Volume 9, Issue 1, January – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
A 50-Year-Old Female with Quadriparesis
Secondary to Viral Myositis: Unusual
Presentation and Diagnostic Approach
1
Dr. Dnyanesh Morkar, 2Dr. Saad Siddiqui, 3Dr. Priyanka Patil
Department of General Medicine,
KLE Academy of Higher Education & Research,
Belagavi, India
Abstract:- It’s not common to encounter acute viral own after a week of symptoms starting when healing starts.
myositis that occurs during convalescence from illness, However, reports of rhabdomyolysis with renal failure and
most commonly influenza. Myalgia with weakness and compartment syndrome are documented. (5) Typical symptoms
isolated laboratory finding of elevated serum creatine in adults are characterized by muscle pain and severe
kinase (CK) are hallmarks of this disease. The disease is weakness in the proximal muscles of the upper extremity,
often thought to occur only in children with male which resolve slowly over weeks rather than days. (6) Viral and
predominance and weakness predominantly in calf postinfectious myositis in adults are uncommon but have been
muscles. Recovery usually takes a few days and is usually reported with influenza, mononucleosis, cytomegalovirus
spontaneous. This case therefore indicates that it can occur infection, echovirus 9, and viral hepatitis. (1)
in adults with atypical presentation. Close differentials are
inflammatory and hereditary myopathies which require Muscle fibre degeneration and myonecrosis with
subjecting patients to unnecessary invasive testing. It is leukocyte infiltration are the pathological hallmarks of muscle
well proven in numerous studies that invasive testing such biopsy (7) But paediatricians know that invasive tests are futile.
(8,3)
as muscle biopsy has no role in treatment as well as By taking into account the typical clinical and laboratory
prognosis in cases like benign acute pediatric myositis, findings of this disease and identifying more serious
therefore physicians should be aware of such cases and pathological conditions that should be ruled out, benign acute
avoid unnecessary anxiety-provoking and invasive testing. childhood myositis can be diagnosed. This can prevent
unnecessary diagnostic tests and can ensure an excellent
Keywords:- Quadriparesis, Viral Myositis, Diagnostic prognosis for patients. (3)
Approach, Biopsy.
II. CASE DESCRIPTION
I. INTRODUCTION
A 50-year-old female patient, a resident of rural
Multiple viruses are linked with acute myositis, with Karnataka (India) and, a farmer by occupation presented to the
influenza being the most common. (1) Influenza B is more ER with complaints of truncal weakness associated with
likely to cause myositis due to the presence of NB protein in weakness, pain and swelling of bilateral upper and lower limbs
the membrane than influenza A, which aids in viral entry and for one month. The patient gives a history of fever one month
may have a myotropic effect. (1,2) Since the viral agent has not back which lasted for two days associated with upper
consistently been detected in biopsy samples, it is unknown if respiratory tract symptoms and pain in large joints which was
this is the result of immunological mechanisms, myotoxic aggravated on activity and relieved on rest. The patient sought
cytokines, or direct viral infection of the muscle.. (1) treatment for the same from a local hospital in her village, and
symptoms were relieved for a few days.
Myositis is most common in children and only happens
in a tiny percentage of influenza patients (mean age of eight Three weeks before admission, the patient complained of
years), known as benign acute childhood myositis, possibly persistent pain in bilateral upper and lower extremities along
because of virus tropism for immature muscle cells, males are with soreness of her hand and legs, which was not relieved by
more commonly affected. (1) It is associated with a mild to medication restricting her movements.
moderate rise in serum creatine kinase levels (CK), lactate
dehydrogenase (LDH) and aspartate aminotransferase (AST). In the next two days, the patient noticed swelling in her
(3)
upper and lower extremities such that her clothes and bangles
became tight, and she was not able to put her feet in her
During the early stages of the virus' recovery, the most footwear.
common symptom of viral myositis is the abrupt onset of
muscle weakness, discomfort, and soreness. Symptoms are Two weeks before admission, she developed difficulty in
often limited to calf muscles, but other muscle group getting up from the squatting position and combing her hair.
involvement is also reported. (4) Usually, it goes away on its Weakness slowly progressed over the next week making her
IJISRT24JAN364 www.ijisrt.com 309
Volume 9, Issue 1, January – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
unable to eat, dress or undress by herself along with difficulty was no history of bowel or bladder involvement or a band-like
walking by herself. sensation, shooting pain, or involuntary movement/seizure-
like activity.
One week before admission, she could not get up from
lying down or roll in bed from side to side. There was no history of neurological illness or any other
comorbidity. There was no history of drug intake or significant
5 days before admission, she could not hold her neck family history. Her last COVID-19 vaccination dose was 6
upright and was then referred to us for further evaluation. months back.
On the day of admission, she was afebrile with stable On examination, she had a normal general physical
vitals. On further probing, there was no history of loss of examination apart from bilateral pedal edema extending to her
sensation, dysphagia, dysarthria, nasal regurgitation, facial thighs which was tender on touch. There was no rash or
asymmetry, diplopia, visual disturbances or headache. There subcutaneous nodule or any other neurocutaneous marker.
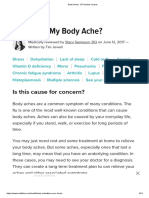
Table 1 Case Examination
Parameter Reference Range Admission Day 1 Day 3 Day 7 Day 15 Day 24
Haemoglobin (g/L) 12-15 17.2 17.5 12.0 11.3 12.2
PCV (%) 37-47 52.5 54.2 35.8 36.7 38.1
RBC (x 10^6/microL) 3.80-4.80 5.89 6.00 3.64 3.87 3.86
Platelets (x 10^3/microL) 150-450 339 314 189 199 239
Total Counts (x 10^3/microL) 4-10 18.13 17.80 18.34 11.93 9.93 6.89
Urea (mg/dl) 17-49 32 51 30 19 25
Serum Creatinine (mg/dl) 0.60-1.17 0.7 0.8 0.9 0.6 0.6
Total Bilirubin (mg/dl) 0.0-1.1 0.3 0.4 0.2 0.6 0.7
SGOT/AST (U/L) 0-35 1133 1298 187 27 25
SGPT/ALT (U/L) 0-45 352 375 311 18 16
Alk. Phosphatase 159 195 56 84 56
CPK (U/L) 20-180 - 3688 2194 9938 107
Sodium (mEq/L) 136-145 144 138 136 142 135 138
Potassium (mEq/L) 3.5-5.10 4.0 4.46 3.7 3.9 3.6 4.1
LDH 1524
Her higher mental function, cranial nerve examination, On day 3 of hospitalization, her serum cortisol levels
sensory examination, and reflexes were normal along with no were within normal range, ANA profile, myositis panel and
cerebellar signs, and intact cortical function with no signs of rheumatoid factor were sent, which was negative.
meningeal irritation. Although, there was a motor deficit in the
upper limb– shoulder (2/5), elbow (2/5), wrist (3/5), and finger Our differentials were myositis secondary to
(4/5) with poor handgrip. Her lower limb power – hip (1/5), autoimmune aetiology or viral aetiology, she was started on
knee (2/5), ankle (4/5) was present along with poor neck and steroid pulse therapy (Injection methylprednisolone 1g/day for
truncal flexion. 5 days) followed by tablet methylprednisolone 1mg/kg body
weight in a tapering manner for the next 4 weeks. If symptoms
On the day of presentation, she had raised haemoglobin recurred on a tapering dose of steroid, we would incline
levels of 17.2 g/dl (normal 12-15g/dl) with elevated hematocrit towards autoimmune aetiology.
of 52.5% (normal 36-46%) suggesting a dehydrated state,
along with elevated ALT of 352 U/L (normal 1-33 U/L) and On day 8 of hospitalization, her muscle power improved
AST of 1133 U/L (normal 1-32 U/L). Her total count was and by day 15, her liver function test normalized.
18.13 x 109/L (normal 4.5-11.0 x 109/L), and she was started
on IV antibiotics along with IV fluids to treat any superadded On day 24 of admission, her serum creatine kinase levels
infection and dehydration. Her HIV, Hepatitis B and Hepatitis were within normal limits (107 U/L), and she was discharged
C results came back negative. Dengue, leptospirosis and after 4 weeks of hospitalization with normal bilateral upper
typhoid were also ruled out. and lower limb power of 5/5.
On Day 2 of hospitalization, she had elevated serum III. DISCUSSION
creatine kinase levels of 3688 U/L along with an elevated LDH
value of 1524 U/L with normal serum PCT, thyroid profile, The case of a 50-year-old female presenting with a
serum electrolytes and urine examination. Diagnosis of gradually progressive weakness predominant in the truncal
myositis secondary to unknown etiology was made however region and bilateral proximal upper and lower limb muscles
any invasive testing like EMG, NCV or muscle biopsy was with no other abnormal central nervous system examination
deferred. along with elevated serum creatine kinase levels, deranged
IJISRT24JAN364 www.ijisrt.com 310
Volume 9, Issue 1, January – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
ALT, AST succeeding a fever episode with a prolonged diagnosis of benign viral myositis was first disregarded since
recovery time describes a disease remarkably similar to benign it was thought to be a condition that only affected children.
acute childhood myositis (BACM) in terms of onset during
convalescence phase of a viral illness, distribution of pain in A muscle biopsy was thus performed while it is not
limbs and elevated creatine kinase levels, however, it also useful for the diagnosis of benign acute childhood myositis
highlights the unique features such as the age and gender of which is following our theory of non-invasive diagnostic
the patient, time taken for onset of symptoms and recovery and algorithm. He also said that any inflammatory or genetic
the ability of diagnosis without the use of invasive tests such myopathy would have relapses. (8) Our case is also of the adult
as EMG and biopsies. age group, however, there are some differentiating features
such as the gender (female) and time duration of onset and
In 1955, LUNDBERG first described an illness that recovery, which is longer in our case. A causal infectious agent
started with high fever and headache. When the temperature was also not found in our case; however, it can be explained
nearly returns to normal and the headache subsides, usually as the search for a virus is done after the symptomatic period
after three to four days, the pain appears in the calf. It was when the pathogen has presumably been eliminated.
termed ‘myalgia cruris epidemica’ and was reported in 70
children and four adults, however later the adult cases were Scaber et al. in 2020 highlighted that in adults, proximal
overlooked and ‘myalgia cruris epidemica’ was renamed muscles of bilateral upper and lower limbs can be
benign acute childhood myositis. (9) Since then, many studies involved in an illness like BACM which resolves over weeks
have been carried out in the pediatric population and similar rather than days which is similar to our case where recovery
diseases in adults have been poorly understood, therefore took an entire month. Additionally, he hypothesises that the
understanding a case of an adult presenting with a similar most plausible explanation is that the virus directly causes
constellation of symptoms and laboratory values becomes muscle cell necrosis through its action on muscle cells, or that
important. the effects of the virus's immune response are responsible for
the short 3-day delay between the start of the flu-like sickness
A similar study done by Mackay et al. in 1999 described and the onset of neurological symptoms. (11)
benign acute myositis of childhood as a disorder of mid-
childhood (mean age of 8.1 years), typically affecting young Naylor et al did a study and found a usual presentation of
males. Symptoms include calf pain and difficulty walking after two female adults who presented with insidious onset bilateral
a viral illness with spontaneous recovery in one week. He also upper and lower limb weakness following an episode of viral
highlights that biopsy done revealed nonspecific degenerative infection, the latency period in each case was about 10-14 days
changes, focal muscle fibre vacuolation, and extensive muscle (about 2 weeks), with recovery taking few weeks rather than
necrosis, however, several biopsies did not show any days which is similar to our case where patient took around
inflammatory changes as the process of the disease is ‘patchy’ three weeks to develop a full constellation of symptoms and
and it is exceedingly rare to isolate influenza or other viruses recovered in one-month duration. He also says biopsy shows
from the muscle (10) which is in concordance with our approach features suggestive of necrosis and inflammation and rarely a
of refraining from invasive testing such as biopsy. virus has been isolated from a biopsy specimen (6) thereby
again proving the fact that even in cases which are atypical in
Initial investigation results of elevated CK, LDH, AST terms of duration, investigation like biopsy has no role to play
and ALT along with thorough history taking and clinical in treatment or prognosis. He also mentions two cases of
examination ruled out several causes of quadriparesis. They myositis secondary to viral infection where corticosteroids
inclined us towards the diagnosis of myositis of unknown were started, to which both patients responded well like our
aetiology, close differentials such as inflammatory, hereditary, case.
and metabolic causes were ruled out by a negative myositis
panel, negative ANA profile and a normal thyroid function A study done by Gibson et al. during the H1N1 epidemic
test. However, a similar conclusion was drawn by Neocleous of 2009 highlights the fact that H1N1 disproportionately
et al. in 2012 which emphasises that the correct diagnosis of affects younger and healthier patients when compared to
BACM is by evaluating the clinical and laboratory findings typical influenza, postulating that presentation depends on the
and by recognising other serious medical conditions, which strain of the virus. He also mentions that a negative muscle
must be excluded from the diagnosis by a detailed patient biopsy does not rule out viral myositis and therefore muscle
workup including a detailed CNS examination, blood biopsy is not routinely recommended in such cases. (12) This
investigations including serum CPK and CRP values and a does makes us wonder whether the atypical presentation in our
urinary analysis (to rule out rhabdomyolysis) are enough for case could be due to different strains of influenza prevalent at
the diagnosis and can avoid unnecessary diagnostic tests and the time in that geographical region or like epidemics of the
reassure parents and patients of a good prognosis. (3) past, the recent epidemic of COVID-19 has a lingering effect.
Chanson et al. in 2018 described a BACM-like illness in To answer our last question, more research on a wide
a 32-year-old patient with severe pain and oedema in both legs scale including more patients from different regions needs to
associated with lower extremity motor impairment, The be done.
biopsy of the left anterior tibial muscle showed necrosis and
muscle cell regeneration without inflammatory infiltration, the
patient recovered after a few days. According to him, the
IJISRT24JAN364 www.ijisrt.com 311
Volume 9, Issue 1, January – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
IV. INVESTIGATION REFERENCES
[1]. Crum-Cianflone NF. Bacterial, fungal, parasitic, and
viral myositis. Clin Microbiol Rev [Internet].
2008;21(3):473–94. Available from:
http://dx.doi.org/10.1128/CMR.00001-08
[2]. Betakova T, Nermut MV, Hay AJ. The NB protein is an
integral component of the membrane of influenza B
virus. J Gen Virol [Internet]. 1996;77 (Pt 11) (11):2689–
94. Available from: http://dx.doi.org/10.1099/0022-
1317-77-11-2689
[3]. Neocleous C, Spanou C, Mpampalis E, Xatzigeorgiou S,
Pavlidou C, Poulos E, et al. Unnecessary diagnostic
investigations in benign acute childhood myositis: a case
series report. Scott Med J [Internet]. 2012;57(3):182.
Available from:
http://dx.doi.org/10.1258/smj.2012.012023
[4]. Middleton P, Alexander R, Szymanski M. Severe
V. CONCLUSION myositis during recovery from influenza. Lancet
[Internet]. 1970;296(7672):533–5. Available from:
The patient presented with atypical presentation of a http://dx.doi.org/10.1016/s0140-6736(70)91343-7
disease which is like benign acute childhood myositis [5]. Carrillo-Esper R, Ornelas-Arroyo S, Pérez-Bustos E,
(BACM), the diagnosis was made based on a thorough history Sánchez-Zúñiga J, Uribe-Esquivel M. Rhabdomyolysis
taking ruling out an extensive list of differential diagnoses and acute renal failure in human influenza A H1N1
along with detailed physical examination including central mediated infection. Gac Med Mex. 2009;145(6):519–21.
nervous system examination and positive laboratory results. [6]. Naylor CD, Jevnikar AM, Witt NJ. Sporadic viral
After ruling out inflammatory causes of myositis, our myositis in two adults. CMAJ. 1987;137(9):819–21.
differential diagnosis was myositis secondary to viral vs [7]. Agyeman P, Duppenthaler A, Heininger U, Aebi C.
autoimmune cause. The decision of not subjecting our patient Influenza-associated myositis in children. Infection
to unnecessary invasive procedures like EMG, NCV and [Internet]. 2004;32(4):199–203. Available from:
muscle biopsy was made which would not have any significant http://dx.doi.org/10.1007/s15010-004-4003-2
difference to the treatment. Instead, the patient was given [8]. Chanson J-B, Dakayi C, Lannes B, Echaniz-Laguna A.
steroid pulse therapy followed by a tapering dose steroid Benign acute myositis in an adult patient. BMJ Case Rep
keeping in mind that any autoimmune cause would flare up on [Internet]. 2018;2018: bcr-2017-223493. Available
withdrawal of steroids. The patient responded well and made from: http://dx.doi.org/10.1136/bcr-2017-223493
a full recovery with 4 weeks of steroid therapy along with [9]. Lundberg Å. Myalgia cruris epidemica. Acta Paediatr
supportive care, aggressive physiotherapy and rehabilitation. [Internet]. 1957;46(1):18–31. Available from:
http://dx.doi.org/10.1111/j.1651-2227.1957.tb08627.x
The patient was followed up at 1 month, 3 months and 6 [10]. Mackay MT, Kornberg AJ, Shield LK, Dennett X.
months of duration, there was no evidence of any recurrence Benign acute childhood myositis: laboratory and clinical
with the patient able to carry out her usual activity without any features. Neurology [Internet]. 1999;53(9):2127–31.
difficulty, helping us retrospectively incline towards the Available from: http://dx.doi.org/10.1212/wnl.53.9.2127
diagnosis of myositis secondary to viral infection. [11]. Scaber J, Molyneux AJ, Buckley C, Webb AJS. Two
cases are reports of distal upper limb weakness following
influenza-like illness: an emerging pattern of para-
infectious myositis in adults. BMC Neurol [Internet].
2020;20(1):237. Available from:
http://dx.doi.org/10.1186/s12883-020-01821-1
[12]. Gibson SB, Majersik JJ, Smith AG, Bromberg MB.
Three cases of acute myositis in adults following
influenza-like illness during the H1N1 pandemic. J
Neurosci Rural Pract [Internet]. 2013;4(1):51–4.
Available from: http://dx.doi.org/10.4103/0976-
3147.105614
IJISRT24JAN364 www.ijisrt.com 312
You might also like
- Severe Sepsis and Septic Shock - Understanding A Serious Killer PDFDocument448 pagesSevere Sepsis and Septic Shock - Understanding A Serious Killer PDFCarkos MorenoNo ratings yet
- Optic Neuritis and COVIDDocument2 pagesOptic Neuritis and COVIDHamzeh AlsalhiNo ratings yet
- Avindra Nath Neurology 2023Document13 pagesAvindra Nath Neurology 2023FernandoNo ratings yet
- MuhammadMirzaRaziqBinMohdZailani DMS2223Document8 pagesMuhammadMirzaRaziqBinMohdZailani DMS2223Muhammad Mirza RaziqNo ratings yet
- When The Limp Has A Dietary Cause - A Retrospective Study On Scurvy in A Tertiary Italian Pediatric HospDocument9 pagesWhen The Limp Has A Dietary Cause - A Retrospective Study On Scurvy in A Tertiary Italian Pediatric HospgistaluvikaNo ratings yet
- Chikungunya Virus InfectionDocument35 pagesChikungunya Virus InfectionManny GabrielNo ratings yet
- Fulltext - Ams v5 Id1040Document4 pagesFulltext - Ams v5 Id1040yaneemayNo ratings yet
- Transverse Myelitis: Clinical PracticeDocument9 pagesTransverse Myelitis: Clinical PracticearnabNo ratings yet
- Late Presentation of Post Diphtheritic Myocarditis in A 15-Year MaleDocument3 pagesLate Presentation of Post Diphtheritic Myocarditis in A 15-Year MaleFaqih Alam RuqmanaNo ratings yet
- 2016 Hasan Et Al. - A Case Report of Mixed Connective Tissue Disease PDocument5 pages2016 Hasan Et Al. - A Case Report of Mixed Connective Tissue Disease PPratyay HasanNo ratings yet
- History of Polio-1Document21 pagesHistory of Polio-1world photocopyNo ratings yet
- Lecture Note of PathologyDocument73 pagesLecture Note of PathologyRafez JoneNo ratings yet
- 2019, Dijkstra Et Al, Myoclonus and Cerebellar Ataxia Pós Covid 19Document3 pages2019, Dijkstra Et Al, Myoclonus and Cerebellar Ataxia Pós Covid 19Carol PaesNo ratings yet
- ZikaVirus (1) (Repaired)Document4 pagesZikaVirus (1) (Repaired)ARISNo ratings yet
- 2.10.3 Joint and Bone InfectionsDocument9 pages2.10.3 Joint and Bone InfectionsZayan SyedNo ratings yet
- Attending Osteomyelitis ModuleDocument9 pagesAttending Osteomyelitis ModuleMrLarry DolorNo ratings yet
- Nepharites Lesson PlanDocument21 pagesNepharites Lesson Plansaritha Oruganti100% (1)
- Set C Long CovidDocument5 pagesSet C Long CovidHanggara SatrioNo ratings yet
- IDSA Osteomielite Vertebral Guideline 2015Document21 pagesIDSA Osteomielite Vertebral Guideline 2015Julia CarijoNo ratings yet
- An Approach To A Child With ArthritisDocument9 pagesAn Approach To A Child With Arthritispadamati govardhan reddy reddyNo ratings yet
- Zika VirusDocument5 pagesZika VirusStephanie Joy EscalaNo ratings yet
- Association Food Allergy Dried Fish Complex Regional Pain SyndromeDocument5 pagesAssociation Food Allergy Dried Fish Complex Regional Pain SyndromeSSR-IIJLS JournalNo ratings yet
- Association Food Allergy Dried Fish Complex Regional Pain SyndromeDocument5 pagesAssociation Food Allergy Dried Fish Complex Regional Pain SyndromeSSR-IIJLS JournalNo ratings yet
- Solitary Intramuscular Cysticercosis of Right Elbow RegionDocument7 pagesSolitary Intramuscular Cysticercosis of Right Elbow RegionIJAR JOURNALNo ratings yet
- Subscapularis Pyomyositis, A Rare Cause of Shoulder Pain, in A Patient Without Apparent Risk Factors: A Case ReportDocument8 pagesSubscapularis Pyomyositis, A Rare Cause of Shoulder Pain, in A Patient Without Apparent Risk Factors: A Case ReportSimon GrangeNo ratings yet
- Japanese Encephalitis (JE) : Lina PurnamasariDocument13 pagesJapanese Encephalitis (JE) : Lina PurnamasariLinaPurnamasariNo ratings yet
- RESEARCH PROPOSAL FinalDocument75 pagesRESEARCH PROPOSAL Finaldimi3895No ratings yet
- PenjasDocument4 pagesPenjasteni joharaNo ratings yet
- Journal Reading Survey OphtalmologyDocument17 pagesJournal Reading Survey OphtalmologynadyajondriNo ratings yet
- Infections of Cardiovascular Implantable Electronic Devices: Clinical PracticeDocument8 pagesInfections of Cardiovascular Implantable Electronic Devices: Clinical PracticeTha Vila Le ColloNo ratings yet
- Septic Arthritis: Nurul Hidayu - Nik Nor Liyana - Nurul HusnaDocument34 pagesSeptic Arthritis: Nurul Hidayu - Nik Nor Liyana - Nurul HusnaarifdeathsciethNo ratings yet
- Histopatho Lec - Assignment No. 1Document4 pagesHistopatho Lec - Assignment No. 1Manelli Faten BuenaventuraNo ratings yet
- Case Study 5 Dengue Fever CorrectedDocument13 pagesCase Study 5 Dengue Fever CorrectedyounggirldavidNo ratings yet
- Chikungunya - DINKES - RS UNAIR 22 November 2017Document24 pagesChikungunya - DINKES - RS UNAIR 22 November 2017Mojo PuskesmasNo ratings yet
- Labmed36 0419 PDFDocument5 pagesLabmed36 0419 PDFRahul K. JagaNo ratings yet
- 1st Cinical CaseDocument5 pages1st Cinical CasejoidaNo ratings yet
- A Rare Localization of Tuberculosis of The Wrist: The Scapholunate JointDocument4 pagesA Rare Localization of Tuberculosis of The Wrist: The Scapholunate JointtaufikolingNo ratings yet
- A. Introduction OsteomyelitisDocument10 pagesA. Introduction OsteomyelitisMa. Gina DerlaNo ratings yet
- CF Case No.2 Revised 55Document107 pagesCF Case No.2 Revised 55Wendell Gian GolezNo ratings yet
- Childhood Multisystem Inflammatory Syndrome With PDocument5 pagesChildhood Multisystem Inflammatory Syndrome With PGiska VelindaNo ratings yet
- NCM116 3NC3 Group3 CognitiveDisordersDocument11 pagesNCM116 3NC3 Group3 CognitiveDisordersCARLOS JOSETON PAOLO SANTIAGO TORRENo ratings yet
- ALS-Rot-4-meningococcemia (MOJICA, NOAH KENT)Document18 pagesALS-Rot-4-meningococcemia (MOJICA, NOAH KENT)Noah Kent MojicaNo ratings yet
- A Review On Hepatitis and Haemostasis: February 2018Document24 pagesA Review On Hepatitis and Haemostasis: February 2018Lydie Praxede EkoboNo ratings yet
- 1 s2.0 S2772973723009013 MainDocument8 pages1 s2.0 S2772973723009013 MainMDrakeNo ratings yet
- Jurnal Rheumatoid Arthritis - 6 PDFDocument4 pagesJurnal Rheumatoid Arthritis - 6 PDFJeanstepanisaragihNo ratings yet
- Applsci 11 08323Document8 pagesApplsci 11 08323atmokotomoNo ratings yet
- Ofx163 1546Document2 pagesOfx163 1546crisNo ratings yet
- MainDocument3 pagesMainomidazadmehr1375No ratings yet
- HHS Public Access: Varicella Zoster Virus InfectionDocument41 pagesHHS Public Access: Varicella Zoster Virus InfectionRiskaNo ratings yet
- Outline Writing - Group 14Document4 pagesOutline Writing - Group 14My NguyễnNo ratings yet
- Applied Therapeutic Ii FAR 454/3: Topic: MeningitisDocument14 pagesApplied Therapeutic Ii FAR 454/3: Topic: MeningitisgentamicinNo ratings yet
- Urinary Tract Infection Core Curriculum 2024Document11 pagesUrinary Tract Infection Core Curriculum 2024JESSICA VELAZQUEZNo ratings yet
- What Is Post-Viral Fatigue Syndrome, The Condition Affecting Some COVID-19 Survivors? - ABC NewsDocument6 pagesWhat Is Post-Viral Fatigue Syndrome, The Condition Affecting Some COVID-19 Survivors? - ABC NewsAnonymous zNdbKT993YNo ratings yet
- Ucu Iii Post Test July 4 2023 RatioDocument74 pagesUcu Iii Post Test July 4 2023 RatioVince C. MatamisNo ratings yet
- Diagnosis and Management of Spinal InfectionsDocument6 pagesDiagnosis and Management of Spinal Infectionsdr.maulanahutabaratNo ratings yet
- Case 3Document27 pagesCase 3Eduard GarchitorenaNo ratings yet
- CELLULITISSSDocument5 pagesCELLULITISSSLet BorlagdanNo ratings yet
- Necrotizing FasciitisDocument8 pagesNecrotizing FasciitisDra Maha HafezNo ratings yet
- Disease and ManDocument14 pagesDisease and ManTanesha JohnsonNo ratings yet
- Transverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandTransverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- AI Robots in Various SectorDocument3 pagesAI Robots in Various SectorInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyDocument8 pagesNurturing Corporate Employee Emotional Wellbeing, Time Management and the Influence on FamilyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnDocument3 pagesDynamic Analysis of High-Rise Buildings for Various Irregularities with and without Floating ColumnInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)Document7 pagesAn Explanatory Sequential Study of Public Elementary School Teachers on Deped Computerization Program (DCP)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionDocument9 pagesAnalysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Classifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningDocument8 pagesClassifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportDocument4 pagesDiode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsDocument14 pagesBreaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersDocument10 pagesMediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Organizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaDocument10 pagesOrganizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparison of JavaScript Frontend Frameworks - Angular, React, and VueDocument8 pagesComparison of JavaScript Frontend Frameworks - Angular, React, and VueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Disseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsDocument15 pagesDisseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingDocument15 pagesAn Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonDocument11 pagesOccupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Influence of Artificial Intelligence On Employment Trends in The United States (US)Document5 pagesThe Influence of Artificial Intelligence On Employment Trends in The United States (US)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Gender-Based Violence: Engaging Children in The SolutionDocument10 pagesGender-Based Violence: Engaging Children in The SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaDocument19 pagesThe Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingDocument8 pagesIntegrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pecha Kucha Presentation in The University English Classes: Advantages and DisadvantagesDocument4 pagesPecha Kucha Presentation in The University English Classes: Advantages and DisadvantagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Total Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationDocument11 pagesTotal Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Development of Creative Thinking: Case Study of Basic Design StudioDocument9 pagesDevelopment of Creative Thinking: Case Study of Basic Design StudioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarDocument4 pagesThe Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ibbs 2011 IndonesiaDocument80 pagesIbbs 2011 Indonesiarifka yoesoefNo ratings yet
- Medicalandmaintenance Treatmentsforvitiligo: Thierry PasseronDocument8 pagesMedicalandmaintenance Treatmentsforvitiligo: Thierry PasseronAro MandaNo ratings yet
- A Review of Malaysian Herbal Plants and Their ActiDocument20 pagesA Review of Malaysian Herbal Plants and Their ActiMuzan KibutsjiNo ratings yet
- Alexithymia Advances in Research Theory and Clinical Practice 1St Edition Olivier Luminet Online Ebook Texxtbook Full Chapter PDFDocument69 pagesAlexithymia Advances in Research Theory and Clinical Practice 1St Edition Olivier Luminet Online Ebook Texxtbook Full Chapter PDFarthur.fletcher883100% (16)
- Principles of Blood TransfusionDocument2 pagesPrinciples of Blood TransfusionGerardLum100% (3)
- Analysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolDocument3 pagesAnalysis of Volatile Organic Compounds in Exhaled Breath For Detection of Diabetes Mellitus and CholesterolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Writting Discussion TextDocument2 pagesWritting Discussion TextAditya Diyan100% (1)
- Executive Health Check Up Package - RSPI - Pondok Indah - 2023Document20 pagesExecutive Health Check Up Package - RSPI - Pondok Indah - 2023stephanymelody123No ratings yet
- Bosnia and HerzegovinaDocument2 pagesBosnia and HerzegovinaAnonymous G4VuCbNo ratings yet
- Beneficial Effect of Pachyrhizus Erosus Fiber As A Supplemental Diet To Counteract High Sugar-Induced Fatty Liver Disease in MiceDocument8 pagesBeneficial Effect of Pachyrhizus Erosus Fiber As A Supplemental Diet To Counteract High Sugar-Induced Fatty Liver Disease in MiceAdam Ryhan NoshikiNo ratings yet
- Revised HS360 ICICI Lombard Health Insurance PlanDocument29 pagesRevised HS360 ICICI Lombard Health Insurance PlanrbitrackerNo ratings yet
- Muhammad Alif Farhan - Journal Reading - VitiligoDocument27 pagesMuhammad Alif Farhan - Journal Reading - Vitiligomaliffarhan091No ratings yet
- Grade 7 NS Baseline 202022 2023Document2 pagesGrade 7 NS Baseline 202022 2023DIOSA N.CAPISTRANONo ratings yet
- Chapter 1 Suicide Learning From The Past To Improve The FutDocument109 pagesChapter 1 Suicide Learning From The Past To Improve The FutDr-Hope FaithNo ratings yet
- Microvascular Decompression Treatment For Trigeminal NeuralgiaDocument5 pagesMicrovascular Decompression Treatment For Trigeminal NeuralgiaAkmal Niam FirdausiNo ratings yet
- A Still-Face Paradigm For Young Children 212 YearDocument78 pagesA Still-Face Paradigm For Young Children 212 YearFannyNo ratings yet
- Body Aches - 15 Possible CausesDocument24 pagesBody Aches - 15 Possible Causesjbotha01No ratings yet
- Angel Hill's ThesisDocument45 pagesAngel Hill's ThesisJoan MelendresNo ratings yet
- Online Candidate Interview Form Education - OSHC (Rafael Bautista) PDFDocument2 pagesOnline Candidate Interview Form Education - OSHC (Rafael Bautista) PDFYaksá HiperbólicoNo ratings yet
- Glioma: ClassificationDocument2 pagesGlioma: ClassificationAppas SahaNo ratings yet
- Forta Super-Sweep Fine®: Safety Data SheetDocument5 pagesForta Super-Sweep Fine®: Safety Data Sheetnoe tellezNo ratings yet
- Psychiatry 1 Unit Topic 1 A History and Introduction To PsychiatryDocument11 pagesPsychiatry 1 Unit Topic 1 A History and Introduction To PsychiatryironbuangNo ratings yet
- Sexual SelfDocument2 pagesSexual SelfRoselle Razon100% (2)
- Prescriber Update 44 No.3 September 2023Document25 pagesPrescriber Update 44 No.3 September 2023Naeman GoetzNo ratings yet
- Giving To Others and The Association Between Stress and MortalityDocument7 pagesGiving To Others and The Association Between Stress and MortalityIonescu DanNo ratings yet
- Grade 8 Integrated Science Week 12 Lesson 2Document4 pagesGrade 8 Integrated Science Week 12 Lesson 2bettyboopmaingNo ratings yet
- Botanicals For Chronic Venous Insufficiency: Alternative and Complementary Therapies December 2007Document9 pagesBotanicals For Chronic Venous Insufficiency: Alternative and Complementary Therapies December 2007Анђела КостићNo ratings yet
- Dissertation Daniel GladowDocument7 pagesDissertation Daniel GladowWhereCanIFindSomeoneToWriteMyCollegePaperCharlesto100% (1)
- The Impact Pregnancy Have On Teenager English SBADocument2 pagesThe Impact Pregnancy Have On Teenager English SBAChrissyNo ratings yet
- New ScientistDocument60 pagesNew ScientistTrúc Phan Nguyên Thảo100% (1)