Download as pdf or txt
You might also like
- Review of Pediatrics and NeonatologyDocument609 pagesReview of Pediatrics and NeonatologyJansi Arul100% (3)
- Vol9 Issue1 06Document4 pagesVol9 Issue1 06annisaNo ratings yet
- Systematic Review of Firsttrimester Ultrasound Screening For Detection of Fetal Structural Anomalies and Factors Affecting Screening PerformanceDocument14 pagesSystematic Review of Firsttrimester Ultrasound Screening For Detection of Fetal Structural Anomalies and Factors Affecting Screening PerformanceMariana B.No ratings yet
- Screening For Congenital AnomaliesDocument7 pagesScreening For Congenital AnomaliesFamilia CieletNo ratings yet
- DR Ogunwale A.N Ufm UnitDocument37 pagesDR Ogunwale A.N Ufm UnitzumarockNo ratings yet
- Screening For Fetal Chromosomal AbdnormalitiesDocument22 pagesScreening For Fetal Chromosomal AbdnormalitiesAlejandra MurilloNo ratings yet
- Reviewed - IJANS-Recent Antenatal Investigations For Better Pregnancy OutcomesDocument4 pagesReviewed - IJANS-Recent Antenatal Investigations For Better Pregnancy Outcomesiaset123No ratings yet
- m857 PDFDocument11 pagesm857 PDFMini PGNo ratings yet
- 2004, Vol.31, Issues 1, Ultrasound in ObstetricsDocument213 pages2004, Vol.31, Issues 1, Ultrasound in ObstetricsFebrinata MahadikaNo ratings yet
- Prenatal DiagnosisDocument22 pagesPrenatal DiagnosishusshamNo ratings yet
- Controversies in Perinatal Medicine The Fetus As A Patient 26 Bioethical Aspects of Ultrasonographic and Invasive Prenatal DiagnosisDocument9 pagesControversies in Perinatal Medicine The Fetus As A Patient 26 Bioethical Aspects of Ultrasonographic and Invasive Prenatal DiagnosisZiel C EinsNo ratings yet
- ECPM2016 ABSTRACTBOOKTheJournalofMaternal-FetalNeonatalMedicine PDFDocument314 pagesECPM2016 ABSTRACTBOOKTheJournalofMaternal-FetalNeonatalMedicine PDFDiana-Elena ComandasuNo ratings yet
- 10 1111@jog 143436777777Document17 pages10 1111@jog 143436777777Epiphany SonderNo ratings yet
- Embarazo EctopicoDocument10 pagesEmbarazo EctopicocfsaludNo ratings yet
- Sof MarkersDocument21 pagesSof MarkersHari NairNo ratings yet
- NIH Public Access: Author ManuscriptDocument21 pagesNIH Public Access: Author ManuscriptanyNo ratings yet
- Cell Free Dna Acog 2012Document3 pagesCell Free Dna Acog 2012gs2710No ratings yet
- Desi Rahayu (153112540120468Document53 pagesDesi Rahayu (153112540120468Bella FebriyantiNo ratings yet
- Prenatal Genetic Screening DBiagnosis Hamamy 2010Document27 pagesPrenatal Genetic Screening DBiagnosis Hamamy 2010Georgie StephenNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundHartanto LieNo ratings yet
- Acta Obstet Gynecol Scand - 2013 - SKR Stad - A Randomized Controlled Trial of Third Trimester Routine Ultrasound in ADocument8 pagesActa Obstet Gynecol Scand - 2013 - SKR Stad - A Randomized Controlled Trial of Third Trimester Routine Ultrasound in ADayang fatwarrniNo ratings yet
- Prenatal DiagnosisDocument42 pagesPrenatal DiagnosisarunjyothishNo ratings yet
- PDFDocument137 pagesPDFPeter Osundwa KitekiNo ratings yet
- FMT 4 3 3Document5 pagesFMT 4 3 3kimsrfforensicmedicineNo ratings yet
- Cervical Length Measurement Using An Improvised Cervicometer As A Predictor of Spontaneous Preterm BirthDocument6 pagesCervical Length Measurement Using An Improvised Cervicometer As A Predictor of Spontaneous Preterm BirthImarie RamosNo ratings yet
- The Diagnostic Performance of The Ductus Venosus For The DetectionDocument17 pagesThe Diagnostic Performance of The Ductus Venosus For The DetectionEdwin BravoNo ratings yet
- Prenatal Diagnosis JyDocument33 pagesPrenatal Diagnosis Jyjien_yeenNo ratings yet
- v13 p74 EthicalDocument7 pagesv13 p74 EthicalVincent FloraNo ratings yet
- Frequency of Preterm Labor and Its Factors in Patients Presenting To Secondary Care HospitalDocument6 pagesFrequency of Preterm Labor and Its Factors in Patients Presenting To Secondary Care HospitalJohn WickNo ratings yet
- Overview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateDocument27 pagesOverview of Ultrasound Examination in Obstetrics and Gynecology - UpToDateRopiNo ratings yet
- Fetal Aneuploidy - Screening and Diagnostic TestingDocument8 pagesFetal Aneuploidy - Screening and Diagnostic TestingAngela FernandezNo ratings yet
- Basics of Fetal EchocardiographyDocument58 pagesBasics of Fetal Echocardiographyrk vNo ratings yet
- 3-Invasive or Non-Invasive Prenatal Genetic.Document4 pages3-Invasive or Non-Invasive Prenatal Genetic.Egnilton RamosNo ratings yet
- Dario Update NIPTconsensusstatement 5 Sept 13393Document2 pagesDario Update NIPTconsensusstatement 5 Sept 13393Marios SkarmoutsosNo ratings yet
- Performance of Fetal, Perinatal, and Pediatric AutopsiesDocument6 pagesPerformance of Fetal, Perinatal, and Pediatric AutopsiesbeosroNo ratings yet
- Prenatal Screening SOGCDocument13 pagesPrenatal Screening SOGCBrendaNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticlefeyzarezarNo ratings yet
- OBST aNALISIS-DE-LONGITUD-CERVICAL-Y-RIESGOYDocument6 pagesOBST aNALISIS-DE-LONGITUD-CERVICAL-Y-RIESGOYEduardo Agustín Vargas CamposNo ratings yet
- Aust NZ J Obst Gynaeco - 2014 - Doan - The Timing of Elective Caesarean Deliveries and Early Neonatal Outcomes in SingletonDocument8 pagesAust NZ J Obst Gynaeco - 2014 - Doan - The Timing of Elective Caesarean Deliveries and Early Neonatal Outcomes in SingletonEbenezer AbrahamNo ratings yet
- Medical Record Validation of Maternally Reported History of PreeclampsiDocument7 pagesMedical Record Validation of Maternally Reported History of PreeclampsiezaNo ratings yet
- PRENATAL TESTING VVVDocument44 pagesPRENATAL TESTING VVVmhmtrgnn67No ratings yet
- 2016 Article 211Document25 pages2016 Article 211agus fetal mein feraldNo ratings yet
- 2021 Article 1541Document6 pages2021 Article 1541bintangNo ratings yet
- Sagesorg-Guidelines For The Use of Laparoscopy During PregnancyDocument32 pagesSagesorg-Guidelines For The Use of Laparoscopy During PregnancyLuis Acosta CumberbatchNo ratings yet
- Antipsikotik Pregnancy 3Document9 pagesAntipsikotik Pregnancy 3ThalNo ratings yet
- How Does SubchorionicDocument8 pagesHow Does SubchorionicNovi Nurlaeli Dwi PutriNo ratings yet
- Jurnal Onko RiaDocument13 pagesJurnal Onko RiaMuzdatul KhairiahNo ratings yet
- Transvaginal Ultrasonography and Female InfertilityDocument76 pagesTransvaginal Ultrasonography and Female InfertilityDavid MayoNo ratings yet
- Doi 10.4297/najms.2010.2468Document7 pagesDoi 10.4297/najms.2010.2468Bayu Surya DanaNo ratings yet
- Ultrasound in Prenatal DiagnosisDocument11 pagesUltrasound in Prenatal DiagnosisValentina Grajales RestrepoNo ratings yet
- The Journal of Maternal-Fetal & Neonatal Medicine: To Cite This ArticleDocument8 pagesThe Journal of Maternal-Fetal & Neonatal Medicine: To Cite This ArticleBerry BancinNo ratings yet
- Routine Prenatal Ultrasonography As A Screening ToolDocument17 pagesRoutine Prenatal Ultrasonography As A Screening ToolYulia MufidahNo ratings yet
- Data Mining Approach in Preterm Birth Prediction: Jyothi ThomasDocument13 pagesData Mining Approach in Preterm Birth Prediction: Jyothi ThomasAnonymous Fs8SOuNo ratings yet
- Impact of Oligohydramnios On Maternal and PerinataDocument6 pagesImpact of Oligohydramnios On Maternal and PerinataDiana SchlittlerNo ratings yet
- Sav Chev 2014Document8 pagesSav Chev 2014Nguyễn Cao VânNo ratings yet
- A Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthDocument5 pagesA Case Control Study of Risk Factors and Neonatal Outcomes of Preterm BirthSarahí SosaNo ratings yet
- 03mb01 4Document3 pages03mb01 4matchman_headNo ratings yet
- Jurnal Placenta PreviaDocument9 pagesJurnal Placenta Previasheva25No ratings yet
- Prenatal Diagnosis: Secondary ArticleDocument17 pagesPrenatal Diagnosis: Secondary ArticlegeraldersNo ratings yet
- 2023 Cervical Cancer Guidance AACCDocument21 pages2023 Cervical Cancer Guidance AACCeuniceNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Pre-Final Obg PaperDocument1 pagePre-Final Obg PapervineelainjetyNo ratings yet
- 1970411271mendelian Laws of InheritanceDocument27 pages1970411271mendelian Laws of InheritancevineelainjetyNo ratings yet
- Project Results & GraphsDocument46 pagesProject Results & GraphsvineelainjetyNo ratings yet
- Front Page For RegisterDocument5 pagesFront Page For RegistervineelainjetyNo ratings yet
- Nursing 3012Document6 pagesNursing 3012vineelainjetyNo ratings yet
- Clinical Procedure Manual Section 23 RespiratoryDocument38 pagesClinical Procedure Manual Section 23 RespiratoryvineelainjetyNo ratings yet
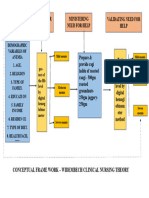
- Conceptual Frame WorkDocument1 pageConceptual Frame WorkvineelainjetyNo ratings yet
- Research Chapter WiseDocument21 pagesResearch Chapter WisevineelainjetyNo ratings yet
- CVADocument6 pagesCVAvineelainjetyNo ratings yet
- G NewexamDocument25 pagesG NewexamvineelainjetyNo ratings yet
- Initial Query FormDocument3 pagesInitial Query FormvineelainjetyNo ratings yet
- 20230930104647MSC Nursing Prospectus 2023-24Document28 pages20230930104647MSC Nursing Prospectus 2023-24vineelainjetyNo ratings yet
- Legal and Ethical AspectsDocument33 pagesLegal and Ethical AspectsvineelainjetyNo ratings yet
- Metformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometDocument5 pagesMetformin, Glucophage, Glucophage XR, Glumetza, Fortamet, RiometAgronaSlaughterNo ratings yet
- Clinical Utility of Multiphasic Questionnaire MPQ - 39 42Document5 pagesClinical Utility of Multiphasic Questionnaire MPQ - 39 42DN100% (1)
- CMRF FundDocument3 pagesCMRF FundLovely ChetanNo ratings yet
- Elective 2 Lecture 1 Concept of IllnessDocument9 pagesElective 2 Lecture 1 Concept of IllnessMelchor Felipe Salvosa100% (1)
- The Cardiovascular System: Elaine N. MariebDocument151 pagesThe Cardiovascular System: Elaine N. Mariebwhiskers qtNo ratings yet
- DiabetesmanipurchakraDocument3 pagesDiabetesmanipurchakraBhavin VoraNo ratings yet
- Modified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineDocument5 pagesModified Duke's Criteria For Infective Endocarditis - Mnemonic - EpomedicineAsmaNo ratings yet
- Davao Doctors College Nursing Program Nursing Care PlanDocument6 pagesDavao Doctors College Nursing Program Nursing Care PlanSHINI0% (1)
- JC Severe Scrub TyphusDocument27 pagesJC Severe Scrub TyphusAakarsh RastogiNo ratings yet
- Science of HeartbreakDocument6 pagesScience of HeartbreakPrashanth JanakiramNo ratings yet
- Aplikasi Mikro Teori KolcabaDocument11 pagesAplikasi Mikro Teori KolcabaKing DonNo ratings yet
- 2008 With AnswersDocument40 pages2008 With AnswersNeelam AlizeeshanNo ratings yet
- NURS 627 Case Study PaperDocument11 pagesNURS 627 Case Study PaperJaclyn Strangie100% (4)
- Gen Med Revision PDF 5Document107 pagesGen Med Revision PDF 5sharen100% (3)
- Clinical Review October 20 2017 - SHINGRIXDocument158 pagesClinical Review October 20 2017 - SHINGRIXPayneMaxNo ratings yet
- ClozetestgatDocument9 pagesClozetestgatnongnee23No ratings yet
- Assignment On Burns 2Document15 pagesAssignment On Burns 2Suby Beigh100% (3)
- Exams & Answers1Document207 pagesExams & Answers1Nwwff Al HhloaNo ratings yet
- Enoxaparin - Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin - Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Medical Nutrition Therapy For Burns: Leny Budhi Harti, S.GZ, M.Si - MedDocument36 pagesMedical Nutrition Therapy For Burns: Leny Budhi Harti, S.GZ, M.Si - Medfina26No ratings yet
- Resume Esmaeil ImaniDocument2 pagesResume Esmaeil ImaniSepideh MirzaeiNo ratings yet
- The Risks vs. Benefits of Face Masks - Is There An Agenda - Children's Health DefenseDocument7 pagesThe Risks vs. Benefits of Face Masks - Is There An Agenda - Children's Health DefenseAndrew LatorcaiNo ratings yet
- M-i-M For DME Matrix-In-A-Matrix Technique For Deep Margin ElevationDocument5 pagesM-i-M For DME Matrix-In-A-Matrix Technique For Deep Margin Elevationfernando vicente100% (1)
- Berg 2012Document7 pagesBerg 2012Mario Espinosa GamezNo ratings yet
- Questions and Answers: Varicella (Chickenpox)Document3 pagesQuestions and Answers: Varicella (Chickenpox)MENU A/P MOHANNo ratings yet
- Telmisartan+Amlodipine 31 MMHG in 1 WeekDocument10 pagesTelmisartan+Amlodipine 31 MMHG in 1 WeekPoogle111No ratings yet
- MIT20 441JF09 Quiz3 SampleDocument4 pagesMIT20 441JF09 Quiz3 SampleGuilherme HenriqueNo ratings yet
- Metabolic Acidosis: Irish Grace A. Dayao Dra. RamosDocument14 pagesMetabolic Acidosis: Irish Grace A. Dayao Dra. RamosBing DayaoNo ratings yet
- Infanrix-Hexa SMPC 09 2020Document15 pagesInfanrix-Hexa SMPC 09 2020walkrogNo ratings yet