
Basic First Aid Note 2023
Basic First Aid Note 2023
You might also like
- SSP HandbookDocument246 pagesSSP Handbookacgarci83% (59)
- 9422 Accident Prevention ManualDocument84 pages9422 Accident Prevention Manuallucholade100% (2)
- Annual: PerformanceDocument176 pagesAnnual: PerformanceArja WoldeNo ratings yet
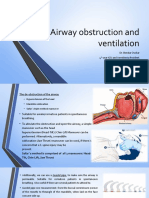
- Airway Obstruction and VentilationDocument8 pagesAirway Obstruction and VentilationJeremias KwapiszNo ratings yet
- Occupational Safety and Health Management PlanDocument30 pagesOccupational Safety and Health Management PlanRaymond R Rosales100% (1)
- Q3 Health 9 Module 1Document32 pagesQ3 Health 9 Module 1Rashiel Jane Celiz100% (1)
- Phecc CPG 2021Document188 pagesPhecc CPG 2021Mary Janine Joy RimanoNo ratings yet
- ACLS Supplementary Material PDFDocument74 pagesACLS Supplementary Material PDFsmbawasainiNo ratings yet
- Gnuhealth PDFDocument220 pagesGnuhealth PDFbhupendrapawar279No ratings yet
- Principles of Epidemiology in Public Health PracticeDocument512 pagesPrinciples of Epidemiology in Public Health PracticeAdare Oluwafemi Thomas100% (4)
- Health: Learning Activity SheetDocument48 pagesHealth: Learning Activity SheetGabrielle Tomo86% (7)
- Basic First AidDocument53 pagesBasic First Aidlead_chipmunkNo ratings yet
- Ashi Bfa SH SampleDocument12 pagesAshi Bfa SH SampleDamien AshwoodNo ratings yet
- Model of School CM PlanDocument217 pagesModel of School CM PlanBoskoNo ratings yet
- Full Textbook - CHCAGE005Document76 pagesFull Textbook - CHCAGE005Kabita123 NepzzNo ratings yet
- Disaster Preparedness Guide PDFDocument67 pagesDisaster Preparedness Guide PDFEmacon30No ratings yet
- 2017 Resident HandbookDocument61 pages2017 Resident HandbookP100% (1)
- Reabilitare Dupa AvcDocument91 pagesReabilitare Dupa AvcDiana StancaNo ratings yet
- Full Textbook - CHCCCS011Document62 pagesFull Textbook - CHCCCS011Kabita123 NepzzNo ratings yet
- CPR Pro HandbookDocument43 pagesCPR Pro HandbookResearch4OT100% (1)
- 1584 FemaDocument174 pages1584 Femamayor44patitoNo ratings yet
- International Medical Graduates in American MedicineDocument54 pagesInternational Medical Graduates in American MedicineoffdanNo ratings yet
- Preventing Heat Stress at Work PDF enDocument32 pagesPreventing Heat Stress at Work PDF enMohamed SaadNo ratings yet
- OpheaDocument75 pagesOpheaapi-391714949No ratings yet
- NAICurricula 2007Document252 pagesNAICurricula 2007tau88No ratings yet
- Student - Parent Handbook: Delasalle High SchoolDocument46 pagesStudent - Parent Handbook: Delasalle High SchoolMitch Gundran-CaisipNo ratings yet
- First Aid Digital GuideDocument63 pagesFirst Aid Digital GuidetimterakopovNo ratings yet
- ELSI Core Manual April 2012Document90 pagesELSI Core Manual April 2012sacabonaNo ratings yet
- dental-hygiene-student-manual-19-20Document62 pagesdental-hygiene-student-manual-19-20livrodontoNo ratings yet
- CPR AED and Basic FirstAidDocument77 pagesCPR AED and Basic FirstAidIsabel Cristina Jaramillo100% (1)
- Wa0000.Document51 pagesWa0000.rishaunagNo ratings yet
- EmergencysafetyguideDocument211 pagesEmergencysafetyguideapi-287826317No ratings yet
- Health Safety Craft Breweries Distilleries bk164 PDF en PDFDocument76 pagesHealth Safety Craft Breweries Distilleries bk164 PDF en PDFJai AndalesNo ratings yet
- Student Manual 2019 ECOEDocument38 pagesStudent Manual 2019 ECOEScribdTranslationsNo ratings yet
- FA ManualDocument346 pagesFA ManualbabudevanandNo ratings yet
- Infection Control ManualDocument206 pagesInfection Control Manualastha singhNo ratings yet
- PDF Human Factors in Air Transport Understanding Behavior and Performance in Aviation Erik Seedhouse Ebook Full ChapterDocument46 pagesPDF Human Factors in Air Transport Understanding Behavior and Performance in Aviation Erik Seedhouse Ebook Full Chapterwendell.vaughn463100% (3)
- Ophthalmic Nursing - Getting StartedDocument72 pagesOphthalmic Nursing - Getting StartedRamesh BabuNo ratings yet
- 50 Tips For More Effective Safety TrainingDocument64 pages50 Tips For More Effective Safety Trainingpjuan211100% (1)
- Fema Covid 19 Pandemic Operational Guidance 5-17-2021Document85 pagesFema Covid 19 Pandemic Operational Guidance 5-17-2021slayNo ratings yet
- Cadet Basic Training Guide (2000)Document105 pagesCadet Basic Training Guide (2000)CAP History Library100% (1)
- National Final Report: Cross-Site at Home/Chez Soi ProjectDocument48 pagesNational Final Report: Cross-Site at Home/Chez Soi ProjectOmer ErgeanNo ratings yet
- Universal Jurisdiction Law and Practice in FinlandDocument35 pagesUniversal Jurisdiction Law and Practice in FinlandAchraf RabadiNo ratings yet
- PDF 2013 EIS ConferenceDocument143 pagesPDF 2013 EIS Conferencecharlene zechenderNo ratings yet
- ScenariosDocument39 pagesScenariosNunuy NuriahNo ratings yet
- 47478finaldmmanualDocument63 pages47478finaldmmanualMonydit SantinoNo ratings yet
- Mindfulness Metacognitive Awareness Guide FINAL 20200512Document71 pagesMindfulness Metacognitive Awareness Guide FINAL 20200512Maria Menendez MartinNo ratings yet
- Epi Dem OlogyDocument512 pagesEpi Dem OlogyDevansh KumarNo ratings yet
- Workers' Compensation and Injury Management at UWADocument34 pagesWorkers' Compensation and Injury Management at UWANaveen ChaudharyNo ratings yet
- Home Office-Dealing With DisasterDocument104 pagesHome Office-Dealing With DisastervilladoloresNo ratings yet
- WTRTFDocument384 pagesWTRTFNewsNo ratings yet
- Cardiothoracic Care for Children and Young People: A Multidisciplinary ApproachFrom EverandCardiothoracic Care for Children and Young People: A Multidisciplinary ApproachKerry CookNo ratings yet
- SENIOR CITIZEN LIVING: Discover How You Can Make Your Senior Years As Golden as Possible!From EverandSENIOR CITIZEN LIVING: Discover How You Can Make Your Senior Years As Golden as Possible!No ratings yet
- Teaching Civics: A Manual for Secondary Education TeachersFrom EverandTeaching Civics: A Manual for Secondary Education TeachersNo ratings yet
- Living with Hearing Difficulties: The process of enablementFrom EverandLiving with Hearing Difficulties: The process of enablementNo ratings yet
- The Amazing Biological Revolution and The Amazing New Health CareFrom EverandThe Amazing Biological Revolution and The Amazing New Health CareNo ratings yet
- Epidemic Leadership: How to Lead Infectiously in the Era of Big ProblemsFrom EverandEpidemic Leadership: How to Lead Infectiously in the Era of Big ProblemsNo ratings yet
- Striving for Clean Air: Air Pollution and Public Health in South AsiaFrom EverandStriving for Clean Air: Air Pollution and Public Health in South AsiaNo ratings yet
- Staying Well After Psychosis: A Cognitive Interpersonal Approach to Recovery and Relapse PreventionFrom EverandStaying Well After Psychosis: A Cognitive Interpersonal Approach to Recovery and Relapse PreventionNo ratings yet
- Crowding of Structures and People May Prevent Poor Draining Leading To More Serious Problems Such As The FollowingDocument11 pagesCrowding of Structures and People May Prevent Poor Draining Leading To More Serious Problems Such As The FollowingAngela NeriNo ratings yet
- اسنان باطنة Clinical FinalDocument40 pagesاسنان باطنة Clinical FinalShady AnwarNo ratings yet
- ICAO Aviation English Proficiency Evaluation: Practice Materials Part G - Story RetellingDocument3 pagesICAO Aviation English Proficiency Evaluation: Practice Materials Part G - Story RetellingGökçen Akma100% (1)
- First Aid QuizDocument8 pagesFirst Aid QuizNightrider TLFNo ratings yet
- First Aid and Water SurvivalDocument59 pagesFirst Aid and Water SurvivalLaurenz Logmao PascuaNo ratings yet
- Microsoft PowerPoint - BHDDocument35 pagesMicrosoft PowerPoint - BHDandarias kevinNo ratings yet
- First Aid: Reinila D. Manalang Btvted FSM 3-ADocument17 pagesFirst Aid: Reinila D. Manalang Btvted FSM 3-ARein Dayrit ManalangNo ratings yet
- Cardiopulmonary 3 2010 With AnswersDocument14 pagesCardiopulmonary 3 2010 With AnswersWenzy Cruz100% (3)
- CPR 2Document3 pagesCPR 2Baebee Lou100% (1)
- Module 4 - Applying Basic First AidDocument2 pagesModule 4 - Applying Basic First AidjessafesalazarNo ratings yet
- Skill 32.1 Using A Bed or Chair Exit Safety Monitoring DeviceDocument7 pagesSkill 32.1 Using A Bed or Chair Exit Safety Monitoring Devicerahtu suzi ameliaNo ratings yet
- US Navy Course NAVEDTRA 13119 - Standard First Aid CourseDocument175 pagesUS Navy Course NAVEDTRA 13119 - Standard First Aid CourseGeorges100% (4)
- Infant CPR ProcedureDocument3 pagesInfant CPR ProcedureDaniica MacaranasNo ratings yet
- Nursing Test 3 (NP Iv)Document16 pagesNursing Test 3 (NP Iv)Yuxin LiuNo ratings yet
- Emergency Nursing (Medical Emergencies - ABC) - StudentsDocument19 pagesEmergency Nursing (Medical Emergencies - ABC) - StudentsAngielyn Ramos OlorazaNo ratings yet
- First Aid Is An Immediate, Temporary and Continuing Care Given To A Person Who Has Been Injured or Suddenly Taken IllDocument56 pagesFirst Aid Is An Immediate, Temporary and Continuing Care Given To A Person Who Has Been Injured or Suddenly Taken IllLemery MpsNo ratings yet
- Second Academic Work For English Five - 2022 - I: (Fecha de Entrega Hasta El 17 de Julio 2022)Document9 pagesSecond Academic Work For English Five - 2022 - I: (Fecha de Entrega Hasta El 17 de Julio 2022)leliloveNo ratings yet
- Unintentional InjuriesDocument11 pagesUnintentional InjuriesFrance FabroaNo ratings yet
- Standard 12 - Basic Life SupportDocument15 pagesStandard 12 - Basic Life SupportLuiza UngureanuNo ratings yet
- CPR Consist of 4 Main Parts Which AreDocument6 pagesCPR Consist of 4 Main Parts Which Arematgar100% (3)
- CPR InfantDocument4 pagesCPR InfantLorelyn Santos CorpuzNo ratings yet
- Edacs 1Document1 pageEdacs 1CARME FORGAS MASSONo ratings yet
- Airway Obstruction and Foreign BodiesDocument26 pagesAirway Obstruction and Foreign BodiesQuolette ConstanteNo ratings yet
- Prepper's Medical Handbook - Prepper's Long-Term Survival Guide For BeginnersDocument297 pagesPrepper's Medical Handbook - Prepper's Long-Term Survival Guide For Beginnersfalcao_daniel100% (3)
- Saudi Heart Association Presentation Highlighted PDFDocument72 pagesSaudi Heart Association Presentation Highlighted PDFStephanie AquinoNo ratings yet
- Loose Parts: What Does This Mean?Document2 pagesLoose Parts: What Does This Mean?kinderb2 2020nisNo ratings yet
- CPR Alternate Assignment HOPEDocument5 pagesCPR Alternate Assignment HOPEMadison Snyder75% (4)





















































































Download as pdf or txt
You might also like
- SSP HandbookDocument246 pagesSSP Handbookacgarci83% (59)
- 9422 Accident Prevention ManualDocument84 pages9422 Accident Prevention Manuallucholade100% (2)
- Annual: PerformanceDocument176 pagesAnnual: PerformanceArja WoldeNo ratings yet
- Airway Obstruction and VentilationDocument8 pagesAirway Obstruction and VentilationJeremias KwapiszNo ratings yet
- Occupational Safety and Health Management PlanDocument30 pagesOccupational Safety and Health Management PlanRaymond R Rosales100% (1)
- Q3 Health 9 Module 1Document32 pagesQ3 Health 9 Module 1Rashiel Jane Celiz100% (1)
- Phecc CPG 2021Document188 pagesPhecc CPG 2021Mary Janine Joy RimanoNo ratings yet
- ACLS Supplementary Material PDFDocument74 pagesACLS Supplementary Material PDFsmbawasainiNo ratings yet
- Gnuhealth PDFDocument220 pagesGnuhealth PDFbhupendrapawar279No ratings yet
- Principles of Epidemiology in Public Health PracticeDocument512 pagesPrinciples of Epidemiology in Public Health PracticeAdare Oluwafemi Thomas100% (4)
- Health: Learning Activity SheetDocument48 pagesHealth: Learning Activity SheetGabrielle Tomo86% (7)
- Basic First AidDocument53 pagesBasic First Aidlead_chipmunkNo ratings yet
- Ashi Bfa SH SampleDocument12 pagesAshi Bfa SH SampleDamien AshwoodNo ratings yet
- Model of School CM PlanDocument217 pagesModel of School CM PlanBoskoNo ratings yet
- Full Textbook - CHCAGE005Document76 pagesFull Textbook - CHCAGE005Kabita123 NepzzNo ratings yet
- Disaster Preparedness Guide PDFDocument67 pagesDisaster Preparedness Guide PDFEmacon30No ratings yet
- 2017 Resident HandbookDocument61 pages2017 Resident HandbookP100% (1)
- Reabilitare Dupa AvcDocument91 pagesReabilitare Dupa AvcDiana StancaNo ratings yet
- Full Textbook - CHCCCS011Document62 pagesFull Textbook - CHCCCS011Kabita123 NepzzNo ratings yet
- CPR Pro HandbookDocument43 pagesCPR Pro HandbookResearch4OT100% (1)
- 1584 FemaDocument174 pages1584 Femamayor44patitoNo ratings yet
- International Medical Graduates in American MedicineDocument54 pagesInternational Medical Graduates in American MedicineoffdanNo ratings yet
- Preventing Heat Stress at Work PDF enDocument32 pagesPreventing Heat Stress at Work PDF enMohamed SaadNo ratings yet
- OpheaDocument75 pagesOpheaapi-391714949No ratings yet
- NAICurricula 2007Document252 pagesNAICurricula 2007tau88No ratings yet
- Student - Parent Handbook: Delasalle High SchoolDocument46 pagesStudent - Parent Handbook: Delasalle High SchoolMitch Gundran-CaisipNo ratings yet
- First Aid Digital GuideDocument63 pagesFirst Aid Digital GuidetimterakopovNo ratings yet
- ELSI Core Manual April 2012Document90 pagesELSI Core Manual April 2012sacabonaNo ratings yet
- dental-hygiene-student-manual-19-20Document62 pagesdental-hygiene-student-manual-19-20livrodontoNo ratings yet
- CPR AED and Basic FirstAidDocument77 pagesCPR AED and Basic FirstAidIsabel Cristina Jaramillo100% (1)
- Wa0000.Document51 pagesWa0000.rishaunagNo ratings yet
- EmergencysafetyguideDocument211 pagesEmergencysafetyguideapi-287826317No ratings yet
- Health Safety Craft Breweries Distilleries bk164 PDF en PDFDocument76 pagesHealth Safety Craft Breweries Distilleries bk164 PDF en PDFJai AndalesNo ratings yet
- Student Manual 2019 ECOEDocument38 pagesStudent Manual 2019 ECOEScribdTranslationsNo ratings yet
- FA ManualDocument346 pagesFA ManualbabudevanandNo ratings yet
- Infection Control ManualDocument206 pagesInfection Control Manualastha singhNo ratings yet
- PDF Human Factors in Air Transport Understanding Behavior and Performance in Aviation Erik Seedhouse Ebook Full ChapterDocument46 pagesPDF Human Factors in Air Transport Understanding Behavior and Performance in Aviation Erik Seedhouse Ebook Full Chapterwendell.vaughn463100% (3)
- Ophthalmic Nursing - Getting StartedDocument72 pagesOphthalmic Nursing - Getting StartedRamesh BabuNo ratings yet
- 50 Tips For More Effective Safety TrainingDocument64 pages50 Tips For More Effective Safety Trainingpjuan211100% (1)
- Fema Covid 19 Pandemic Operational Guidance 5-17-2021Document85 pagesFema Covid 19 Pandemic Operational Guidance 5-17-2021slayNo ratings yet
- Cadet Basic Training Guide (2000)Document105 pagesCadet Basic Training Guide (2000)CAP History Library100% (1)
- National Final Report: Cross-Site at Home/Chez Soi ProjectDocument48 pagesNational Final Report: Cross-Site at Home/Chez Soi ProjectOmer ErgeanNo ratings yet
- Universal Jurisdiction Law and Practice in FinlandDocument35 pagesUniversal Jurisdiction Law and Practice in FinlandAchraf RabadiNo ratings yet
- PDF 2013 EIS ConferenceDocument143 pagesPDF 2013 EIS Conferencecharlene zechenderNo ratings yet
- ScenariosDocument39 pagesScenariosNunuy NuriahNo ratings yet
- 47478finaldmmanualDocument63 pages47478finaldmmanualMonydit SantinoNo ratings yet
- Mindfulness Metacognitive Awareness Guide FINAL 20200512Document71 pagesMindfulness Metacognitive Awareness Guide FINAL 20200512Maria Menendez MartinNo ratings yet
- Epi Dem OlogyDocument512 pagesEpi Dem OlogyDevansh KumarNo ratings yet
- Workers' Compensation and Injury Management at UWADocument34 pagesWorkers' Compensation and Injury Management at UWANaveen ChaudharyNo ratings yet
- Home Office-Dealing With DisasterDocument104 pagesHome Office-Dealing With DisastervilladoloresNo ratings yet
- WTRTFDocument384 pagesWTRTFNewsNo ratings yet
- Cardiothoracic Care for Children and Young People: A Multidisciplinary ApproachFrom EverandCardiothoracic Care for Children and Young People: A Multidisciplinary ApproachKerry CookNo ratings yet
- SENIOR CITIZEN LIVING: Discover How You Can Make Your Senior Years As Golden as Possible!From EverandSENIOR CITIZEN LIVING: Discover How You Can Make Your Senior Years As Golden as Possible!No ratings yet
- Teaching Civics: A Manual for Secondary Education TeachersFrom EverandTeaching Civics: A Manual for Secondary Education TeachersNo ratings yet
- Living with Hearing Difficulties: The process of enablementFrom EverandLiving with Hearing Difficulties: The process of enablementNo ratings yet
- The Amazing Biological Revolution and The Amazing New Health CareFrom EverandThe Amazing Biological Revolution and The Amazing New Health CareNo ratings yet
- Epidemic Leadership: How to Lead Infectiously in the Era of Big ProblemsFrom EverandEpidemic Leadership: How to Lead Infectiously in the Era of Big ProblemsNo ratings yet
- Striving for Clean Air: Air Pollution and Public Health in South AsiaFrom EverandStriving for Clean Air: Air Pollution and Public Health in South AsiaNo ratings yet
- Staying Well After Psychosis: A Cognitive Interpersonal Approach to Recovery and Relapse PreventionFrom EverandStaying Well After Psychosis: A Cognitive Interpersonal Approach to Recovery and Relapse PreventionNo ratings yet
- Crowding of Structures and People May Prevent Poor Draining Leading To More Serious Problems Such As The FollowingDocument11 pagesCrowding of Structures and People May Prevent Poor Draining Leading To More Serious Problems Such As The FollowingAngela NeriNo ratings yet
- اسنان باطنة Clinical FinalDocument40 pagesاسنان باطنة Clinical FinalShady AnwarNo ratings yet
- ICAO Aviation English Proficiency Evaluation: Practice Materials Part G - Story RetellingDocument3 pagesICAO Aviation English Proficiency Evaluation: Practice Materials Part G - Story RetellingGökçen Akma100% (1)
- First Aid QuizDocument8 pagesFirst Aid QuizNightrider TLFNo ratings yet
- First Aid and Water SurvivalDocument59 pagesFirst Aid and Water SurvivalLaurenz Logmao PascuaNo ratings yet
- Microsoft PowerPoint - BHDDocument35 pagesMicrosoft PowerPoint - BHDandarias kevinNo ratings yet
- First Aid: Reinila D. Manalang Btvted FSM 3-ADocument17 pagesFirst Aid: Reinila D. Manalang Btvted FSM 3-ARein Dayrit ManalangNo ratings yet
- Cardiopulmonary 3 2010 With AnswersDocument14 pagesCardiopulmonary 3 2010 With AnswersWenzy Cruz100% (3)
- CPR 2Document3 pagesCPR 2Baebee Lou100% (1)
- Module 4 - Applying Basic First AidDocument2 pagesModule 4 - Applying Basic First AidjessafesalazarNo ratings yet
- Skill 32.1 Using A Bed or Chair Exit Safety Monitoring DeviceDocument7 pagesSkill 32.1 Using A Bed or Chair Exit Safety Monitoring Devicerahtu suzi ameliaNo ratings yet
- US Navy Course NAVEDTRA 13119 - Standard First Aid CourseDocument175 pagesUS Navy Course NAVEDTRA 13119 - Standard First Aid CourseGeorges100% (4)
- Infant CPR ProcedureDocument3 pagesInfant CPR ProcedureDaniica MacaranasNo ratings yet
- Nursing Test 3 (NP Iv)Document16 pagesNursing Test 3 (NP Iv)Yuxin LiuNo ratings yet
- Emergency Nursing (Medical Emergencies - ABC) - StudentsDocument19 pagesEmergency Nursing (Medical Emergencies - ABC) - StudentsAngielyn Ramos OlorazaNo ratings yet
- First Aid Is An Immediate, Temporary and Continuing Care Given To A Person Who Has Been Injured or Suddenly Taken IllDocument56 pagesFirst Aid Is An Immediate, Temporary and Continuing Care Given To A Person Who Has Been Injured or Suddenly Taken IllLemery MpsNo ratings yet
- Second Academic Work For English Five - 2022 - I: (Fecha de Entrega Hasta El 17 de Julio 2022)Document9 pagesSecond Academic Work For English Five - 2022 - I: (Fecha de Entrega Hasta El 17 de Julio 2022)leliloveNo ratings yet
- Unintentional InjuriesDocument11 pagesUnintentional InjuriesFrance FabroaNo ratings yet
- Standard 12 - Basic Life SupportDocument15 pagesStandard 12 - Basic Life SupportLuiza UngureanuNo ratings yet
- CPR Consist of 4 Main Parts Which AreDocument6 pagesCPR Consist of 4 Main Parts Which Arematgar100% (3)
- CPR InfantDocument4 pagesCPR InfantLorelyn Santos CorpuzNo ratings yet
- Edacs 1Document1 pageEdacs 1CARME FORGAS MASSONo ratings yet
- Airway Obstruction and Foreign BodiesDocument26 pagesAirway Obstruction and Foreign BodiesQuolette ConstanteNo ratings yet
- Prepper's Medical Handbook - Prepper's Long-Term Survival Guide For BeginnersDocument297 pagesPrepper's Medical Handbook - Prepper's Long-Term Survival Guide For Beginnersfalcao_daniel100% (3)
- Saudi Heart Association Presentation Highlighted PDFDocument72 pagesSaudi Heart Association Presentation Highlighted PDFStephanie AquinoNo ratings yet
- Loose Parts: What Does This Mean?Document2 pagesLoose Parts: What Does This Mean?kinderb2 2020nisNo ratings yet
- CPR Alternate Assignment HOPEDocument5 pagesCPR Alternate Assignment HOPEMadison Snyder75% (4)