Download as pdf or txt
You might also like
- Dubai's Golden SandsDocument17 pagesDubai's Golden SandsscrbdfanNo ratings yet
- Nature of PlanningDocument2 pagesNature of Planningjaanaan92% (24)
- Oral Notes Rupesh PillaiDocument172 pagesOral Notes Rupesh PillaiRachit100% (4)
- 66 Job Interview Questions For Data ScientistsDocument10 pages66 Job Interview Questions For Data ScientistsRavi RanjanNo ratings yet
- Tele Rehabilitation Service Delivery Journey From Prototype To Robust in Home Use D and R OnlineDocument10 pagesTele Rehabilitation Service Delivery Journey From Prototype To Robust in Home Use D and R OnlineFelipe Palma UrrutiaNo ratings yet
- Person-Generated Health Data in Simulated Rehabilitation Using Kinect For Stroke: Literature ReviewDocument12 pagesPerson-Generated Health Data in Simulated Rehabilitation Using Kinect For Stroke: Literature ReviewBey AlivandNo ratings yet
- Personalization of Mobile Health ApplicationsDocument6 pagesPersonalization of Mobile Health ApplicationsojuNo ratings yet
- Awareness, Perception and Acceptability of Digital Physiotherapy Intervention Among Malaysian PhysiotherapistDocument7 pagesAwareness, Perception and Acceptability of Digital Physiotherapy Intervention Among Malaysian PhysiotherapistIJPHSNo ratings yet
- Fog-Centric IoT Based Framework For Healthcare Monitoring Management and Early Warning SystemDocument12 pagesFog-Centric IoT Based Framework For Healthcare Monitoring Management and Early Warning SystemVidya NeemuNo ratings yet
- Painreports 7 E1026Document11 pagesPainreports 7 E1026Luisa OsorioNo ratings yet
- Hir 24 387Document7 pagesHir 24 387salad.ass420420No ratings yet
- Bigdata Oriented Multimedia Mobile Health ApplicationsDocument10 pagesBigdata Oriented Multimedia Mobile Health ApplicationsChRinaldoNo ratings yet
- Abdulelah Albukhari Capstone Final-CompressedDocument21 pagesAbdulelah Albukhari Capstone Final-Compressedapi-529533386No ratings yet
- Health Monitoring Using Internet of Things (Iot)Document5 pagesHealth Monitoring Using Internet of Things (Iot)Tanusri GhoshNo ratings yet
- Paper Su Case Study Medicina Lotti PontederaDocument2 pagesPaper Su Case Study Medicina Lotti PontederaronnyNo ratings yet
- Proposal For An Implementation Framework For DigitDocument18 pagesProposal For An Implementation Framework For DigitAndréNo ratings yet
- Digital Health Intervention For Stress and Anxiety ReliefDocument19 pagesDigital Health Intervention For Stress and Anxiety ReliefFiorel Loves EveryoneNo ratings yet
- Embodia - McMaster 2023Document69 pagesEmbodia - McMaster 2023JocelynNo ratings yet
- AI RehabilitaciónDocument21 pagesAI RehabilitaciónLuz CoronadoNo ratings yet
- JPM 14 00522 v2Document9 pagesJPM 14 00522 v2PHONG LÊ BÁNo ratings yet
- AI RehabilitaciónDocument11 pagesAI RehabilitaciónLuz CoronadoNo ratings yet
- Aarogya Margdarsh - Medical Camp Related Mobile AppDocument5 pagesAarogya Margdarsh - Medical Camp Related Mobile AppInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CHN1 Lec Session #22 SASDocument8 pagesCHN1 Lec Session #22 SASRetiza EllaNo ratings yet
- INFORMATICSDocument12 pagesINFORMATICSColene PadojinogNo ratings yet
- User Evaluation of A Novel SMS-based Reminder System For Supporting Post-Stroke RehabilitationDocument11 pagesUser Evaluation of A Novel SMS-based Reminder System For Supporting Post-Stroke RehabilitationnindyaNo ratings yet
- Health ExpertDocument6 pagesHealth ExpertIJRASETPublicationsNo ratings yet
- Wearable Computing in Shaping Digital HealthDocument18 pagesWearable Computing in Shaping Digital HealthAmoghNo ratings yet
- Palliative-care-providers-use-of-digital-health-and-perspectives-on-technological-innovation-a-national-study_2021_BioMed-Central-LtdDocument10 pagesPalliative-care-providers-use-of-digital-health-and-perspectives-on-technological-innovation-a-national-study_2021_BioMed-Central-LtdArturo Carrasco HenaoNo ratings yet
- Newtrendsinmedicalsurgical Nursing Salwa HagagDocument30 pagesNewtrendsinmedicalsurgical Nursing Salwa HagagMalathi VarnaNo ratings yet
- Part B: The Feasibility and Acceptability of Mi SMART, A Nurse-Led Technology Intervention For Multiple Chronic ConditionsDocument10 pagesPart B: The Feasibility and Acceptability of Mi SMART, A Nurse-Led Technology Intervention For Multiple Chronic Conditionsindah sundariNo ratings yet
- Integration of IoT and Fog Computing in Healthcare Based The Smart Intensive UnitsDocument13 pagesIntegration of IoT and Fog Computing in Healthcare Based The Smart Intensive UnitsHajaros RegraguiNo ratings yet
- CHN1 Lec Session #22 SASDocument9 pagesCHN1 Lec Session #22 SASspooderm4nNo ratings yet
- Digital TechnologiesDocument12 pagesDigital TechnologiesAbhijit PalitNo ratings yet
- Comparative Health Technology Assessment of Robotic-AssistedDocument9 pagesComparative Health Technology Assessment of Robotic-AssistedDanica SavićNo ratings yet
- Get M365Document17 pagesGet M365kiritoblackswordsmen07No ratings yet
- Artigo Mobile SaúdeDocument12 pagesArtigo Mobile SaúdeNathielle AlvesNo ratings yet
- Contemporary Nursing-The E Nurse Part 2Document11 pagesContemporary Nursing-The E Nurse Part 2Damie OjoNo ratings yet
- Rehabilitation System For Stroke Patients Using Mixed-Reality and Immersive User InterfacesDocument5 pagesRehabilitation System For Stroke Patients Using Mixed-Reality and Immersive User InterfaceskirubhaNo ratings yet
- 1 s2.0 S2405844020300190 MainDocument9 pages1 s2.0 S2405844020300190 MainAlex KwokNo ratings yet
- Research Journal PublicationDocument5 pagesResearch Journal Publicationgraphic designerNo ratings yet
- 1st Paper PDFDocument4 pages1st Paper PDFsathvikNo ratings yet
- Shti160 0376Document5 pagesShti160 0376Althea Marie AlmadenNo ratings yet
- The Role of Physical Therapists in Introducing Assis-Tive Products For The Home-Bound Elderly DisabledDocument3 pagesThe Role of Physical Therapists in Introducing Assis-Tive Products For The Home-Bound Elderly DisabledKanika BhaskarNo ratings yet
- Cloud GloveDocument7 pagesCloud GloveDaniel EkassiNo ratings yet
- Remote Health Monitoring of Elderly Through Wearable SensorsDocument26 pagesRemote Health Monitoring of Elderly Through Wearable SensorsAkansha SinghNo ratings yet
- ICTs & Digital HealthDocument7 pagesICTs & Digital Healthvicechancellor ofstudentaffairsNo ratings yet
- Internet of Things For In-Home Health Monitoring Systems: Current Advances, Challenges and Future DirectionsDocument11 pagesInternet of Things For In-Home Health Monitoring Systems: Current Advances, Challenges and Future DirectionsEleni maruNo ratings yet
- Telerehabilitación en FT MusculoesueléticaDocument7 pagesTelerehabilitación en FT MusculoesueléticaEveling VerbelNo ratings yet
- Digitalization in Nursing ServicesDocument4 pagesDigitalization in Nursing ServicesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jennifer Bautista A.K.A. Minah Bautista A.K.A. Mildred Narvarte A.K.A. Malinda Sirue A.K.ADocument24 pagesJennifer Bautista A.K.A. Minah Bautista A.K.A. Mildred Narvarte A.K.A. Malinda Sirue A.K.AmalindaNo ratings yet
- The Benefits and Challenges of Implementing Smart Hospital Projects A Systematic Review1Document8 pagesThe Benefits and Challenges of Implementing Smart Hospital Projects A Systematic Review1Apriani KudiNo ratings yet
- Computers in Industry: Sophie Huey-Ming Guo, Her-Kun Chang, Chun-Yi LinDocument8 pagesComputers in Industry: Sophie Huey-Ming Guo, Her-Kun Chang, Chun-Yi LinALmirdhad LatarissaNo ratings yet
- Design and Implementation of Medicine Reminder Box and Health CheckerDocument6 pagesDesign and Implementation of Medicine Reminder Box and Health CheckerIJRASETPublications100% (1)
- Telemedicina 2Document7 pagesTelemedicina 2Michelle VillalvaNo ratings yet
- An Rticle For FInal Exam - PhysiotheraphyDocument3 pagesAn Rticle For FInal Exam - PhysiotheraphyFaika NabilaNo ratings yet
- Information Technology and Community HealthDocument18 pagesInformation Technology and Community HealthDj Gwyn MandigmaNo ratings yet
- Artificial Intelligence in Medical Application: Electrical and Electronic Engineering DepartmentDocument18 pagesArtificial Intelligence in Medical Application: Electrical and Electronic Engineering Departmentمهيمن الابراهيميNo ratings yet
- A Software To Prevent DeliriumDocument7 pagesA Software To Prevent DeliriumConstanza DeviaNo ratings yet
- Telehealth: A Cutting Edge Tool For Healthcare DeliveryDocument4 pagesTelehealth: A Cutting Edge Tool For Healthcare DeliveryIJAR JOURNALNo ratings yet
- 3 - Adnan Khan - Challenges Facing Application IoTDocument17 pages3 - Adnan Khan - Challenges Facing Application IoTAzka SalsabilaNo ratings yet
- Patient Satisfaction With Telehealth Vs Inperson Hand Therapy A Retrospective Review of Results of An Online Satisfaction SurveyDocument7 pagesPatient Satisfaction With Telehealth Vs Inperson Hand Therapy A Retrospective Review of Results of An Online Satisfaction Surveyanita awNo ratings yet
- Human Fitness ApplicationDocument6 pagesHuman Fitness ApplicationIJRASETPublicationsNo ratings yet
- ArticleDocument11 pagesArticleJimena ChavezNo ratings yet
- Healthcare Information Technology for Cardiovascular Medicine: Telemedicine & Digital HealthFrom EverandHealthcare Information Technology for Cardiovascular Medicine: Telemedicine & Digital HealthAmi B. BhattNo ratings yet
- Neuropsychological Functioning of Individuals at CDocument16 pagesNeuropsychological Functioning of Individuals at Candromeda.godoyNo ratings yet
- Kwan 2018Document7 pagesKwan 2018andromeda.godoyNo ratings yet
- Current Practique of CognitiveDocument21 pagesCurrent Practique of Cognitiveandromeda.godoyNo ratings yet
- A Sistematic ReviewDocument8 pagesA Sistematic Reviewandromeda.godoyNo ratings yet
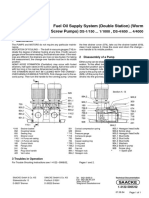
- Fuel Oil Supply System (Double Station) (Worm Screw Pumps) : DS 1/150 ... 1/1000, DS 4/650 ... 4/4000Document1 pageFuel Oil Supply System (Double Station) (Worm Screw Pumps) : DS 1/150 ... 1/1000, DS 4/650 ... 4/4000徐玉坤No ratings yet
- Hypogear 85W-140 - BP Aust Pty LTDDocument4 pagesHypogear 85W-140 - BP Aust Pty LTDBiju_PottayilNo ratings yet
- Dwnload Full Organization Development The Process of Leading Organizational Change 4th Edition Anderson Test Bank PDFDocument35 pagesDwnload Full Organization Development The Process of Leading Organizational Change 4th Edition Anderson Test Bank PDFliamhe2qr8100% (15)
- Vol.11 Issue 46 March 23-29, 2019Document32 pagesVol.11 Issue 46 March 23-29, 2019Thesouthasian TimesNo ratings yet
- NOC Video Walls Solutions - 4!10!2021 Rالبريد1Document2 pagesNOC Video Walls Solutions - 4!10!2021 Rالبريد1Sayed HamedNo ratings yet
- Macquarie University:: 1.) Musec SchoolDocument6 pagesMacquarie University:: 1.) Musec SchoolUtsav ShroffNo ratings yet
- The 60 MM Diameter Solid Shaft Is Subjected To The... PDFDocument3 pagesThe 60 MM Diameter Solid Shaft Is Subjected To The... PDFxy2h5bjs27No ratings yet
- Altagamma Bain Worldwide Market Monitor - Update 2019 PDFDocument15 pagesAltagamma Bain Worldwide Market Monitor - Update 2019 PDFHaider RazaNo ratings yet
- ToyotaDocument4 pagesToyotasunny837No ratings yet
- Homeland Security Thesis StatementDocument8 pagesHomeland Security Thesis Statementdwtcn1jq100% (2)
- Emd-Mi927 IntercoolerDocument8 pagesEmd-Mi927 IntercoolerVictor Raul Tobosque MuñozNo ratings yet
- Oracle Demand Management Cloud DsDocument6 pagesOracle Demand Management Cloud DsmrssabaNo ratings yet
- 6.1 - Distribution Riser Support Cat DDocument3 pages6.1 - Distribution Riser Support Cat DHeather HertzNo ratings yet
- Building SpecificationsDocument5 pagesBuilding Specificationsjologscresencia100% (1)
- Accounting ResearchDocument6 pagesAccounting ResearchAnne PanghulanNo ratings yet
- Cut List Cheat SheetDocument1 pageCut List Cheat SheetmeredithNo ratings yet
- Radio MirchiDocument7 pagesRadio MirchiRahul KasliwalNo ratings yet
- QUIZ 3 Financial Forecasting and BudgetingDocument9 pagesQUIZ 3 Financial Forecasting and BudgetingPRINCESS HONEYLET SIGESMUNDONo ratings yet
- Dr. N.P SheteDocument28 pagesDr. N.P SheteMD Noyon IslamNo ratings yet
- Input Data Required For Pipe Stress AnalysisDocument4 pagesInput Data Required For Pipe Stress Analysisnor azman ab aziz100% (1)
- Introduction To Surface EngineeringDocument31 pagesIntroduction To Surface Engineeringlogeshboy007No ratings yet
- Final Report (NTCC) IoTDocument11 pagesFinal Report (NTCC) IoTSyed MehsherNo ratings yet
- Group 8 Design Main Report + Appendix (1) 1 400Document400 pagesGroup 8 Design Main Report + Appendix (1) 1 400Manishaa Varatha RajuNo ratings yet
- A Hybrid Intrution Detection Approach Based On Deep LearningDocument16 pagesA Hybrid Intrution Detection Approach Based On Deep LearningVictor KingbuilderNo ratings yet
- Course Syllabus Electrical Machines II Summer SemesterDocument4 pagesCourse Syllabus Electrical Machines II Summer SemesterMahmoud Alshar'eNo ratings yet
- Chap 6-Supply, Demand & Government PoliciesDocument30 pagesChap 6-Supply, Demand & Government PoliciesKhánh AnNo ratings yet