Oral Pathology Dent1411Document7 pagesOral Pathology Dent1411api-663458841No ratings yet
- Testicular TumorsDocument6 pagesTesticular Tumorsyoussef.aziz2020No ratings yet
- PancreasDocument7 pagesPancreasMiguel Cuevas DolotNo ratings yet
- Onco ImDocument2 pagesOnco ImAlexandra BascoNo ratings yet
- Gyne - Case 15 Benign Lesions of The Vulva & VaginaDocument2 pagesGyne - Case 15 Benign Lesions of The Vulva & Vaginacbac1990No ratings yet
- Appendiceal Neoplasms: Quinton M. Hatch, M.DDocument4 pagesAppendiceal Neoplasms: Quinton M. Hatch, M.DJorge Salazar AlarcónNo ratings yet
- Wilm's Tumour Nephroblastoma Renal Cell Ca Adenocarcima Grawitz's Carcioma of Urinary BladderDocument2 pagesWilm's Tumour Nephroblastoma Renal Cell Ca Adenocarcima Grawitz's Carcioma of Urinary BladderAhmed ALiNo ratings yet
- ActaDV 100 11 5753Document9 pagesActaDV 100 11 5753NandaNo ratings yet
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenDocument3 pagesRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahNo ratings yet
- OB - GYN Clerkship Charts - Google Drive PDFDocument1 pageOB - GYN Clerkship Charts - Google Drive PDFrpascua123No ratings yet
- Verrucous CarcinomaDocument20 pagesVerrucous CarcinomaOng Yanna MarieNo ratings yet
- PATH-REVISION. EXAM INFO docxDocument18 pagesPATH-REVISION. EXAM INFO docxDaniele TomassiNo ratings yet
- Oncologic Nursing PDFDocument4 pagesOncologic Nursing PDFDenesa Joyce BustamanteNo ratings yet
- C13. Vaginal, Vulvar & CervicalDocument4 pagesC13. Vaginal, Vulvar & Cervicalhari dharshanNo ratings yet
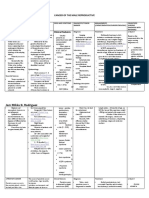
- Jam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Document12 pagesJam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Dinarkram Rabreca EculNo ratings yet
- Vulva CancerDocument2 pagesVulva CancerLim Hui ZhuanNo ratings yet
- Adult Desmoid Tumors: Biology, Management and Ongoing TrialsDocument7 pagesAdult Desmoid Tumors: Biology, Management and Ongoing TrialsGustavo GasperiNo ratings yet
- Squamous Cell Carcinoma of The Cervix With Cranial Metastasis A Case ReportDocument4 pagesSquamous Cell Carcinoma of The Cervix With Cranial Metastasis A Case ReportJonelle baloloyNo ratings yet
- Carcinoma Gall BladderDocument25 pagesCarcinoma Gall Bladderrajan kumarNo ratings yet
- Lungs Benign and MalignantDocument7 pagesLungs Benign and MalignantNestley TiongsonNo ratings yet
- Bab 123Document22 pagesBab 123Diamond Itoe IntanNo ratings yet
- Oncology Table SummaryDocument4 pagesOncology Table SummaryAiah AbenesNo ratings yet
- 151 Peripheral Lung Lesion Potential Pulmonary Adenocarcinoma Compatibility ModeDocument30 pages151 Peripheral Lung Lesion Potential Pulmonary Adenocarcinoma Compatibility ModeGordana PuzovicNo ratings yet
- Tumor MarkerDocument4 pagesTumor Markerkimmynemil80No ratings yet
- Didactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Document28 pagesDidactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Moritz SolivenNo ratings yet
- Bladder Oncology CanvasDocument40 pagesBladder Oncology CanvasNuha HamedNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Breast-SummaryDocument10 pagesBreast-SummarymohamedNo ratings yet
- Breast Cancer Didactics - ManzanoDocument49 pagesBreast Cancer Didactics - ManzanoJoy ManzanoNo ratings yet
- Subspec Urology: GU TumorsDocument5 pagesSubspec Urology: GU TumorsThakoon TtsNo ratings yet
- Primary Vaginal Invasive Squamous Cell Carcinoma A Rare Case Report 2157 7099 1000449Document3 pagesPrimary Vaginal Invasive Squamous Cell Carcinoma A Rare Case Report 2157 7099 1000449FaliyaaaNo ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- Finals ReviewerDocument35 pagesFinals Reviewerimlookingforyou.03No ratings yet
- Path Adrenal TumorDocument4 pagesPath Adrenal TumorRama HijaziNo ratings yet
- Oncology NursingDocument6 pagesOncology NursingreooooNo ratings yet
- ARROCase SalivaryGlandTumorsDocument61 pagesARROCase SalivaryGlandTumorssnolinNo ratings yet
- Neoplasia: Monoclonal Unregulated, and IrreversibleDocument10 pagesNeoplasia: Monoclonal Unregulated, and Irreversiblehippypsyduck mdNo ratings yet
- An Uncommon Cancer of Parotid Squamous Cell HistologyDocument3 pagesAn Uncommon Cancer of Parotid Squamous Cell HistologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bladder Cancer BasicsDocument1 pageBladder Cancer BasicsAziz KhalidNo ratings yet
- Screenshot 2023-03-01 at 3.14.03 PMDocument17 pagesScreenshot 2023-03-01 at 3.14.03 PMmohameeedar1No ratings yet
- 楊志仁 肺結核與腫瘤判讀Document109 pages楊志仁 肺結核與腫瘤判讀au angelNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- Prise en Charge Des Tumeurs Des Glandes Salivaires Royaume-Uni Lignes Directrices Nationales MultidisciplinairesDocument8 pagesPrise en Charge Des Tumeurs Des Glandes Salivaires Royaume-Uni Lignes Directrices Nationales MultidisciplinairesMamadou DIENENo ratings yet
- CNP - AjDocument33 pagesCNP - AjeviltohuntNo ratings yet
- 5.2 Renal Masses and Congenital AnomaliesDocument9 pages5.2 Renal Masses and Congenital AnomaliesMaria roxanne HernandezNo ratings yet
- Neoplasms of The ThyroidDocument5 pagesNeoplasms of The ThyroidMahmoud AbouelsoudNo ratings yet
- Week 16 Gi and Gyne CancerDocument15 pagesWeek 16 Gi and Gyne Cancerjmmacar19No ratings yet
- Management of Salivary Gland Tumours: United Kingdom National Multidisciplinary GuidelinesDocument8 pagesManagement of Salivary Gland Tumours: United Kingdom National Multidisciplinary GuidelinesCeriaindriasariNo ratings yet
- Testicular Cancer: Basic InformationDocument3 pagesTesticular Cancer: Basic InformationAnonymous eF8cmVvJaNo ratings yet
- Bladdercancerabeerfinal 170701110656Document94 pagesBladdercancerabeerfinal 170701110656Aravindh SharmaNo ratings yet
- Lung Ca Small Bx2 PDFDocument4 pagesLung Ca Small Bx2 PDFJose SirittNo ratings yet
- Tumor Markers Common Manifestations Therapy/Treatment Others: Male CancersDocument9 pagesTumor Markers Common Manifestations Therapy/Treatment Others: Male CancersErica DagdagNo ratings yet
- ONCOLOGYDocument26 pagesONCOLOGYShawn TejanoNo ratings yet
- Unusual Cases of Carcinoma of Palatine TonsilDocument5 pagesUnusual Cases of Carcinoma of Palatine TonsilPridho GaziansyahNo ratings yet
- Eau Guidelines On Penile Cancer: Introduction and EpidemiologyDocument15 pagesEau Guidelines On Penile Cancer: Introduction and Epidemiologyhypebeast dopeNo ratings yet
- A Cutaneous Horn On The Ear: ManagementDocument1 pageA Cutaneous Horn On The Ear: ManagementDylanNo ratings yet
- Gynecologic Oncology Reports: Benjamin L. Stueben, Jonathan F. LaraDocument2 pagesGynecologic Oncology Reports: Benjamin L. Stueben, Jonathan F. Lararg2fpgqnc8No ratings yet
- Omental RhabdoDocument4 pagesOmental RhabdoDaisuke KiritoNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- ENT Midterms Long QuizDocument4 pagesENT Midterms Long QuizHa Jae kyeongNo ratings yet
- Ent Midterm SamplexDocument84 pagesEnt Midterm SamplexHa Jae kyeongNo ratings yet
- Ent Samplex - TikitikiDocument25 pagesEnt Samplex - TikitikiHa Jae kyeongNo ratings yet
- Rehab FinalsDocument32 pagesRehab FinalsHa Jae kyeongNo ratings yet
- TCVS 2 Cardiac Surgery Dr. de AsisDocument6 pagesTCVS 2 Cardiac Surgery Dr. de AsisHa Jae kyeongNo ratings yet
- BILIARYDocument20 pagesBILIARYHa Jae kyeongNo ratings yet
- Administrative Order No. 55 S. 1988Document12 pagesAdministrative Order No. 55 S. 1988Ha Jae kyeongNo ratings yet
- Dr. Jesus C. Delgado Memorial Center: MissionDocument2 pagesDr. Jesus C. Delgado Memorial Center: MissionHa Jae kyeongNo ratings yet
- The Canterbury Tales and Pardoner's TaleDocument47 pagesThe Canterbury Tales and Pardoner's TaleHa Jae kyeongNo ratings yet
- Orange Fantasy MocktailDocument1 pageOrange Fantasy MocktailHa Jae kyeongNo ratings yet
- Partus & LactationDocument27 pagesPartus & LactationfrankyNo ratings yet
- Soluvit N PIDocument3 pagesSoluvit N PIsigitNo ratings yet
- Magnetic Resonance Imaging of The Breast: Recommendations From The EUSOMA Working GroupDocument21 pagesMagnetic Resonance Imaging of The Breast: Recommendations From The EUSOMA Working GroupNelly ChacónNo ratings yet
- Tumors of The KidneyDocument5 pagesTumors of The KidneyShivaniNo ratings yet
- Cap. 58) Intracerebral HemmorhageDocument10 pagesCap. 58) Intracerebral HemmorhageRobert DumaNo ratings yet
- A Rauf (Clinical Pathways) L.MDocument17 pagesA Rauf (Clinical Pathways) L.MShahab AlamNo ratings yet
- Đề Thi Sở Bình DươngDocument12 pagesĐề Thi Sở Bình DươngThảo PhạmNo ratings yet
- Han Dog 2017Document10 pagesHan Dog 2017ErtyWitalayaL.ToruanNo ratings yet
- 2005 Health Care Fraud RepotDocument46 pages2005 Health Care Fraud RepotMike DeWineNo ratings yet
- Nursing Procedure Checklist: Administering An Eye IrrigationDocument1 pageNursing Procedure Checklist: Administering An Eye IrrigationOrl Trinidad100% (1)
- Treatment and Management of Lumpy Skin Disease in Cow: A Case ReportDocument2 pagesTreatment and Management of Lumpy Skin Disease in Cow: A Case ReportjabidurNo ratings yet
- An Update On The Diagnosis and Treatment of LeprosyDocument10 pagesAn Update On The Diagnosis and Treatment of LeprosyChlarissa WahabNo ratings yet
- Executive Order BCDCDocument3 pagesExecutive Order BCDCjhanicesolimancentenoNo ratings yet
- FebuxostatDocument2 pagesFebuxostatJoshua Pascasio100% (1)
- 4 Badac Data Capture FormsDocument11 pages4 Badac Data Capture FormsKimberly AbayonNo ratings yet
- HACCP-meat and PoultryDocument19 pagesHACCP-meat and PoultryNGUYỄN HOÀNG LINHNo ratings yet
- Assessment and Management of Patients With Hematologic DisordersDocument124 pagesAssessment and Management of Patients With Hematologic DisordersAngelicaMarieRafananNo ratings yet
- National Programs Related To Child Health and WelfareDocument61 pagesNational Programs Related To Child Health and WelfareSujata Mishra100% (8)
- Posterior Tibialis Tendon Dysfunction (PTTD)Document11 pagesPosterior Tibialis Tendon Dysfunction (PTTD)bigpawn13No ratings yet
- Cure Diabetes in 3 WeeksDocument7 pagesCure Diabetes in 3 Weeksdmsint20078577100% (3)
- Health Insurance Portability in IndiaDocument2 pagesHealth Insurance Portability in IndiaJalaj PathakNo ratings yet
- Notice: Refusal of Vaccine For CauseDocument1 pageNotice: Refusal of Vaccine For CauseCatalin EnacheNo ratings yet
- Thesis of Agha Khan UniversityDocument40 pagesThesis of Agha Khan UniversityAHSAN ANSARINo ratings yet
- TIKOSYN Treatment GuidelinesDocument8 pagesTIKOSYN Treatment GuidelinesrbmartinivNo ratings yet
- MS Ii MT2Document11 pagesMS Ii MT2Rika MaeNo ratings yet
- Sales: $17,300.0M One Year Growth: 2.4%Document11 pagesSales: $17,300.0M One Year Growth: 2.4%lanezalNo ratings yet
- Catch Up Friday Session PlanDocument24 pagesCatch Up Friday Session Planwifetaehyung55No ratings yet
- Press Note - 19th Insurance Summit - Reimagining Insurance Bussiness - Insurance For All by 2047Document3 pagesPress Note - 19th Insurance Summit - Reimagining Insurance Bussiness - Insurance For All by 2047Vitesh KondalNo ratings yet
- Kerangka JJ HurrellDocument14 pagesKerangka JJ HurrellNur qamaliahNo ratings yet


































































































Download as pdf or txt
You might also like
- NMAT Inductive Reasoning Module 6Document3 pagesNMAT Inductive Reasoning Module 6Ha Jae kyeong0% (1)
- SK FUND UTILIZATION ReportDocument1 pageSK FUND UTILIZATION ReportMary Grace Villacote100% (3)
- Oral Pathology Dent1411Document7 pagesOral Pathology Dent1411api-663458841No ratings yet
- Testicular TumorsDocument6 pagesTesticular Tumorsyoussef.aziz2020No ratings yet
- PancreasDocument7 pagesPancreasMiguel Cuevas DolotNo ratings yet
- Onco ImDocument2 pagesOnco ImAlexandra BascoNo ratings yet
- Gyne - Case 15 Benign Lesions of The Vulva & VaginaDocument2 pagesGyne - Case 15 Benign Lesions of The Vulva & Vaginacbac1990No ratings yet
- Appendiceal Neoplasms: Quinton M. Hatch, M.DDocument4 pagesAppendiceal Neoplasms: Quinton M. Hatch, M.DJorge Salazar AlarcónNo ratings yet
- Wilm's Tumour Nephroblastoma Renal Cell Ca Adenocarcima Grawitz's Carcioma of Urinary BladderDocument2 pagesWilm's Tumour Nephroblastoma Renal Cell Ca Adenocarcima Grawitz's Carcioma of Urinary BladderAhmed ALiNo ratings yet
- ActaDV 100 11 5753Document9 pagesActaDV 100 11 5753NandaNo ratings yet
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenDocument3 pagesRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahNo ratings yet
- OB - GYN Clerkship Charts - Google Drive PDFDocument1 pageOB - GYN Clerkship Charts - Google Drive PDFrpascua123No ratings yet
- Verrucous CarcinomaDocument20 pagesVerrucous CarcinomaOng Yanna MarieNo ratings yet
- PATH-REVISION. EXAM INFO docxDocument18 pagesPATH-REVISION. EXAM INFO docxDaniele TomassiNo ratings yet
- Oncologic Nursing PDFDocument4 pagesOncologic Nursing PDFDenesa Joyce BustamanteNo ratings yet
- C13. Vaginal, Vulvar & CervicalDocument4 pagesC13. Vaginal, Vulvar & Cervicalhari dharshanNo ratings yet
- Jam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Document12 pagesJam Mikka G. Rodriguez (Cancer of The Male Reproductive 1)Dinarkram Rabreca EculNo ratings yet
- Vulva CancerDocument2 pagesVulva CancerLim Hui ZhuanNo ratings yet
- Adult Desmoid Tumors: Biology, Management and Ongoing TrialsDocument7 pagesAdult Desmoid Tumors: Biology, Management and Ongoing TrialsGustavo GasperiNo ratings yet
- Squamous Cell Carcinoma of The Cervix With Cranial Metastasis A Case ReportDocument4 pagesSquamous Cell Carcinoma of The Cervix With Cranial Metastasis A Case ReportJonelle baloloyNo ratings yet
- Carcinoma Gall BladderDocument25 pagesCarcinoma Gall Bladderrajan kumarNo ratings yet
- Lungs Benign and MalignantDocument7 pagesLungs Benign and MalignantNestley TiongsonNo ratings yet
- Bab 123Document22 pagesBab 123Diamond Itoe IntanNo ratings yet
- Oncology Table SummaryDocument4 pagesOncology Table SummaryAiah AbenesNo ratings yet
- 151 Peripheral Lung Lesion Potential Pulmonary Adenocarcinoma Compatibility ModeDocument30 pages151 Peripheral Lung Lesion Potential Pulmonary Adenocarcinoma Compatibility ModeGordana PuzovicNo ratings yet
- Tumor MarkerDocument4 pagesTumor Markerkimmynemil80No ratings yet
- Didactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Document28 pagesDidactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Moritz SolivenNo ratings yet
- Bladder Oncology CanvasDocument40 pagesBladder Oncology CanvasNuha HamedNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Breast-SummaryDocument10 pagesBreast-SummarymohamedNo ratings yet
- Breast Cancer Didactics - ManzanoDocument49 pagesBreast Cancer Didactics - ManzanoJoy ManzanoNo ratings yet
- Subspec Urology: GU TumorsDocument5 pagesSubspec Urology: GU TumorsThakoon TtsNo ratings yet
- Primary Vaginal Invasive Squamous Cell Carcinoma A Rare Case Report 2157 7099 1000449Document3 pagesPrimary Vaginal Invasive Squamous Cell Carcinoma A Rare Case Report 2157 7099 1000449FaliyaaaNo ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- Finals ReviewerDocument35 pagesFinals Reviewerimlookingforyou.03No ratings yet
- Path Adrenal TumorDocument4 pagesPath Adrenal TumorRama HijaziNo ratings yet
- Oncology NursingDocument6 pagesOncology NursingreooooNo ratings yet
- ARROCase SalivaryGlandTumorsDocument61 pagesARROCase SalivaryGlandTumorssnolinNo ratings yet
- Neoplasia: Monoclonal Unregulated, and IrreversibleDocument10 pagesNeoplasia: Monoclonal Unregulated, and Irreversiblehippypsyduck mdNo ratings yet
- An Uncommon Cancer of Parotid Squamous Cell HistologyDocument3 pagesAn Uncommon Cancer of Parotid Squamous Cell HistologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bladder Cancer BasicsDocument1 pageBladder Cancer BasicsAziz KhalidNo ratings yet
- Screenshot 2023-03-01 at 3.14.03 PMDocument17 pagesScreenshot 2023-03-01 at 3.14.03 PMmohameeedar1No ratings yet
- 楊志仁 肺結核與腫瘤判讀Document109 pages楊志仁 肺結核與腫瘤判讀au angelNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- Prise en Charge Des Tumeurs Des Glandes Salivaires Royaume-Uni Lignes Directrices Nationales MultidisciplinairesDocument8 pagesPrise en Charge Des Tumeurs Des Glandes Salivaires Royaume-Uni Lignes Directrices Nationales MultidisciplinairesMamadou DIENENo ratings yet
- CNP - AjDocument33 pagesCNP - AjeviltohuntNo ratings yet
- 5.2 Renal Masses and Congenital AnomaliesDocument9 pages5.2 Renal Masses and Congenital AnomaliesMaria roxanne HernandezNo ratings yet
- Neoplasms of The ThyroidDocument5 pagesNeoplasms of The ThyroidMahmoud AbouelsoudNo ratings yet
- Week 16 Gi and Gyne CancerDocument15 pagesWeek 16 Gi and Gyne Cancerjmmacar19No ratings yet
- Management of Salivary Gland Tumours: United Kingdom National Multidisciplinary GuidelinesDocument8 pagesManagement of Salivary Gland Tumours: United Kingdom National Multidisciplinary GuidelinesCeriaindriasariNo ratings yet
- Testicular Cancer: Basic InformationDocument3 pagesTesticular Cancer: Basic InformationAnonymous eF8cmVvJaNo ratings yet
- Bladdercancerabeerfinal 170701110656Document94 pagesBladdercancerabeerfinal 170701110656Aravindh SharmaNo ratings yet
- Lung Ca Small Bx2 PDFDocument4 pagesLung Ca Small Bx2 PDFJose SirittNo ratings yet
- Tumor Markers Common Manifestations Therapy/Treatment Others: Male CancersDocument9 pagesTumor Markers Common Manifestations Therapy/Treatment Others: Male CancersErica DagdagNo ratings yet
- ONCOLOGYDocument26 pagesONCOLOGYShawn TejanoNo ratings yet
- Unusual Cases of Carcinoma of Palatine TonsilDocument5 pagesUnusual Cases of Carcinoma of Palatine TonsilPridho GaziansyahNo ratings yet
- Eau Guidelines On Penile Cancer: Introduction and EpidemiologyDocument15 pagesEau Guidelines On Penile Cancer: Introduction and Epidemiologyhypebeast dopeNo ratings yet
- A Cutaneous Horn On The Ear: ManagementDocument1 pageA Cutaneous Horn On The Ear: ManagementDylanNo ratings yet
- Gynecologic Oncology Reports: Benjamin L. Stueben, Jonathan F. LaraDocument2 pagesGynecologic Oncology Reports: Benjamin L. Stueben, Jonathan F. Lararg2fpgqnc8No ratings yet
- Omental RhabdoDocument4 pagesOmental RhabdoDaisuke KiritoNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- ENT Midterms Long QuizDocument4 pagesENT Midterms Long QuizHa Jae kyeongNo ratings yet
- Ent Midterm SamplexDocument84 pagesEnt Midterm SamplexHa Jae kyeongNo ratings yet
- Ent Samplex - TikitikiDocument25 pagesEnt Samplex - TikitikiHa Jae kyeongNo ratings yet
- Rehab FinalsDocument32 pagesRehab FinalsHa Jae kyeongNo ratings yet
- TCVS 2 Cardiac Surgery Dr. de AsisDocument6 pagesTCVS 2 Cardiac Surgery Dr. de AsisHa Jae kyeongNo ratings yet
- BILIARYDocument20 pagesBILIARYHa Jae kyeongNo ratings yet
- Administrative Order No. 55 S. 1988Document12 pagesAdministrative Order No. 55 S. 1988Ha Jae kyeongNo ratings yet
- Dr. Jesus C. Delgado Memorial Center: MissionDocument2 pagesDr. Jesus C. Delgado Memorial Center: MissionHa Jae kyeongNo ratings yet
- The Canterbury Tales and Pardoner's TaleDocument47 pagesThe Canterbury Tales and Pardoner's TaleHa Jae kyeongNo ratings yet
- Orange Fantasy MocktailDocument1 pageOrange Fantasy MocktailHa Jae kyeongNo ratings yet
- Partus & LactationDocument27 pagesPartus & LactationfrankyNo ratings yet
- Soluvit N PIDocument3 pagesSoluvit N PIsigitNo ratings yet
- Magnetic Resonance Imaging of The Breast: Recommendations From The EUSOMA Working GroupDocument21 pagesMagnetic Resonance Imaging of The Breast: Recommendations From The EUSOMA Working GroupNelly ChacónNo ratings yet
- Tumors of The KidneyDocument5 pagesTumors of The KidneyShivaniNo ratings yet
- Cap. 58) Intracerebral HemmorhageDocument10 pagesCap. 58) Intracerebral HemmorhageRobert DumaNo ratings yet
- A Rauf (Clinical Pathways) L.MDocument17 pagesA Rauf (Clinical Pathways) L.MShahab AlamNo ratings yet
- Đề Thi Sở Bình DươngDocument12 pagesĐề Thi Sở Bình DươngThảo PhạmNo ratings yet
- Han Dog 2017Document10 pagesHan Dog 2017ErtyWitalayaL.ToruanNo ratings yet
- 2005 Health Care Fraud RepotDocument46 pages2005 Health Care Fraud RepotMike DeWineNo ratings yet
- Nursing Procedure Checklist: Administering An Eye IrrigationDocument1 pageNursing Procedure Checklist: Administering An Eye IrrigationOrl Trinidad100% (1)
- Treatment and Management of Lumpy Skin Disease in Cow: A Case ReportDocument2 pagesTreatment and Management of Lumpy Skin Disease in Cow: A Case ReportjabidurNo ratings yet
- An Update On The Diagnosis and Treatment of LeprosyDocument10 pagesAn Update On The Diagnosis and Treatment of LeprosyChlarissa WahabNo ratings yet
- Executive Order BCDCDocument3 pagesExecutive Order BCDCjhanicesolimancentenoNo ratings yet
- FebuxostatDocument2 pagesFebuxostatJoshua Pascasio100% (1)
- 4 Badac Data Capture FormsDocument11 pages4 Badac Data Capture FormsKimberly AbayonNo ratings yet
- HACCP-meat and PoultryDocument19 pagesHACCP-meat and PoultryNGUYỄN HOÀNG LINHNo ratings yet
- Assessment and Management of Patients With Hematologic DisordersDocument124 pagesAssessment and Management of Patients With Hematologic DisordersAngelicaMarieRafananNo ratings yet
- National Programs Related To Child Health and WelfareDocument61 pagesNational Programs Related To Child Health and WelfareSujata Mishra100% (8)
- Posterior Tibialis Tendon Dysfunction (PTTD)Document11 pagesPosterior Tibialis Tendon Dysfunction (PTTD)bigpawn13No ratings yet
- Cure Diabetes in 3 WeeksDocument7 pagesCure Diabetes in 3 Weeksdmsint20078577100% (3)
- Health Insurance Portability in IndiaDocument2 pagesHealth Insurance Portability in IndiaJalaj PathakNo ratings yet
- Notice: Refusal of Vaccine For CauseDocument1 pageNotice: Refusal of Vaccine For CauseCatalin EnacheNo ratings yet
- Thesis of Agha Khan UniversityDocument40 pagesThesis of Agha Khan UniversityAHSAN ANSARINo ratings yet
- TIKOSYN Treatment GuidelinesDocument8 pagesTIKOSYN Treatment GuidelinesrbmartinivNo ratings yet
- MS Ii MT2Document11 pagesMS Ii MT2Rika MaeNo ratings yet
- Sales: $17,300.0M One Year Growth: 2.4%Document11 pagesSales: $17,300.0M One Year Growth: 2.4%lanezalNo ratings yet
- Catch Up Friday Session PlanDocument24 pagesCatch Up Friday Session Planwifetaehyung55No ratings yet
- Press Note - 19th Insurance Summit - Reimagining Insurance Bussiness - Insurance For All by 2047Document3 pagesPress Note - 19th Insurance Summit - Reimagining Insurance Bussiness - Insurance For All by 2047Vitesh KondalNo ratings yet
- Kerangka JJ HurrellDocument14 pagesKerangka JJ HurrellNur qamaliahNo ratings yet