Download as pdf or txt
You might also like
- 10.1097@00006534 201511001 00017Document9 pages10.1097@00006534 201511001 00017JoãoNo ratings yet
- Bodyblade Exercise Guide WallchartDocument1 pageBodyblade Exercise Guide WallchartDavid Leonardo Rodriguez SarmientoNo ratings yet
- Mid Face Rejuvenation PDFDocument3 pagesMid Face Rejuvenation PDFAlan LongNo ratings yet
- Pathophysiology of StrokeDocument2 pagesPathophysiology of StrokeACe JAy100% (2)
- Anatomy of The Face and Neck: Peter M. PrendergastDocument18 pagesAnatomy of The Face and Neck: Peter M. PrendergastMaher Khoury100% (1)
- Volumetric Structural Rejuvenation For The Male Face PDFDocument6 pagesVolumetric Structural Rejuvenation For The Male Face PDFImanuel CristiantoNo ratings yet
- Commissuroplasty: Sean M Parsel, DO, Ryan D Winters, MDDocument5 pagesCommissuroplasty: Sean M Parsel, DO, Ryan D Winters, MDAndy HongNo ratings yet
- Hypertrophy Execution Mastery - Module 2 Workouts - Biceps & Triceps PDFDocument24 pagesHypertrophy Execution Mastery - Module 2 Workouts - Biceps & Triceps PDFMarvin100% (1)
- Cornea: Points From Snell's Ocular Anatomy Compiled by Dr. AliDocument14 pagesCornea: Points From Snell's Ocular Anatomy Compiled by Dr. Ali9999999999999-567421No ratings yet
- 37 1Document3 pages37 1MoneymakerNo ratings yet
- Cephalocaudal Assessment (Cen)Document4 pagesCephalocaudal Assessment (Cen)Kristine Young100% (1)
- Facial Cosmetic Surgery - YjomsDocument2 pagesFacial Cosmetic Surgery - YjomsPaulo Ferreira OrtodontiaNo ratings yet
- Anatomy of The Face and Neck: Peter M. PrendergastDocument18 pagesAnatomy of The Face and Neck: Peter M. PrendergastPaul SalahoruNo ratings yet
- 266 2021 Art Mercado-RossoDocument12 pages266 2021 Art Mercado-RossoIsnelda EricesNo ratings yet
- Application of Botulinum Toxin in Maxillofacial Field: Part II. Wrinkle, Intraoral Ulcer, and Cranio-Maxillofacial PainDocument15 pagesApplication of Botulinum Toxin in Maxillofacial Field: Part II. Wrinkle, Intraoral Ulcer, and Cranio-Maxillofacial PainmatheuscorreabmfNo ratings yet
- 2019 Humzah Tateo Siquier Neck ApproachDocument4 pages2019 Humzah Tateo Siquier Neck ApproachANDRÉ CAMARGONo ratings yet
- Aplied Anatomy BotoxDocument8 pagesAplied Anatomy BotoxYesuratnam DudduNo ratings yet
- The Skin RejuvenationDocument7 pagesThe Skin Rejuvenationbruno mañonNo ratings yet
- 00012Document11 pages00012t3klaNo ratings yet
- Botulinum Toxin Below The Eyes - CarruthersDocument9 pagesBotulinum Toxin Below The Eyes - CarruthersRafael Autran Cavalcante AraújoNo ratings yet
- Where and How To Use Botulinum Toxin On The Face and Neck - Indications and TechniquesDocument9 pagesWhere and How To Use Botulinum Toxin On The Face and Neck - Indications and Techniqueskahkashanahmed065No ratings yet
- Gummy Smile - Mercado-Rosso Classification System and Dynamic Restructuring With Hyaluronic Acid - PMCDocument21 pagesGummy Smile - Mercado-Rosso Classification System and Dynamic Restructuring With Hyaluronic Acid - PMCBelanwahidNo ratings yet
- Nonsurgical Jawline Rejuvenation Using Injectable FillersDocument8 pagesNonsurgical Jawline Rejuvenation Using Injectable FillersArcelino FariasNo ratings yet
- Descripción General Del Envejecimiento Facial. Cirugía Plástica Facial, 2009 25 (05), 281-284. Doi10.1055s-0029-1243075Document4 pagesDescripción General Del Envejecimiento Facial. Cirugía Plástica Facial, 2009 25 (05), 281-284. Doi10.1055s-0029-1243075Germania GavilanesNo ratings yet
- Voluma 2008Document9 pagesVoluma 2008Sharif SalamehNo ratings yet
- Anatomy and Functions of The Muscles of Facial ExpressionDocument15 pagesAnatomy and Functions of The Muscles of Facial Expressionpaolahn14No ratings yet
- B T (B) E F M AL R: Otulinum Oxin Otox TO Nhance Acial Acroesthetics: Iterature EviewDocument8 pagesB T (B) E F M AL R: Otulinum Oxin Otox TO Nhance Acial Acroesthetics: Iterature EviewAnderson AraujoNo ratings yet
- Genioplasty Evaluation and ManagementDocument6 pagesGenioplasty Evaluation and ManagementAnkita GuravNo ratings yet
- Chia CY, Et Al. Clinical Anatomy of The Face. Clin Dermatol J 2017, 2 (1) - 000107Document8 pagesChia CY, Et Al. Clinical Anatomy of The Face. Clin Dermatol J 2017, 2 (1) - 000107carolina100% (1)
- Subperiosteal Chin Augmentation With Hyaluronic AcDocument10 pagesSubperiosteal Chin Augmentation With Hyaluronic AcPriscilla SamuelNo ratings yet
- Speech OrgansDocument4 pagesSpeech OrgansJ'onn J'onzzNo ratings yet
- Face LiftDocument18 pagesFace LiftreyllcNo ratings yet
- Volume Facial e IdadeDocument6 pagesVolume Facial e IdadeJeniffer RafaelaNo ratings yet
- Rubens 1989Document8 pagesRubens 1989José Cunha CoutinhoNo ratings yet
- Facial Fillers Relevant Anatomy Injection TechniquDocument9 pagesFacial Fillers Relevant Anatomy Injection TechniquMasoud Rahimi100% (1)
- 4 Cotofana 2016Document8 pages4 Cotofana 2016Thamyres Branco100% (1)
- Hazards of Using Guiding Elastics For Maxillo Mandibular Fixation MMF After Open Reduction and Internal Fixation Orif of Upper Mid Jcofs 1000107Document4 pagesHazards of Using Guiding Elastics For Maxillo Mandibular Fixation MMF After Open Reduction and Internal Fixation Orif of Upper Mid Jcofs 1000107dehaaNo ratings yet
- The Jaw and Related StructuresDocument6 pagesThe Jaw and Related Structuresarzdar100% (1)
- Mid Face Rejuvenation PDFDocument3 pagesMid Face Rejuvenation PDFAlan Long100% (1)
- Jco 1998 07 432Document14 pagesJco 1998 07 432Pulkit BimalNo ratings yet
- Anatomy of The Lower Face and Botulinum Toxin.16Document8 pagesAnatomy of The Lower Face and Botulinum Toxin.16Dogan TuncaliNo ratings yet
- Aesthetics Revision Very GoodDocument62 pagesAesthetics Revision Very GoodAndre3893No ratings yet
- The Anatomy of The Aging FaceA ReviewDocument8 pagesThe Anatomy of The Aging FaceA ReviewDoctores Duarte BarrosNo ratings yet
- Treatment of Mid Face Expression RhytidesDocument13 pagesTreatment of Mid Face Expression Rhytideslorena gurdzNo ratings yet
- Mazzola 2014Document9 pagesMazzola 2014Familia Chica SoteloNo ratings yet
- BOTOX: Broadening The Horizon of Dentistry: Abst TDocument5 pagesBOTOX: Broadening The Horizon of Dentistry: Abst TŞükriye AngaNo ratings yet
- Fillers BellDocument12 pagesFillers Belldanielagonzalezt5No ratings yet
- v2 Anatomia Da Face Aplicada Aos Preenchedores e A Toxina Botulinica - Parte IIDocument11 pagesv2 Anatomia Da Face Aplicada Aos Preenchedores e A Toxina Botulinica - Parte IIGiovanna CostaNo ratings yet
- Jump To Navigationjump To Search: For Other Uses, See - "Faces" Redirects Here. For Other Uses, SeeDocument6 pagesJump To Navigationjump To Search: For Other Uses, See - "Faces" Redirects Here. For Other Uses, SeeFe GregorioNo ratings yet
- Smile Analysis PDFDocument4 pagesSmile Analysis PDFtikaNo ratings yet
- Facial AgingDocument8 pagesFacial Agingdanielagonzalezt5No ratings yet
- Botox For The Eyes and BrowDocument5 pagesBotox For The Eyes and Browlfan0% (1)
- FPS 00978Document9 pagesFPS 00978Gonçalo Cunha-CoutinhoNo ratings yet
- Newer Understanding of Specific Anatomic Targets in The Aging Face As Applied To Injectables - Aging Changes in The Craniofacial Skeleton and Facial LigamentsDocument5 pagesNewer Understanding of Specific Anatomic Targets in The Aging Face As Applied To Injectables - Aging Changes in The Craniofacial Skeleton and Facial LigamentsArcelino FariasNo ratings yet
- PAPER Anatomy and Aging of Cheek Fat Compartiments. Salvatore FundaróDocument7 pagesPAPER Anatomy and Aging of Cheek Fat Compartiments. Salvatore FundaróCATALINA PIA ROMERO CORTEZ100% (2)
- Smile Review 2015Document6 pagesSmile Review 2015Guillem BernalNo ratings yet
- Evidence-Based Medicine: Face Lift: Learning Objectives: After Studying This Article, The Participants Should Be AbleDocument17 pagesEvidence-Based Medicine: Face Lift: Learning Objectives: After Studying This Article, The Participants Should Be AbleМаратNo ratings yet
- Face LiftDocument22 pagesFace Lifthansmaloo100% (1)
- Botulinum Toxin For The FaceDocument12 pagesBotulinum Toxin For The Facerizwan javedNo ratings yet
- The Layered Anatomy of The JawlineDocument7 pagesThe Layered Anatomy of The Jawlineletty3gape100% (1)
- Tailored Injection Techniques in The Mid and Lower Face Using A Multilayering ApproachDocument9 pagesTailored Injection Techniques in The Mid and Lower Face Using A Multilayering Approachalh basharNo ratings yet
- Perioral RejuvenationDocument11 pagesPerioral RejuvenationjuliemonneypennyNo ratings yet
- Lip Diagnostics New Reflection Zones of The Human Organs On The Lips 882Document8 pagesLip Diagnostics New Reflection Zones of The Human Organs On The Lips 882Akın AKDERENo ratings yet
- ProsdentDocument4 pagesProsdentMax PosseltNo ratings yet
- Homeopathy in Practice: Clinical Insights into Homeopathy & RemediesFrom EverandHomeopathy in Practice: Clinical Insights into Homeopathy & RemediesNo ratings yet
- Occupational Health Tips On Eye Protection For Good Visual HealthFrom EverandOccupational Health Tips On Eye Protection For Good Visual HealthNo ratings yet
- Motor Fitness Test 2019 Class Xii Notes-1Document3 pagesMotor Fitness Test 2019 Class Xii Notes-1PRITAM MITRA82% (60)
- Endocrine PathologyDocument31 pagesEndocrine PathologyAnonymous 49jFPGI5KN100% (1)
- One Lung VentilationDocument38 pagesOne Lung VentilationVarun Reddy V100% (1)
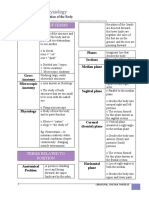
- Anatomy and Physiology: Definition of TermsDocument11 pagesAnatomy and Physiology: Definition of TermsPhilipp LibasoraNo ratings yet
- Orthopaedics New Recruit Examination March 2012Document9 pagesOrthopaedics New Recruit Examination March 2012Gumilang Satrio PNo ratings yet
- AnatomyDocument116 pagesAnatomyyousef sarairehNo ratings yet
- Health AssessmentDocument31 pagesHealth AssessmentLoi Ocampo Crespo100% (1)
- Past Papers Section2Document13 pagesPast Papers Section2Jerilee SoCute Watts50% (2)
- Socrative Quiz 1Document3 pagesSocrative Quiz 1Rachel HayonNo ratings yet
- Department of Education: Summative Test in Science 10Document3 pagesDepartment of Education: Summative Test in Science 10Christine RamosNo ratings yet
- BD Chaurasia PDFDocument18 pagesBD Chaurasia PDFVishwakarma AmitNo ratings yet
- Physiology of HearingDocument36 pagesPhysiology of HearingPrakash PanthiNo ratings yet
- Anatomy One Liners PDFDocument12 pagesAnatomy One Liners PDFAbida AhmedNo ratings yet
- 18 ExcretionDocument70 pages18 ExcretionqingxuguNo ratings yet
- The Articulated Alar Rim Graft: Reengineering The Conventional Alar Rim Graft For Improved Contour and SupportDocument14 pagesThe Articulated Alar Rim Graft: Reengineering The Conventional Alar Rim Graft For Improved Contour and SupportKarina AlvearNo ratings yet
- Extraoral Orthopaedic AppliancesDocument59 pagesExtraoral Orthopaedic AppliancesAmatullahsadiyaNo ratings yet
- Common Nomal VariationDocument3 pagesCommon Nomal Variationngurah123456789No ratings yet
- PCP P-1Document8 pagesPCP P-1VIHAAN SINGH DHAMINo ratings yet
- MCQDocument285 pagesMCQjielani100% (1)
- Disorders of Endocrine SystemDocument48 pagesDisorders of Endocrine SystemSHARIM ASGHARNo ratings yet
- Struktur Dan Mekanisme Kerja Jantung Pada Manusia: AbstractDocument18 pagesStruktur Dan Mekanisme Kerja Jantung Pada Manusia: AbstractZaneta FajarNo ratings yet
- Ortho CaseDocument26 pagesOrtho CaseYusra ShaukatNo ratings yet
- Hindfoot Valgus: AP Talocalcaneal Angle (Kite's Angle)Document4 pagesHindfoot Valgus: AP Talocalcaneal Angle (Kite's Angle)JoaoNo ratings yet
- Socrative QuizDocument1 pageSocrative Quizapi-344681706No ratings yet