Download as pdf or txt
You might also like
- DNB Question Paper-System wise-DNB AnaesthesiaDocument88 pagesDNB Question Paper-System wise-DNB AnaesthesiaSirisha Ckv83% (18)
- When To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsDocument9 pagesWhen To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsepraetorianNo ratings yet
- CCJC BodinDocument2 pagesCCJC Bodinapi-495663503No ratings yet
- Analysis of 67 CasesDocument8 pagesAnalysis of 67 CasesHitesh ChandwaniNo ratings yet
- Antipsychotic PolypharmacyDocument10 pagesAntipsychotic PolypharmacymarcoNo ratings yet
- Pediatric Premedication: A Double-Blind Randomized Trial of Dexmedetomidine or Ketamine Alone Versus A Combination of Dexmedetomidine and KetamineDocument7 pagesPediatric Premedication: A Double-Blind Randomized Trial of Dexmedetomidine or Ketamine Alone Versus A Combination of Dexmedetomidine and KetamineFatty MaulidiraNo ratings yet
- En A09v83n2s0 PDFDocument12 pagesEn A09v83n2s0 PDFRiriNo ratings yet
- Ketamine As Rescue Treatment FDocument8 pagesKetamine As Rescue Treatment Fandrew herringNo ratings yet
- ACEP Ketamine Guideline 2011Document13 pagesACEP Ketamine Guideline 2011Daniel Crook100% (1)
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- Withdrawal Syndrome in The Pediatric Intensive Care Unit. Incidence and Risk FactorsDocument8 pagesWithdrawal Syndrome in The Pediatric Intensive Care Unit. Incidence and Risk Factorsfuka priesleyNo ratings yet
- ChayapathiDocument8 pagesChayapathiVINICIUS CAMARGO KISSNo ratings yet
- Clozapine: SchizophrenicDocument8 pagesClozapine: SchizophrenicVictoria FellowsNo ratings yet
- PCCM Suppl Mar 2016Document13 pagesPCCM Suppl Mar 2016Xavier AbrilNo ratings yet
- Kane1988 PDFDocument8 pagesKane1988 PDFRavi KumarNo ratings yet
- A Selective Summary of Psychopharmacology Research Published in First Half of 2017Document3 pagesA Selective Summary of Psychopharmacology Research Published in First Half of 2017gion.nandNo ratings yet
- Mahatme M S Et. Al., 2018Document6 pagesMahatme M S Et. Al., 2018kaniNo ratings yet
- New Drugs: Self-Test QuestionsDocument3 pagesNew Drugs: Self-Test QuestionscNo ratings yet
- Ann EmergDocument8 pagesAnn EmergDyan TonyNo ratings yet
- Pharmacological Sedation Management in Paediatric Intensive Care UnitDocument16 pagesPharmacological Sedation Management in Paediatric Intensive Care Unitfuka priesleyNo ratings yet
- RSI Post IntubationDocument8 pagesRSI Post IntubationshinjiNo ratings yet
- Ijpd 22 303Document6 pagesIjpd 22 303bellaNo ratings yet
- Chudnofsky 2000Document8 pagesChudnofsky 2000Sanjeewa de AlwisNo ratings yet
- E423 FullDocument11 pagesE423 FullCecepNo ratings yet
- Jurnal Efficacy and Tolerability of Adjunctive Lacosamide in Pediatric Patients With Focal SeizuresDocument15 pagesJurnal Efficacy and Tolerability of Adjunctive Lacosamide in Pediatric Patients With Focal SeizuresAnida HasnaNo ratings yet
- Phase 1 A Randomized Double Blind Placebo Controlled Study of The Safety Tolerability Pharmacokinetics and Pharmacodynamics of LB 102 July 2022 Springer NatureDocument10 pagesPhase 1 A Randomized Double Blind Placebo Controlled Study of The Safety Tolerability Pharmacokinetics and Pharmacodynamics of LB 102 July 2022 Springer Naturecm911No ratings yet
- Epilepsia - 2018 - Maglalang - Rescue Therapies For Seizure Emergencies New Modes of AdministrationDocument9 pagesEpilepsia - 2018 - Maglalang - Rescue Therapies For Seizure Emergencies New Modes of AdministrationKikie Rizky HeningNo ratings yet
- MRX Clinical Alert-August 2018Document6 pagesMRX Clinical Alert-August 2018Nattawat TeerawattanapongNo ratings yet
- Analgesicos y Sedativos en UCI - BZD Propofol y OpioidesDocument19 pagesAnalgesicos y Sedativos en UCI - BZD Propofol y OpioidesManuel MontellanosNo ratings yet
- Refractory Epi ManagementDocument4 pagesRefractory Epi Managementjonniwal sanusiNo ratings yet
- 2020 Troy CefaleasManejo RTDocument6 pages2020 Troy CefaleasManejo RTJULIO CESAR CASTRO MURILLONo ratings yet
- Marketed New Drug Delivery Systems For Opioid Agonists/Antagonists Administration: A Rapid OverviewDocument8 pagesMarketed New Drug Delivery Systems For Opioid Agonists/Antagonists Administration: A Rapid OverviewFaradila Putri SoegiyonoNo ratings yet
- Schizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapyDocument13 pagesSchizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapydilaNo ratings yet
- Therapeutic Use of Medicinal Cannabis in Dif Ficult To Manage EpilepsyDocument3 pagesTherapeutic Use of Medicinal Cannabis in Dif Ficult To Manage EpilepsyEnrique Molina LeonNo ratings yet
- Abaya 2018Document6 pagesAbaya 2018Muhammad Imam NoorNo ratings yet
- Efek SedasiDocument5 pagesEfek Sedasidheva akilNo ratings yet
- Daughton - 2009 - Review of ADHD PharmacotherapiesDocument9 pagesDaughton - 2009 - Review of ADHD PharmacotherapiesRene LutherNo ratings yet
- Safety Update: Dverse Drug ReactionDocument6 pagesSafety Update: Dverse Drug ReactionWilliam ChandraNo ratings yet
- 2006-Long-Term Use of Oxcarbazepine Oral Suspension in Childhood Epilepsy - Open-Label Study PDFDocument6 pages2006-Long-Term Use of Oxcarbazepine Oral Suspension in Childhood Epilepsy - Open-Label Study PDFAnonymous bEwTSXJ1gNo ratings yet
- Mann, Mackay, Et Al.Document9 pagesMann, Mackay, Et Al.Paulina AlonsoNo ratings yet
- HCN 153Document9 pagesHCN 153Suck my dickNo ratings yet
- Modafinil and Armodafinil in Schizophrenia: Chittaranjan Andrade, MDDocument3 pagesModafinil and Armodafinil in Schizophrenia: Chittaranjan Andrade, MDbenedicte lewinNo ratings yet
- Dopamine Vs EpinephrineDocument11 pagesDopamine Vs EpinephrineAyiek WicaksonoNo ratings yet
- 105.basic Clin Pharma Tox - 2015 - Penninga - Adverse Events Associated With Flumazenil Treatment For The Management ofDocument8 pages105.basic Clin Pharma Tox - 2015 - Penninga - Adverse Events Associated With Flumazenil Treatment For The Management oftereNo ratings yet
- Wjem 13 01 26 PDFDocument9 pagesWjem 13 01 26 PDFMoises Vega RodriguezNo ratings yet
- Famacologia Da Epilepsia e Estado de Mal EpilepticoDocument15 pagesFamacologia Da Epilepsia e Estado de Mal Epilepticorafael rocha novaesNo ratings yet
- Disinhibition of Behaviors With Midazolam:: Report of A CaseDocument5 pagesDisinhibition of Behaviors With Midazolam:: Report of A CaserajtanniruNo ratings yet
- Pi Is 0149291820302836Document15 pagesPi Is 0149291820302836John SMithNo ratings yet
- Geriatric Pharmacotherapy PDFDocument6 pagesGeriatric Pharmacotherapy PDFverry aswardsNo ratings yet
- Antiepileptic Drugs-Best Practice Guidelines ForDocument38 pagesAntiepileptic Drugs-Best Practice Guidelines ForAbraham Escobedo MoratillaNo ratings yet
- KETODEXDocument5 pagesKETODEXBarbarita Alvarado CamposNo ratings yet
- AAP Emergencies Ped Drug Doses PDFDocument20 pagesAAP Emergencies Ped Drug Doses PDFUlvionaNo ratings yet
- Clonidine WeanDocument10 pagesClonidine WeanJorge HinojosaNo ratings yet
- STart StroppDocument1 pageSTart StroppHoang Mai NguyenNo ratings yet
- Antiemetic Drug Use in Children What The.3Document6 pagesAntiemetic Drug Use in Children What The.3Zafitri AsrulNo ratings yet
- Opioid and Benzodiazepine Weaning in Pediatric PatientsDocument25 pagesOpioid and Benzodiazepine Weaning in Pediatric PatientsMaverick 18No ratings yet
- Dex Review 2007Document11 pagesDex Review 2007Jackelyne VilelaNo ratings yet
- Methylprednisolone in West SyndromeDocument5 pagesMethylprednisolone in West SyndromeBandya SahooNo ratings yet
- Chapter 12Document59 pagesChapter 12Alif riadiNo ratings yet
- CPT 1435 PDFDocument17 pagesCPT 1435 PDFarramithaNo ratings yet
- Review of The Newer Antiepileptic Drugs PDFDocument28 pagesReview of The Newer Antiepileptic Drugs PDFnickyNo ratings yet
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceFrom EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceRating: 3 out of 5 stars3/5 (1)
- Delirium in The Intensive Care Unit Is Dexmedetomidine EffectiveDocument15 pagesDelirium in The Intensive Care Unit Is Dexmedetomidine EffectiveArgenis SalinasNo ratings yet
- MCPHS Drug Information QuestionDocument5 pagesMCPHS Drug Information QuestionG TeenaNo ratings yet
- Duncan Et Al-2018-Cochrane Database of Systematic ReviewsDocument150 pagesDuncan Et Al-2018-Cochrane Database of Systematic Reviewsluis.fe.gd84No ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- 2348 0548.190064 1Document8 pages2348 0548.190064 1Ankita MohtaNo ratings yet
- Manage Delirium in Critically Ill Patients Through Prevention, Early Diagnosis and Treatment PDFDocument6 pagesManage Delirium in Critically Ill Patients Through Prevention, Early Diagnosis and Treatment PDFPablo RamirezNo ratings yet
- Key Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SDocument2 pagesKey Points: Balanced Anesthesia in Small Animal Patients: Incorporating Cri'SAlejandro Estrada RiosNo ratings yet
- Picco Monitoring During Liver Transplantation For.701Document1 pagePicco Monitoring During Liver Transplantation For.701Chang TruNo ratings yet
- Textbook of Pediatric Dentistry-3rd EditionDocument18 pagesTextbook of Pediatric Dentistry-3rd EditionAnna NgNo ratings yet
- Comparison of Dexmedetomidine, Pethidine and Tramadol in The Treatment of Post-Neuraxial Anaesthesia ShiveringDocument6 pagesComparison of Dexmedetomidine, Pethidine and Tramadol in The Treatment of Post-Neuraxial Anaesthesia ShiveringabdulNo ratings yet
- Smith - S Anesthesia For Infants and Children (Eighth Edition) 2011-384-391Document8 pagesSmith - S Anesthesia For Infants and Children (Eighth Edition) 2011-384-391Alexiel BathoryNo ratings yet
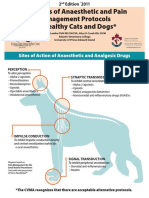
- Examples of Anaesthetic and Pain Management Protocols For Healthy Cats and DogsDocument3 pagesExamples of Anaesthetic and Pain Management Protocols For Healthy Cats and DogsEka FirmanNo ratings yet
- Dexmedetomidine: Pediatric Drug InformationDocument15 pagesDexmedetomidine: Pediatric Drug InformationАлексей НиколаевNo ratings yet
- Anestesia - Cardiovascular - Luna OrtizDocument11 pagesAnestesia - Cardiovascular - Luna OrtizWeimar Andres Bonilla MosqueraNo ratings yet
- Post-Operative Pain: Mechanisms and ManagementDocument6 pagesPost-Operative Pain: Mechanisms and ManagementDevana MaelissaNo ratings yet
- Management of Sedation and Delirium in Ventilated ICU PatientsDocument35 pagesManagement of Sedation and Delirium in Ventilated ICU PatientsJheng-Dao YangNo ratings yet
- General Management in ICUDocument8 pagesGeneral Management in ICUNurzawani Shamsudin67% (3)
- General Topics: Anesthesia, Analgesia, and Sedation of Small MammalsDocument23 pagesGeneral Topics: Anesthesia, Analgesia, and Sedation of Small Mammalsdoja catNo ratings yet
- Awake Intubation: David Leslie BSC (Hons) MBBCH (Hons) Frca Mark Stacey MB Mchir Frca Ilthe MSC (Med Ed)Document4 pagesAwake Intubation: David Leslie BSC (Hons) MBBCH (Hons) Frca Mark Stacey MB Mchir Frca Ilthe MSC (Med Ed)Fadilah SorayaNo ratings yet
- Anesthesia For Craniotomy - UpToDateDocument47 pagesAnesthesia For Craniotomy - UpToDateAna Belén Artero CastañoNo ratings yet
- Anesthetic Considerations For Geriatric DogsDocument3 pagesAnesthetic Considerations For Geriatric DogsFernanda PérezNo ratings yet
- Stanford Anesthesia - CA1 Tutorial Book PDFDocument63 pagesStanford Anesthesia - CA1 Tutorial Book PDFKhamini Dilly Kannan100% (1)
- Anesthesia and Analgesia Book 2Document186 pagesAnesthesia and Analgesia Book 2Diana NiculaeNo ratings yet
- TivaDocument38 pagesTivasunny kumar100% (1)
- SA Anesthesia Drug Dosages 2022Document3 pagesSA Anesthesia Drug Dosages 2022KRLITHIU Borja100% (1)
- ISAPS News Letter 2018Document52 pagesISAPS News Letter 2018Man Koon Suh, M.D.No ratings yet
- Out of Operating Room Anesthesia - A Comprehensive Review-Springer International Publishing (2017)Document467 pagesOut of Operating Room Anesthesia - A Comprehensive Review-Springer International Publishing (2017)Tahseen Talib100% (1)
- Drug Literature Assignment FINALDocument6 pagesDrug Literature Assignment FINALToqa ElmansouryNo ratings yet