Download as pdf or txt
You might also like
- Gestational Diabetes Research PaperDocument16 pagesGestational Diabetes Research Paperapi-251486092No ratings yet
- Stress Reading Task Reading Comprehension Exercises 105292 2Document2 pagesStress Reading Task Reading Comprehension Exercises 105292 2Ana Isaac Rodas OrtizNo ratings yet
- Yaacob 2019Document10 pagesYaacob 2019TikaZyka16No ratings yet
- The Prevalence of Diabetes Mellitus Among Children in Lusaka Zambia, 2009-2019 A Hospital-Based StudyDocument7 pagesThe Prevalence of Diabetes Mellitus Among Children in Lusaka Zambia, 2009-2019 A Hospital-Based StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pediatric Diabetes - 2018 - Candler - Treatment Adherence and BMI Reduction Are Key Predictors of HbA1c 1 Year AfterDocument7 pagesPediatric Diabetes - 2018 - Candler - Treatment Adherence and BMI Reduction Are Key Predictors of HbA1c 1 Year AfterPraska BalabanovaNo ratings yet
- Screening Diagnostics of Gestional Diabetes Mellitus and Its Prevention During Pandemic PeriodDocument11 pagesScreening Diagnostics of Gestional Diabetes Mellitus and Its Prevention During Pandemic PeriodCentral Asian StudiesNo ratings yet
- Hubungan Pengetahuan, Motivasi, Dan Sikap Dengan Kepatuhan Diet Pada Penderita DM Tipe 2Document9 pagesHubungan Pengetahuan, Motivasi, Dan Sikap Dengan Kepatuhan Diet Pada Penderita DM Tipe 2sokhib930No ratings yet
- Kelompok 8 - Diabetes Mellitus Dan Obesitas (1) .Id - enDocument23 pagesKelompok 8 - Diabetes Mellitus Dan Obesitas (1) .Id - enKinkin NindiNo ratings yet
- Animal Model For Gestational DiabetesDocument14 pagesAnimal Model For Gestational DiabetesAnushka DhandeNo ratings yet
- Serbis 2020Document23 pagesSerbis 2020Eleni KotanidouNo ratings yet
- 2181 2407 3 PBDocument18 pages2181 2407 3 PBFahrika Luthfi AfiqohNo ratings yet
- Jurnal JeumpaDocument7 pagesJurnal JeumpaJeumpa SyahranaNo ratings yet
- Spruijt Metz2014Document10 pagesSpruijt Metz2014indah puspitaNo ratings yet
- Macedo 2010 Risk Factors For Type Diabetes Mel PDFDocument7 pagesMacedo 2010 Risk Factors For Type Diabetes Mel PDFZayNo ratings yet
- Dafonseca 2017Document45 pagesDafonseca 2017visiniNo ratings yet
- Articulo de InvestigacionDocument8 pagesArticulo de Investigacionjai_santiago_rojasNo ratings yet
- Awareness of Diabetes Mellitus Among Public Attending The Primary Health Centres in MalaysiaDocument13 pagesAwareness of Diabetes Mellitus Among Public Attending The Primary Health Centres in Malaysiamaryam farrukhNo ratings yet
- Comparison of Surgical and Medical Therapy For Type 2 Diabetes in Severely Obese AdolescentsDocument9 pagesComparison of Surgical and Medical Therapy For Type 2 Diabetes in Severely Obese AdolescentsMahesa Kurnianti PutriNo ratings yet
- The Effect of Health Education Through Session-Health Application Media On Behavior Management Behavior of Diabetes Melitus in Bengkulu CityDocument9 pagesThe Effect of Health Education Through Session-Health Application Media On Behavior Management Behavior of Diabetes Melitus in Bengkulu CityIskandar PakayaNo ratings yet
- 53 Jurnal Ilmu Kesehatan Vol. 1 No. 1 Nopember 2012: ISSN 2303-1433Document6 pages53 Jurnal Ilmu Kesehatan Vol. 1 No. 1 Nopember 2012: ISSN 2303-1433RyanSinagaNo ratings yet
- s13410 020 00876 7Document9 pagess13410 020 00876 7Vicente Fasce OlmosNo ratings yet
- 14419-Article Text-71808-1-10-20231108Document18 pages14419-Article Text-71808-1-10-20231108wtfd9t9dnrNo ratings yet
- 12 Kusrini ICOPH Vol.53 Sup2Document16 pages12 Kusrini ICOPH Vol.53 Sup2Inna 3003No ratings yet
- CiptnDocument7 pagesCiptnShinta AlfianiNo ratings yet
- Mursal 2Document12 pagesMursal 2ibrahimNo ratings yet
- Assessment of Growth Among Children With Type 1 Diabetes MellitusDocument9 pagesAssessment of Growth Among Children With Type 1 Diabetes MellitusTimothy supitNo ratings yet
- Aisyah GDM ArticleDocument18 pagesAisyah GDM ArticleBesari Md DaudNo ratings yet
- I. Made Arimbawa, Ketut Suastika, I. Ketut Junitha, I. Wayan Bikin Suryawan, Michelle HusinDocument6 pagesI. Made Arimbawa, Ketut Suastika, I. Ketut Junitha, I. Wayan Bikin Suryawan, Michelle HusinFajar SukmajayaNo ratings yet
- Srinivasan 2014Document9 pagesSrinivasan 2014Dr XNo ratings yet
- Long Term Complications in Youth Onset Type 2 Diabetes: Original ArticleDocument11 pagesLong Term Complications in Youth Onset Type 2 Diabetes: Original ArticleESPINO DE LA TORRE LUZ ELENANo ratings yet
- Repub 103040-OaDocument8 pagesRepub 103040-OaEmma Lyn SantosNo ratings yet
- Attitude of Nurses Towards Diabetes CareDocument24 pagesAttitude of Nurses Towards Diabetes CareGemgem AcostaNo ratings yet
- The Cost Effectıveness and Effect of Web-Based and Indıvıdualızed Educatıon Provıded to Classroom Teachers on the Preventıon of the Rısk of Type 2 Dıabetes the İmpact of Education on Diabetes Risk and CostDocument9 pagesThe Cost Effectıveness and Effect of Web-Based and Indıvıdualızed Educatıon Provıded to Classroom Teachers on the Preventıon of the Rısk of Type 2 Dıabetes the İmpact of Education on Diabetes Risk and CostInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal DasmarniDocument10 pagesJurnal DasmarniPutri DafrianiNo ratings yet
- Assessment of Mother's Knowledge Regarding Management of Children With Diabetes Mellitus Type 1Document10 pagesAssessment of Mother's Knowledge Regarding Management of Children With Diabetes Mellitus Type 1Rushikesh JadhavNo ratings yet
- Nutritional Status of Children in Critical Condition at Admission To Pediatric Intensive Care UnitsDocument6 pagesNutritional Status of Children in Critical Condition at Admission To Pediatric Intensive Care UnitsAnonymous h0DxuJTNo ratings yet
- Type of Diabetes in Pregnancy Impacts Risk For ChildDocument2 pagesType of Diabetes in Pregnancy Impacts Risk For ChildGerry FonziNo ratings yet
- 893-Article Text-5798-1-10-20211229Document6 pages893-Article Text-5798-1-10-20211229Fatli DjanniNo ratings yet
- Diabetes in South Africa ThesisDocument7 pagesDiabetes in South Africa Thesisuxgzruwff100% (2)
- Awareness of Diabetic Children Care Givers About Complications of Type 1 Diabetes Mellitus in Dhahran, Saudi ArabiaDocument7 pagesAwareness of Diabetic Children Care Givers About Complications of Type 1 Diabetes Mellitus in Dhahran, Saudi ArabiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hubungan Umur Dan Status Gizi Dengan Kadar Gula Darah Penderita Diabetes Melitus Tipe IiDocument11 pagesHubungan Umur Dan Status Gizi Dengan Kadar Gula Darah Penderita Diabetes Melitus Tipe IiMr. TsumNo ratings yet
- Association Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenDocument6 pagesAssociation Between Breastfeeding Patterns and Type 1 Diabetes Among ChildrenHarun joel tatipataNo ratings yet
- Pone 0118436Document19 pagesPone 0118436Tibério VasconcelosNo ratings yet
- REVIEWED Team, ch1, ch2, ch3Document20 pagesREVIEWED Team, ch1, ch2, ch3ibrahimNo ratings yet
- KAP Towards DMDocument10 pagesKAP Towards DMHabtamu Wondifraw100% (1)
- Nej Mo A 2100165Document11 pagesNej Mo A 2100165Syaffa Sadida ZahraNo ratings yet
- Childhood Obesity and Type 2 Diabetes: The Frightening EpidemicDocument2 pagesChildhood Obesity and Type 2 Diabetes: The Frightening Epidemic010390No ratings yet
- Prasetya Lestari-R1111029Document8 pagesPrasetya Lestari-R1111029Theresia SulistyaningrumNo ratings yet
- Type 2 Diabetes Mellitus - Edited.editedDocument9 pagesType 2 Diabetes Mellitus - Edited.editedBreen GreenNo ratings yet
- Classification Pathophysiology Diagnosis and ManagDocument10 pagesClassification Pathophysiology Diagnosis and ManagHeru SetiawanNo ratings yet
- Classification Pathophysiology Diagnosis and Management of Diabetesmellitus 2155 6156 1000541Document9 pagesClassification Pathophysiology Diagnosis and Management of Diabetesmellitus 2155 6156 1000541AldaniaNo ratings yet
- RAHAYU DAMAYANTI - 1610201049 - ILMU KEPERAWATAN - NaspubDocument13 pagesRAHAYU DAMAYANTI - 1610201049 - ILMU KEPERAWATAN - NaspubritaNo ratings yet
- Knowledge About Diabetic ComplicationsDocument5 pagesKnowledge About Diabetic ComplicationsAdmasu BelayNo ratings yet
- Frequency, Clinical Characteristics and Predictors of KetoacidosisDocument9 pagesFrequency, Clinical Characteristics and Predictors of KetoacidosisYogiPrimaZulkifliNo ratings yet
- Fasting Blood Glucose Levels in Adult Women With Type 2 Diabetes Mellitus and Its Associated FactorsDocument7 pagesFasting Blood Glucose Levels in Adult Women With Type 2 Diabetes Mellitus and Its Associated FactorsLiguna efendiNo ratings yet
- Jurnal 5 Meta Bahasa Inggris PubmedDocument12 pagesJurnal 5 Meta Bahasa Inggris PubmedFokus TesisNo ratings yet
- Oafw/Viewform?Edit2 2 - Abaonuf4Zkjedats-Aiwgi - Oia74Keehi5Mdskap - XTR The Background of The StudyDocument2 pagesOafw/Viewform?Edit2 2 - Abaonuf4Zkjedats-Aiwgi - Oia74Keehi5Mdskap - XTR The Background of The Studydesy rahmadantiNo ratings yet
- Diabetes GAM 2015Document7 pagesDiabetes GAM 2015Anonymous qsegfnnOdNo ratings yet
- Genetics of Type 2 Diabetes Past Present and FuturDocument12 pagesGenetics of Type 2 Diabetes Past Present and FuturChengwustZhangNo ratings yet
- Disease Specific Knowledge and Lifestyle Behavior in Patients With Diabetes Mellitus 2016 Obesity MedicineDocument4 pagesDisease Specific Knowledge and Lifestyle Behavior in Patients With Diabetes Mellitus 2016 Obesity MedicineLiaAriestaNo ratings yet
- Diabetes Mellitus and Oral Health: An Interprofessional ApproachFrom EverandDiabetes Mellitus and Oral Health: An Interprofessional ApproachNo ratings yet
- Global Incidence, Prevalence, Years Lived With Disability YLDs, Disability-Adjusted Life-YearsDocument29 pagesGlobal Incidence, Prevalence, Years Lived With Disability YLDs, Disability-Adjusted Life-Yearsluis sanchezNo ratings yet
- The High Prevalence of Overweight and Obesity in Mexican ChildrenDocument9 pagesThe High Prevalence of Overweight and Obesity in Mexican Childrenluis sanchezNo ratings yet
- StrokeDocument17 pagesStrokeluis sanchezNo ratings yet
- Worldwide Trends in Underweight and Obesity From 1990 To 2022Document24 pagesWorldwide Trends in Underweight and Obesity From 1990 To 2022luis sanchezNo ratings yet
- Analysis of SIRT1 Genetic Variants in Young Mexican Individuals. Relationships Wit Overweight and ObesityDocument12 pagesAnalysis of SIRT1 Genetic Variants in Young Mexican Individuals. Relationships Wit Overweight and Obesityluis sanchezNo ratings yet
- Carbapenem-Resistant Acinetobacter Baumannii in Latin AmericaDocument21 pagesCarbapenem-Resistant Acinetobacter Baumannii in Latin Americaluis sanchezNo ratings yet
- Clinical and Treatment Profiles of Arterial Hypertension in Mexico During The COVID-19 PandemicDocument29 pagesClinical and Treatment Profiles of Arterial Hypertension in Mexico During The COVID-19 Pandemicluis sanchezNo ratings yet
- Association Between Children's Caregivers Time Preferences and Childhood Overweight and Obesity in MexicoDocument20 pagesAssociation Between Children's Caregivers Time Preferences and Childhood Overweight and Obesity in Mexicoluis sanchezNo ratings yet
- Here's What To Know About Cardiovascular-Kidney-Metabolic Syndrome, Newly Defined by The AHADocument2 pagesHere's What To Know About Cardiovascular-Kidney-Metabolic Syndrome, Newly Defined by The AHAluis sanchezNo ratings yet
- 2023 Focused Update ESC Guidelines For The DX and TX of A&CHFDocument13 pages2023 Focused Update ESC Guidelines For The DX and TX of A&CHFluis sanchezNo ratings yet
- Associations of Socioeconomic Status and Healthy Lifestyle With Incident Early-Onset and Late-Onset DementiaDocument10 pagesAssociations of Socioeconomic Status and Healthy Lifestyle With Incident Early-Onset and Late-Onset Dementialuis sanchezNo ratings yet
- Global, Regional, and National Age-Specific Progress Towards The 2020 MilestonesDocument28 pagesGlobal, Regional, and National Age-Specific Progress Towards The 2020 Milestonesluis sanchezNo ratings yet
- The Cardiac Wound Healing Response To Myocardial InfarctionDocument19 pagesThe Cardiac Wound Healing Response To Myocardial Infarctionluis sanchezNo ratings yet
- Efficacy of Liraglutide in Obesity in Children and Adolescents. Systematic Review and Meta-Analysis of Randomized Controlled Trials. 2023Document10 pagesEfficacy of Liraglutide in Obesity in Children and Adolescents. Systematic Review and Meta-Analysis of Randomized Controlled Trials. 2023luis sanchezNo ratings yet
- The Full Value of Immunisation Against Respiratory Syncytial Virus For Infants Younger Tha 1 YearDocument10 pagesThe Full Value of Immunisation Against Respiratory Syncytial Virus For Infants Younger Tha 1 Yearluis sanchezNo ratings yet
- Obesity - 2022 - Santini - Marked Weight Loss On Liraglutide 3 0 MG Real Life Experience of A Swiss Cohort With ObesityDocument9 pagesObesity - 2022 - Santini - Marked Weight Loss On Liraglutide 3 0 MG Real Life Experience of A Swiss Cohort With Obesityluis sanchezNo ratings yet
- Chagas DiseaseDocument16 pagesChagas Diseaseluis sanchezNo ratings yet
- Two-Year Follow-Up of The COVID-19 Pandemic in MexicoDocument14 pagesTwo-Year Follow-Up of The COVID-19 Pandemic in Mexicoluis sanchezNo ratings yet
- 01 Admission Discharge Criteria and TriageDocument5 pages01 Admission Discharge Criteria and TriageSuhasani JainNo ratings yet
- Mental Health and Gender DysphoriaDocument15 pagesMental Health and Gender DysphoriaGe NomNo ratings yet
- Juliet Hurn, Laurence Church, Roxanne Keynejad, Sarah Stringer - Psychiatry P.R.N - Principles, Reality, Next Steps-Oxford University Press (2020)Document305 pagesJuliet Hurn, Laurence Church, Roxanne Keynejad, Sarah Stringer - Psychiatry P.R.N - Principles, Reality, Next Steps-Oxford University Press (2020)Francisco VillalonNo ratings yet
- Literature Review On Diabetes Mellitus in NigeriaDocument4 pagesLiterature Review On Diabetes Mellitus in Nigeriaea0kvft0100% (1)
- Basics of NeuropsychologyDocument7 pagesBasics of NeuropsychologyJasroop MahalNo ratings yet
- Voice-Related Quality of Life (V-Rqol) MeasureDocument2 pagesVoice-Related Quality of Life (V-Rqol) MeasurebarrackNo ratings yet
- Pediatric Drowning: DR Nayyar Raza KazmiDocument15 pagesPediatric Drowning: DR Nayyar Raza KazminayyarNo ratings yet
- Chronic Traumatic Encephalopathy in The Brains of Military PersonnelDocument9 pagesChronic Traumatic Encephalopathy in The Brains of Military PersonnelBruce Fredy Chino ChambillaNo ratings yet
- Trauma-And Stressor - Related DisordersDocument24 pagesTrauma-And Stressor - Related DisordersNoelle Grace Ulep BaromanNo ratings yet
- Personality Disorders Lesson PlanDocument17 pagesPersonality Disorders Lesson Planapi-284104206No ratings yet
- General Psychiatry For Residents Royal College StaffhoodDocument500 pagesGeneral Psychiatry For Residents Royal College Staffhoodpocego2767No ratings yet
- Case Study Final DraftDocument15 pagesCase Study Final Draftapi-608049224No ratings yet
- ChainingDocument38 pagesChainingKhadija ArshadNo ratings yet
- Weakness and Hypotonia: Prepared by DR Hodan Jama MDDocument38 pagesWeakness and Hypotonia: Prepared by DR Hodan Jama MDabdisalaan hassanNo ratings yet
- Prolonged LabourDocument6 pagesProlonged LabourLithiya JoseNo ratings yet
- BulimiaDocument2 pagesBulimiaGuerra Fernandes50% (2)
- Dissertation Eating DisordersDocument6 pagesDissertation Eating DisordersPapersWritingServiceHartford100% (1)
- Acute Abdomen - DR Raya Batubara, SP.BDocument39 pagesAcute Abdomen - DR Raya Batubara, SP.BGJMasterNo ratings yet
- Exam 2 BlueprintDocument6 pagesExam 2 BlueprintMindiNo ratings yet
- Care of The Client With Cranial SurgeryDocument38 pagesCare of The Client With Cranial SurgeryPatreek Wong ÜNo ratings yet
- Eating and Sleep-Wake Disorders Handout-1Document23 pagesEating and Sleep-Wake Disorders Handout-1Fulache, Lei Angeline B.No ratings yet
- Research PaperDocument6 pagesResearch PaperTham DangNo ratings yet
- Overview of The Hereditary Ataxias - UpToDateDocument15 pagesOverview of The Hereditary Ataxias - UpToDatericanoy191No ratings yet
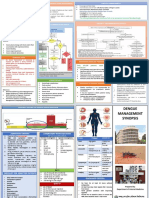
- Dengue Management Synopsis BSMMUDocument2 pagesDengue Management Synopsis BSMMURakibk65No ratings yet
- Biology Investigatory ProjectDocument20 pagesBiology Investigatory ProjectrevNo ratings yet
- Pretest Onco Key (May 2024) 1Document1 pagePretest Onco Key (May 2024) 1Nathan BuhawiNo ratings yet
- Stroke Hemoragik: Dr. Puji Pinta O. Sinurat, Sps Bagian Neurologi Fk-Umi 2019Document28 pagesStroke Hemoragik: Dr. Puji Pinta O. Sinurat, Sps Bagian Neurologi Fk-Umi 2019Desima Tamara sinuratNo ratings yet
- Is It ADHD or TraumaDocument5 pagesIs It ADHD or TraumaBojana RSNo ratings yet
- Dementia NCPDocument4 pagesDementia NCPkarl montano100% (3)