Professional Documents
Culture Documents
Nonpharmacological Interventions To Prevent Delirium
Nonpharmacological Interventions To Prevent Delirium
Uploaded by
juan.pablo.castroOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Nonpharmacological Interventions To Prevent Delirium
Nonpharmacological Interventions To Prevent Delirium
Uploaded by
juan.pablo.castroCopyright:
Available Formats
Feature
Nonpharmacological
Interventions to Prevent
Delirium: An Evidence-
Based Systematic Review
RYAN M. RIVOSECCHI, PharmD
PAMELA L. SMITHBURGER, PharmD, MS, BCPS
SUSAN SVEC, RN, BSN, CCRN
SHAUNA CAMPBELL, RN, BSN
SANDRA L. KANE-GILL, PharmD, MS
Development of delirium in critical care patients is associated with increased length of stay, hospital costs, and
mortality. Delirium occurs across all inpatient settings, although critically ill patients who require mechanical
ventilation are at the highest risk. Overall, evidence to support the use of antipsychotics to either prevent or
treat delirium is lacking, and these medications can have adverse effects. The pain, agitation, and delirium
guidelines of the American College of Critical Care Medicine provide the strongest level of recommendation
for the use of nonpharmacological approaches to prevent delirium, but questions remain about which non-
pharmacological interventions are beneficial. (Critical Care Nurse. 2015;35[1]:39-51)
elirium has a substantial impact on health care. This complication is associated with a
D 15-day increase in hospital length of stay (LOS),1 a financial impact of $4 billion to $16 billion
annually,2 and a 19% increase in 6-month mortality.3 Delirium is common across all patient
settings; the prevalence, however, varies according to acuity of illness. Delirium develops in general
medicine patients at rates ranging from 11% to 42%.4 The highest prevalence of delirium, as high as 87%,
occurs in critically ill patients.5 Understanding the impact of delirium on hospitalized patients makes
prevention and optimal treatment of this complication a priority. Two approaches are used to manage
delirium: use of pharmacological agents and application of nonpharmacological therapies.
CNE Continuing Nursing Education
This article has been designated for CNE credit. A closed-book, multiple-choice examination follows this article,
which tests your knowledge of the following objectives:
1. Describe the nursing literature on nonpharmacological interventions to prevent delirium
2. Discuss nonpharmacological interventions that have been shown to be effective in preventing delirium
3. Explain the tools developed for the measurement of delirium in intensive care unit patients
©2015 American Association of Critical-Care Nurses doi: http://dx.doi.org/10.4037/ccn2015423
www.ccnonline.org CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 39
The 2013 pain, agitation, and delirium guidelines6 of patients studied, one can reasonably assume that critically
the American College of Critical Care Medicine provide ill patients, who are at the highest risk for delirium, would
recommendations for the use of pharmacological agents also benefit from nonpharmacological interventions. Large
in the prevention and treatment of delirium. Because of randomized controlled trials with a multi-interventional
a lack of compelling data, the guidelines do not provide approach that includes pharmacological and nonphar-
a recommendation for a pharmacological protocol or for macological approaches to prevent delirium are needed.17
a combined nonpharmacological and pharmacological Any appropriate attempt at such a study requires a strong
protocol for prevention of delirium. Furthermore, the understanding of nonpharmacological approaches. The
guidelines give a -2C recommendation for pharmacologi- purpose of this systematic review is to summarize the
cal prevention with either haloperidol or atypical available literature on nonpharmacological management
antipsychotics. The lack of evidence supporting the use of delirium among all populations of patients. The ulti-
of pharmacological agents creates a void in the effective mate goal is to identify which strategies are beneficial to
management of delirium. facilitate the development of a nonpharmacological pro-
The guidelines6 give the highest grade within the tocol that could be implemented for critically ill patients.
delirium section (1B) to a nonpharmacological preven-
tion strategy, meaning the recommendation is a strong Methods
one backed by a moderate level of evidence. Unfortu- A literature search was completed by using MEDLINE
nately, most of the literature is on nonpharmacological and EMBASE. With PubMed, the following terms were
interventions used in either general medicine, geriatric, used to search MEDLINE for material from 1946 to
or perioperative patients.7-16 Although critically ill October 15, 2013: delirium AND (critically ill, intensive
patients certainly differ from most of the populations of care, ICU, intensive care unit, OR critical illness), AND
(treatment, prevention, prophylaxis, adjunctive therapy,
OR adjunct therapy). Additional searches in MEDLINE
Authors
were then performed with the terms (mobility, animation,
Ryan M. Rivosecchi is a second-year pharmacy resident in critical exercise, rehabilitation, physical therapy, OR bicycle),
care at the University of Pittsburgh Medical Center, Presbyterian (light, window, curtains, shades, OR blinds), (earplugs,
Hospital, Pittsburgh, Pennsylvania. ear, noise, OR hearing aid), (sleep, sleep hygiene, OR
Pamela L. Smithburger is an assistant professor of pharmacy and sleep deprivation), (eyeglasses, glasses, OR magnifying
therapeutics, University of Pittsburgh School of Pharmacy, Pittsburgh, lens), orientation, and hydration, each combined with
Pennsylvania, and a clinical specialist in the medical intensive care
unit at the University of Pittsburgh Medical Center, Presbyterian AND delirium, AND (critically ill, intensive care, ICU,
Hospital. intensive care unit, OR critical illness). EMBASE was
Susan Svec is the clinical director of the medical intensive care unit, searched by using the same strategy. The search was
University of Pittsburgh Medical Center, Presbyterian Hospital. She restricted to studies conducted in humans and reported
recently graduated from the master’s of leadership and administration
program at California University of Pennsylvania, California, in English. A second reviewer independently performed
Pennsylvania. the same search for validation. The titles of all citations
Shauna Campbell is the nursing director of the medical intensive care retrieved from the search were reviewed for relevance.
unit at the University of Pittsburgh Medical Center, Presbyterian On the basis of the relevance of the title, articles were
Hospital.
selected to be reviewed at the abstract level. Abstracts were
Sandra L. Kane-Gill is an associate professor of pharmacy and considered for full-text review if delirium was measured
therapeutics at the University of Pittsburgh School of Pharmacy.
She has secondary appointments in the School of Medicine in the as an outcome (incidence or severity), and the screening
Clinical Translational Science Institute, Department of Critical for delirium was completed by using a standardized screen-
Care Medicine, and the Department of Biomedical Informatics. ing tool. No further review of an abstract was done if the
She is also the critical care medication safety pharmacist at the Uni-
versity of Pittsburgh Medical Center in the Department of Pharmacy. study covered was not original research, addressed exclu-
Corresponding author: Sandra Kane-Gill, 918 Salk Hall, 3501 Terrace St, Pittsburgh, sively pharmacological approaches, or used a combination
PA 15261 (e-mail: slk54@pitt.edu). of pharmacological and nonpharmacological approaches.
To purchase electronic or print reprints, contact the American Association of Critical- If, after review, the abstract was still deemed applicable,
Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949)
362-2050 (ext 532); fax, (949) 362-2049; e-mail, reprints@aacn.org. a full-text review was done in which the same inclusion
40 CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 www.ccnonline.org
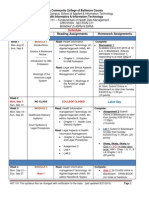
and exclusion criteria were applied
to the text of the article. No inclusion EMBASE MEDLINE
1540 citations 1104 citations
restrictions were placed on the study
setting or population of patients
(critically ill or not critically ill). Limit to English
and humans 821
Studies with mixed nonpharmaco-
logical interventions, including non- Titles screened for relevance
pharmacological protocols with
89 Selected for further
many interventions, were included. review of abstract
The exclusion of any involvement of Abstracts screened outcomes,
delirium screening, and pharmacological
pharmaceuticals was necessary to interventions
evaluate the true benefit of a non-
54 Selected
pharmacological protocol and mini- References for full-text
mize confounding variables. The reviewed for review 44 Excluded
inclusion ▪ 24 were not original research
references of the included articles ▪ 6 did not measure delirium or did not
were reviewed to ensure a compre- use standard delirium measurement
hensive assessment. 10 Included ▪ 5 contained pharmacological intervention
▪ 5 were not full-text articles
7 Included ▪ 4 did not involve an intervention
Results 17 Included
All Studies in review
A total of 17 articles7-24 met the
inclusion criteria and were selected Figure Breakdown of articles selected in literature search.
for review (see Figure and Tables 1
and 2). Seven studies18-24 were done
in critically ill patients, 5 in geriatric nonpharmacological intervention. Additionally, among
9-13 14-16
general medicine patients, 3 in postoperative patients, the 6 evaluations7-10,13,18 of the severity of delirium, all but
7,8
and 2 in patients who had a hip fracture. A total of 13 1 study9 indicated a reduction in severity. Patients’ LOS
of the studies were prospective investigations,7-11,13,15,16,18,21-24 was examined in 6 studies.7,8,11,18-20 Of the 6 studies, the
14-16,24
and 4 were randomized control trials. The Confusion results of 2 revealed a decrease in LOS.11,19 Among the 3
Assessment Method or the Confusion Assessment Method studies18-20
for the Intensive Care Unit (CAM-ICU) was the most fre- done in the Delirium is associated with multiple negative
quently used tool and was used in 10 studies.7-10,13,19-23 The ICU, only 1 consequences, including increased length
Neelon and Champagne Confusion Scale was used in 4 indicated a of stay, higher health care costs, and even
evaluations,14-16,24 and the Intensive Care Delirium Screen- reduction in increased mortality.
18 19
ing Checklist, the Diagnostic and Statistical Manual of LOS. When
12
Mental Disorders (Fourth Edition; DSM-IV), and the any outcome related to delirium (incidence, duration,
Delirium Screening Scale12 were each used once. The severity) was examined, only 2 studies11,19 did not show
frequency of delirium screening ranged from less than any benefit from the addition of a nonpharmacological
daily to 3 times per day. intervention.
The incidence of delirium was determined in 12 A total of 28 unique nonpharmacological interven-
studies.7-15,18-21 Among these, 9 revealed a benefit of the tions were used in the clinical studies. The most com-
nonpharmacological intervention.8-10,12-15,20,21 Table 3 gives mon interventions associated with any clinical benefit
the interventions used in the individual studies. Among were mobilization,8,10,20-23 reorientation,9,10,13,18,21 education
the interventions that were beneficial, the mean reduc- of nurses,7,10,12,18,23 and music therapy.9,16,18,20,21 A single
tion in the incidence of delirium was 24.7%, with a nonpharmacological intervention was examined in 5
7,8,10,11,22,23
range of 9.7% to 31.8%. In 6 studies, the dura- studies,12,14-16,24 and multiple nonpharmacological inter-
tion of delirium decreased after the addition of the ventions were examined in 12 investigations.7-10,11,13,18-23
www.ccnonline.org CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 41
Table 1 Studies included that involved patients who were not critically ill
Reference, Screening tool
year Design used (frequency) Population (N) Notable exclusions Nonpharmacological interventions
Milisen et al, 7
Prospective CAM, modified CAM Hip fracture, Nursing education
2001 emergency Poster in units
department/
trauma, (26)
Marcantonio Prospective, CAM (daily) Hip fracture, Metastatic cancer, Module: dehydration, dentures, nutrition
et al,8 2001 randomized, ≥ 65 years old life expectancy supplements, mobilization (physical/occu-
double-blind (126) < 6 months pational therapy), glasses, hearing aids,
clock, calendar, family presence
Inouye et al,9 Prospective, CAM (daily) General medicine, Inability to complete Protocol: orientation with care-team names
1999 individual > 70 years old interview, low risk and day’s schedule, cognitive stimulation
matching (852) for delirium activities, sleep protocol (warm drink,
relaxing music, back massage, noise
reduction, medication reschedule),
mobilization, visual aids, adaptive equipment,
hearing aids, hydration
Vidán et al,10 Prospective, CAM (daily) Geriatric unit, age Expected hospital Staff education
2009 controlled > 70 years (542) stay <48 hours Poster in units
Orientation: clock, calendar, reason for
admission, date, place, family letter
Glasses, hearing aids
Sleep: warm drink, reschedule medications
and procedures
Mobilization: out of bed, catheter removal,
change positions, avoid restraints
Hydration: schedule water if ratio of blood urea
nitrogen to serum level of creatinine > 40
Nutrition
Lundström Prospective DSM-IV criteria Age > 70 years, None Medical team education
et al,11 2005 (days 1, 3, and 7) geriatric unit (400) Reorganization of nursing staff
Tabet et al,12 Case-control, Delirium Rating Scale Age > 70 years, Patient not present Medical team education
2005 single-blind geriatric unit (250) on unit during
assessment
Caplan and Prospective CAM (every Age > 70 years, Severe dementia Reorientation
Harper,13 2007 other day) geriatric unit (37) Discharged within 48 Cognitive stimulation activities
MDAS for severity if hours Feeding assistance
CAM positive Hydration
Vision protocol
Hearing protocol
Ono et al,14 Randomized, NEECHAM (no com- Esophagectomy Bright light therapy
2011 randomized ment on how often) (22)
controlled trial
Taguchi et al,15 Prospective, NEECHAM Esophagectomy Bright light therapy
2007 randomized (twice a day) (11)
controlled trial
McCaffrey,16 Prospective, NEECHAM Hip or knee Music therapy
2009 randomized (daily for 3 days) surgery, > 75
controlled trial years old (22)
Abbreviations: CAM, Confusion Assessment Method; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition); LOS, length of stay;
MDAS, Memorial Delirium Assessment Scale; NEECHAM, Neelon and Champagne Confusion Scale.
42 CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 www.ccnonline.org
Outcomes Comments Antipsychotic use
No difference in incidence Used resource study nurses Not reported
3-day reduction in duration Screened only patients with CAM if NEECHAM identified them as
Reduction in the severity (2.94 points) high risk
No difference in LOS Screened only on days 1, 3, 5, and 8
18% reduction in incidence Recommendations by geriatric consultant based on module Yes
17% reduction in severity Recommendations not made if team was already doing them
1.2-day reduction in duration
No difference in LOS
5.1% reduction in incidence Less than 50% screened met inclusion criteria Not reported
56 fewer days delirious Used research nurses
28 fewer episodes Geared intervention against risk factors
No difference in severity Same medical team provided care to both groups
No difference in recurrence
6.8% reduction in incidence Must have risk factor for inclusion Not reported
0.4 decrease in severity Disposition to either geriatric or general medicine decided by
2.5-hour reduction in duration emergency department physician
No difference in recurrence Baseline characteristics not very similar
No difference in functional decline Note intervention more helpful in intermediate risk
No difference in death
No difference in prevalence at 24 and 72 hours Extensive nursing training for the intervention Not reported
4-day reduction in LOS
9.7% reduction in point prevalence of delirium Investigators had no role in day-to-day management Not reported
Use of daytime assessment and point prevalence could be
underestimated
31.8% reduction in incidence Patient must have 1 risk factor for enrollment Not reported
3.9-point reduction in MDAS score Mean intervention time 14-19 h/wk
Very small sample size
Cost analysis
31.7% reduction in prevalence Mean LOS 24.8 days Not reported
Two dropped out because light was too bright
All male population
Screening stopped on postoperative day 5
34% reduction in incidence at day 3 All male population Not reported
Decrease in delirium each of the 3 days All patients received standard pain, mobilization protocol Not reported
Music set to play 4 times a day for 1 hour; patients could do
more if they wished to
www.ccnonline.org CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 43
Table 2 Studies included that involved patients who were critically ill
Reference, Screening tool
year Design used (frequency) Population (N) Notable exclusions Nonpharmacological interventions
Skrobik et al, 18
Prospective ICDSC Medical-surgical Nursing education
2010 (3 times a day) ICU (1133) Radio or compact disc player, reorientation
Arenson et al,19 Randomized, CAM, CAM-ICU Cardiac surgery Inpatient death, Private room, no barriers
2013 cohort (3 times a day) (ICU/medicine) preexisting structural Windows
(1010) brain disease
Kamdar et al,20 Observational, CAM-ICU Medical ICU (300) Visual or hearing Sleep: minimize overhead page, turn off
2013 pre-post (2 times a day) impairment television, dim hallway, group care activities
design Open blinds
Prevent napping
Mobilization
Minimize caffeine before bed
Sleep: earplugs, eye mask, music
Colombo Prospective, CAM-ICU Medical-surgical Reorientation: follow mnemonic—use first
et al,21 2012 observational, (2 times a day) ICU (314) name, give information about location, LOS,
2 stage and illness
Clock
Read paper or book, music, radio
Reduction of night noise
Schweickert Prospective, CAM-ICU (daily) Medical ICU (104) Absent limbs, Mobilization, physical/occupational therapy
et al,22 2009 randomized 6-month mortality Passive range-of-motion exercises
<50%, cardiac arrest
Needham Prospective CAM-ICU (daily) Medical ICU (57) No exclusions Mobilization, physical/occupational therapy
et al,23 2010 Nursing education
Van Rompaey Prospective, NEECHAM (daily) ICU (136) Minimum score of Ear plugs
et al,24 2012 randomized 10 on Glasgow
controlled trial Coma Scale
Hearing impairment
Sedation
Abbreviations: CABG, coronary artery bypass graft; CAM, Confusion Assessment Method; ICDSC, Intensive Care Delirium Screening Checklist; ICU, intensive care unit;
LOS, length of stay; NEECHAM, Neelon and Champagne Confusion Scale; RASS, Richmond Agitation-Sedation Scale.
In 6 of those studies,8-10,13,20,21 the interventions were were used most often. All studies20-24 that included either
incorporated into a protocol. The mean number of mobilization or noise-reduction or sleep protocols indi-
interventions used per study was 4.1. cated a statistically significant benefit in at least 1 delirium-
related outcome.
ICU Studies
Of the 7 studies18-24 (Table 2) conducted in ICU patients, Discussion
6 investigations18,20-24 indicated a benefit in at least 1 ICU delirium is associated with numerous adverse
delirium-related outcome, including incidence, duration, consequences, ranging from increased cost to mortality.3,5
or severity. In the remaining study,19 a 0.6-day reduction As in a multitude of other ailments, prevention is the opti-
in ICU LOS occurred. Only 1 study18 indicated a reduction mal strategy, especially when effective treatment options
in subsyndromal delirium. In all but 1 study,24 more than are unavailable. Haloperidol has been studied for preven-
1 nonpharmacological intervention was used; mobiliza- tion and treatment of ICU delirium, but the results have
tion, a noise-reduction protocol, and a sleep protocol been inconclusive.25,26 Because of the unconvincing evidence
44 CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 www.ccnonline.org
Outcomes Comments Antipsychotic use
No difference in rate of delirium Hospital does not provide cardiac surgery or trauma care Yes
8.7% reduction in ICDSC score = 0 Nurses could give haldoperidol if ICDSC score > 3
8.4% reduction in subsyndromal delirium No difference in antipsychotic administered
No difference in LOS (patients with delirium)
No difference between environments Same anesthetic used Not reported
Day 3 median day of onset 63.9% underwent CABG, 71.7% men
0.6-day reduction in ICU LOS 6.2% delirium in < 65-year-olds vs 21.4% in > 65-year-olds
Baseline characteristics very different
5% increase in delirium-free or coma-free days Primary outcome delirium-coma combination according to Yes
20% reduction in incidence of delirium or coma CAM/RASS
No difference in ICU mortality Delirium secondary outcome
No difference in ICU LOS Compared ICU with post-ICU
Primarily respiratory failure patients
Primary outcome of sleep quality: no difference
13.5% reduction in incidence Used research nurses Yes
Mean onset on day 2 Standardized sedation protocol
Delirium increased ICU LOS by 2 days All treatment haloperidol or olanzapine
Medical ICU significantly higher rates of delirium
Midazolam use hazard ratio of 2.145
2-day reduction in ICU delirium days All patients received mechanical ventilation Yes
24% decrease in ICU time with delirium Less than 10% of patients in medical ICU included
13% decrease in hospital days with delirium Delirium a secondary outcome
8% reduction in days delirious Inclusion was mechanical ventilation ≥ 4 days Not reported
32% increase in days not delirious Routine delirium screening not part of standard care before
24% decrease in days unable to assess project started
No delirium assessments on 15 (pre) and 28 (post) patient days
2-point reduction on NEECHAM score NEECHAM scorer blinded to use of ear plugs Not reported
25% reduction when delirium and mild confusion Lowest NEECHAM score used for calculation of incidence
grouped together
for pharmacological management of delirium, nonphar- in medical ICU patients receiving mechanical ventilation,
macological strategies need to be further evaluated. and the results showed benefits for all outcomes evaluated.
The nonpharmacological intervention specifically The onus then switches to the development of a
discussed in the pain, agitation, and delirium guidelines6 nonpharmacological protocol to prevent delirium, but
of the American College of Critical Care Medicine is the ideal protocol has not yet been developed. One start-
early mobilization. Our review fully supports this recom- ing point would be to use the known risk factors for
mendation, and we think early mobilization should be delirium and target interventions to patients who have
included, when feasible, in any nonpharmacological these risk factors. This strategy was used by Inouye et al,9
prevention protocols implemented across all practice who created a standardized protocol to combat 6 risk
settings. Some type of mobilization was used in 6 stud- factors: cognitive impairment, sleep deprivation, immo-
ies,8,10,20-23 and 4 of the types8,10,20,21 were included in proto- bility, visual impairment, auditory impairment, and
cols with many interventions. The 2 studies22,23 in which dehydration. The observational PRE-DELIRIC (PREdic-
mobilization was not part of a protocol were conducted tion of DELIRium in ICu patients) study27 was done in
www.ccnonline.org CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 45
Table 3 Interventions showing benefita
Minimization of caffeine before bed
Medication/procedure reschedule
Avoidance of restraints
Dim hallways at night
Cognitive stimulation
Adaptive equipment
Nursing education
Catheter removal
Hearing protocol
Noise reduction
Visual displays
Daily schedule
Back massage
Reorientation
Light therapy
Eye protocol
Open blinds
Warm drink
Reference
Hydration
Eye mask
Dentures
Nutrition
Calendar
Mobility
Family
Music
7 X X Clock
8 X X X X X X X X X
18 # # #
9 X X X X X X X X X X X X X
10 X X X X X X X X X X X X X
20 # # # # # # #
21 # # # # # #
22 #
23 # #
12 X
13 X X X X X X
14 X
15 X
24 #
16 X
a Key: X, trial in patients who were not critically ill; #, trial in critically ill patients.
an ICU, and multivariate logistic regression analysis that encompassed 10 modules with at least 2 recommen-
indicated that 10 of the 25 risk factors evaluated were dations to be made for each module. Collectively, 31
predictive of delirium. Unfortunately, the majority of recommendations potentially could have been used.
the predictors, such as age and scores on the Acute Implementation of the appropriate recommendations
Physiology and Chronic Health Evaluation II, were for each patient resulted in one of the largest reductions
characteristics in both incidence and severity of delirium. Vidán et al10
Implementation of the appropriate that could not also used a multicomponent intervention and had results
recommendations for each patient be altered by similar to those of Marcantonio et al.8 The inevitable
resulted in one of the largest reductions use of a follow-up question becomes, Is a certain aspect of these
in both incidence and severity of delirium. nonpharmaco- multicomponent interventions leading to the positive
logical inter- results, and, if so, what aspect?
vention. Although creation of a protocol based on risk The importance of a protocol that includes multiple
factors is an excellent starting point, efforts must be interventions is evident when the outcomes of studies with
directed toward modifiable health care–associated 2 or fewer interventions7,11,12,14-16,18,19,22-24 are compared with
exposures and not nonmodifiable susceptibilities. the outcomes of studies with many interventions.8-10,13,20,21
Protocols with many interventions would be needed For incidence of delirium, the multi-interventional pro-
in order to include the many risk factors for delirium tocols resulted in a 15.9% mean reduction, whereas those
identified through the literature and to combat each fac- with 2 or fewer interventions showed an 11% reduction.
tor appropriately. Marcantonio et al8 attempted to devise The 11% reduction is slightly misleading because 4 of the
such a protocol. They developed a geriatric consultation 11 studies7,11,18,19 with 2 or fewer interventions did not
46 CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 www.ccnonline.org
indicate any difference in the incidence of delirium, studies must include use of a standardized screening
whereas all 6 of the multi-interventional studies8-10,13,20,21 tool, preferably either the CAM-ICU or the Intensive
indicated a reduction in incidence of at least 5.1%. Care Delirium Screening Checklist, to allow accurate
Another strategy, included in 6 studies,7,10-12,18,23 was interpretation of the impact of any future interventions
extensive education of nurses. The specifics of the educa- or protocol.
tion were typically not reported, but the material tended
to focus on the effects of delirium, screening for delirium, Implications for Critical Care Nurses
and, at times, implementation of the investigators’ pro- Although we reviewed of studies of both critically ill
tocol. This strategy was used as the sole intervention in and non–critically ill patients, we think that a variety of
2 studies.11,12 Milisen et al7 used education of nurses and interventions that benefit patients who are not critically
prominent display of educational material, both of which ill would still be useful in an ICU. The evidence shows
resulted in no difference in the incidence of delirium or that targeting interventions to prevent or treat known
the LOS, but a positive reduction in both the duration risk factors for delirium have the greatest benefit (eg,
and the severity of delirium. Tabet et al12 concentrated cognitive stimulation, reorientation), and a great deal
on an education-only strategy for both nurses and of overlap exists between risk factors for both critically
physicians and reported a 9.7% reduction in the point- and non–critically ill patients. A wide variety of patients
prevalence of delirium. However, the investigators used are treated in ICUs, and the variety of specialized ICUs
the Delirium Rating Scale, a screening tool that is not can be as unique as the patients treated within the units.
recommended in the guidelines6 of the American College For these reasons, strong consideration should be given
of Critical Care Medicine. Whether or not the results to having ICUs implement nonpharmacological inter-
would be the same if either the Intensive Care Delirium ventions that have been beneficial for patients who were
Screening Checklist or the CAM-ICU were used is not not critically ill.
clear. Last, Lundström et al11 used a similar strategy but Multicomponent intervention protocols to combat
also included a reorganization of the nursing staff. These delirium have proved beneficial. On the basis of guideline
investigators noted no difference in the prevalence of recommendations and the strength of literature, these
delirium at 24 or 72 hours. Patients in the study were protocols should include early mobilization, education
tested for delirium by using the DSM-IV on hospital days of nurses, and cognitive stimulation with reorientation.
1, 3, and 7. Because the DSM-IV is a set of diagnostic Depending on the severity of a patient’s illness, a variety
criteria and not a delirium screening tool, whether or of ways can
not these results can reliably be compared with the be used to All studies that included mobilization,
results of other studies in which screening for delirium accomplish noise-reduction, or sleep protocols displayed
was used is unclear.12 early mobi- a benefit in the reduction of delirium.
We would be remiss if we did not address the notion lization.
that perhaps the best protocol simply involves high-level Mobilization can be as complete as full physical or occu-
nursing care. Most of the unique interventions used in pational therapy treatments or merely passive range-of-
the studies reviewed could be easily incorporated into motion exercises. Bedside nurses and other members of
everyday nursing for every patient regardless of the the medical team work together to decide the level of
patient’s risk factors for delirium. Notable exceptions mobilization a patient can complete. Additionally, nurses
would be early mobility, nutrition, and catheter removal. can advocate for removal of tubes, catheters, or restraints
An inability to determine if certain aspects of a newly that may prevent early mobilization.
implemented protocol were already routine nursing Second, education of nurses is an essential component
practice before the protocols were implemented is a lim- of the success of any new intervention or initiative. The
itation of most published studies of nonpharmacological literature describes a variety of strategies for educating
interventions. Unfortunately, a study that could indicate nurses, including didactic lectures, visual displays, and
a true level of the benefit of each intervention would not one-on-one sessions. In order to include the potentially
be feasible, because such a study would require nurses large number of nurses who need to be educated, educa-
to stop providing standard care. Additionally, any future tion should be directed at all types of learners.28,29 Last,
www.ccnonline.org CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 47
cognitive stimulation and reorientation is a rather broad early mobility in any protocol created. ICU staff should
term that allows each nurse to develop a strategy that assemble a multidisciplinary team to review interven-
works for him or her. Still, each nurse’s intervention tions of known benefit to determine which ones can be
should incorporate a few key components, such as implemented within the staff ’s specific unit. CCN
determining how the patient would like to be addressed, Financial Disclosures
frequent reorientation to date and time, providing updates None reported.
on the patient’s schedule and clinical status, and convers-
ing with the patient in a manner that requires memory
Now that you’ve read the article, create or contribute to an online discussion
recall by the patient. about this topic using eLetters. Just visit www.ccnonline.org and select the article
you want to comment on. In the full-text or PDF view of the article, click
The implementation of a new intervention or initiative “Responses” in the middle column and then “Submit a response.”
is often met with resistance to change. In order to mini-
mize this resistance, obtaining nurses’ acceptance of and
willingness to support the change becomes imperative. To learn more about caring for patients with delirium, read
One strategy to eliminate high levels of resistance is to “Impact of a Delirium Screening Tool and Multifaceted Education
on Nurses’ Knowledge of Delirium and Ability to Evaluate It
educate nurses about the dangers and implications of Correctly” by Gesin et al in the American Journal of Critical Care,
the development of delirium while stressing that patients January 2012;21:e1-e11. Available at www.ajcconline.org.
become increasingly difficult to care for once delirium
occurs. Another frequent reason for resistance is an References
1. Salluh JI, Soares M, Teles JM, et al; Delirium Epidemiology in Critical
overall lack Care Study Group. Delirium epidemiology in critical care (DECCA):
Multicomponent protocols targeting of time during an international study. Crit Care. 2010;14(6):R210. doi:10.1186/cc9333.
2. Pun BT, Ely EW. The importance of diagnosing and managing ICU
known risk factors for delirium appear to the nursing delirium. Chest. 2007;132(2):624-636.
3. Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortal-
have benefits over single interventions. shift to add ity in mechanically ventilated patients in the intensive care unit. JAMA.
additional 2004;291(14):1753-1762.
4. Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium
tasks to be completed; however, most interventions we in medical in-patients: a systematic literature review. Age Ageing. 2006;
35(4):350-364.
have mentioned in this review could be worked into a 5. Balas MC, Rice M, Chaperon C, Smith H, Disbot M, Fuchs B. Management
nurse-implemented protocol that would require no more of delirium in critically ill older adults. Crit Care Nurse. 2012;32(4):15-26.
6. Barr J, Fraser GL, Puntillo K, et al; American College of Critical Care Med-
than 5 to 10 minutes per nursing shift to accomplish. icine. Clinical practice guidelines for the management of pain, agitation,
and delirium in adult patients in the intensive care unit. Crit Care Med.
Assembling a multidisciplinary team (physician, nurse, 2013;41(1):263-306.
pharmacist, and respiratory therapist) to determine 7. Milisen K, Foreman MD, Abraham IL, et al. A nurse-led interdisciplinary
intervention program for delirium in elderly hip-fracture patients. J Am
which nonpharmacological interventions are feasible Geriatr Soc. 2001;49(5):523-532.
within each specific unit is important. Ultimately the 8. Marcantonio ER, Flacker JM, Wright RJ, Resnick NM. Reducing delirium
after hip fracture: a randomized trial. J Am Geriatr Soc. 2001;49(5):516-522.
success of a nonpharmacological protocol to prevent 9. Inouye SK, Bogardus ST Jr, Charpentier PA, et al. A multicomponent
intervention to prevent delirium in hospitalized older adults. N Engl J
delirium lies with the bedside nurses, who have the Med. 1999;340(9):669-676.
most frequent contact with patients. 10. Vidán MT, Sánchez E, Alonso M, Montero B, Ortiz J, Serra JA. An inter-
vention integrated into daily clinical practice reduces the incidence of
delirium during hospitalization in elderly patients. J Am Geriatr Soc.
2009;57(11):2029-2036.
Conclusion 11. Lundström M, Edlund A, Karlsson S, Brännström B, Bucht G,
Use of nonpharmacological interventions is essential Gustafson Y. A multifactorial intervention program reduces the dura-
tion of delirium, length of hospitalization, and mortality in delirious
for the prevention of delirium. These interventions can patients. J Am Geriatr Soc. 2005;53(4):622-628.
12. Tabet N, Hudson S, Sweeney V, et al. An educational intervention can
be a low-risk, low-cost strategy that has shown a benefit prevent delirium on acute medical wards. Age Ageing. 2005;34(2):152-156.
in most studies. Nonpharmacological therapy also has 13. Caplan GA, Harper EL. Recruitment of volunteers to improve vitality in
the elderly: the REVIVE study. Intern Med J. 2007;37(2):95-100.
the potential to decrease the off-label use of antipsychotics 14. Ono H, Taguchi T, Kido Y, Fujino Y, Doki Y. The usefulness of bright
light therapy for patients after oesophagectomy. Intensive Crit Care Nurs.
for the treatment of delirium. The largest challenge in 2011;27(3):158-166.
developing a nonpharmacological protocol is determin- 15. Taguchi T, Yano M, Kido Y. Influence of bright light therapy on postop-
erative patients: a pilot study. Intensive Crit Care Nurs. 2007;23(5):289-297.
ing what interventions to include. Although a “one-size- 16. McCaffrey R. The effect of music on acute confusion in older adults
after hip or knee surgery. Appl Nurs Res. 2009;22:107-112.
fits-all” protocol may not be available, a strong body of 17. Khan BA, Zawahiri M, Campbell NL, et al. Delirium in hospitalized
evidence supports the inclusion of education of the med- patients: implications of current evidence on clinical practice and future
avenues for research—a systematic evidence review. J Hosp Med. 2012;
ical team, reorientation with cognitive stimulation, and 7(7):580-589.
48 CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 www.ccnonline.org
18. Skrobik Y, Ahern S, Leblanc M, Marquis F, Awissi DK, Kavanagh BP. The effect of earplugs during the night on the onset of delirium and
Protocolized intensive care unit management of analgesia, sedation, sleep perception: a randomized controlled trial in intensive care patients.
and delirium improves analgesia and subsyndromal delirium rates Crit Care. 2012;16(3):R73.
[published correction appears in Anesth Analg. 2012;115(1):169]. Anesth 25. Wang W, Li HL, Wang DX, et al. Haloperidol prophylaxis decreases
Analg. 2010;111(2):451-463. delirium incidence in elderly patients after noncardiac surgery: a ran-
19. Arenson BG, MacDonald LA, Grocott HP, Heibert BM, Arora RC. Effect domized controlled trial. Crit Care Med. 2012;40(3):731-739.
of intensive care unit environment on in-hospital delirium after cardiac 26. Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the
surgery. J Thorac Cardiovasc Surg. 2013;146(1):172-178. duration of delirium and coma in critically ill patients (Hope-ICU): a
20. Kamdar BB, Yang J, King LM, et al. Developing, implementing, and randomised, double-blind, placebo-controlled trial. Lancet Respir Med.
evaluating a multifaceted quality improvement intervention to promote 2013;1(7):515-523.
sleep in an ICU. Am J Med Qual. 2014;29(6):546-554. 27. van den Boogaard M, Pickkers P, Slooter AJ, et al. Development and val-
21. Colombo R, Corona A, Praga F, et al. A reorientation strategy for reducing idation of PRE-DELIRIC (PREdiction of DELIRium in ICu patients)
delirium in the critically ill: results of an interventional study. Minerva delirium prediction model for intensive care patients: observational
Anestesiol. 2012;78(9):1026-1033. multicentre study. BMJ. 2012;344:e420.
22. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and 28. Devlin JW, Marquis F, Riker RR, et al. Combined didactic and scenario-
occupational therapy in mechanically ventilated, critically ill patients: a based education improves the ability of intensive care unit staff to recog-
randomised controlled trial. Lancet. 2009;373(9678):1874-1882. nize delirium at the bedside. Crit Care. 2008;12(1):R19.
23. Needham DM, Korupolu R, Zanni JM, et al. Early physical medicine 29. Gesin G, Russell BB, Lin AP, Norton HJ, Evans SL, Devlin JW. Impact of
and rehabilitation for patients with acute respiratory failure: a quality a delirium screening tool and multifaceted education on nurses’ knowl-
improvement project. Arch Phys Med Rehabil. 2010;91(4):536-542. edge of delirium and ability to evaluate it correctly. Am J Crit Care. 2012;
24. Van Rompaey B, Elseviers MM, Van Drom W, Fromont V, Jorens PG. 21(1):e1-e11.
www.ccnonline.org CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 49
CCN Fast Facts CriticalCareNurse
The journal for high acuity, progressive, and critical care nursing
Nonpharmacological Interventions to
Prevent Delirium: An Evidence-Based
Systematic Review
Facts patient can complete. Additionally, nurses can advo-
Development of delirium in critical care patients is cate for removal of tubes, catheters, or restraints that
associated with increased length of stay, hospital costs, may prevent early mobilization.
and mortality. The pain, agitation, and delirium guide- • Education of nurses is an essential component of the
lines of the American College of Critical Care Medicine success of any new intervention. In order to include
provide the strongest level of recommendation for the the potentially large number of nurses who need to
use of nonpharmacological approaches to prevent be educated, education should be directed at all
delirium, but questions remain about which nonphar- types of learners.
macological interventions are beneficial. • Cognitive stimulation and reorientation is a broad
• Prevention is the optimal strategy, especially term that allows each nurse to develop an individual
when effective treatment options are unavailable. strategy. Still, each nurse’s intervention should
Haloperidol has been studied for prevention and incorporate a few key components, such as deter-
treatment of intensive care unit (ICU) delirium, mining how the patient would like to be addressed,
but the results have been inconclusive. frequent reorientation to date and time, providing
• A variety of interventions that benefit patients updates on the patient’s schedule and clinical status,
who are not critically ill would still be useful in and conversing with the patient in a manner that
an ICU. The evidence shows that targeting inter- requires memory recall by the patient.
ventions to prevent or treat known risk factors • Obtaining nurses’ acceptance of and willingness to
for delirium have the greatest benefit (eg, cogni- support the new intervention is imperative.
tive stimulation, reorientation), and a great deal • One reason for resistance is a lack of time during the
of overlap exists between risk factors for both nursing shift to add additional tasks. Assembling a
critically and non–critically ill patients. multidisciplinary team (physician, nurse, pharma-
• Multicomponent intervention protocols to cist, respiratory therapist) to determine which non-
combat delirium have proved beneficial. These pharmacological interventions are feasible within
protocols should include early mobilization, each specific unit is important.
education of nurses, and cognitive stimulation • Ultimately the success of a nonpharmacological protocol
with reorientation. to prevent delirium lies with the bedside nurses, who
• Mobilization can be as complete as full physical have the most frequent contact with patients. CCN
or occupational therapy treatments or merely
passive range-of-motion exercises. Bedside nurses
and other members of the medical team work
together to decide the level of mobilization a
Rivosecchi RM, Smithburger PL, Svec S, Campbell S, Kane-Gill SL. Nonpharmacological Interventions to Prevent Delirium: An Evidence-Based Systematic Review.
Critical Care Nurse. 2015;35(1):39-51.
50 CriticalCareNurse Vol 35, No. 1, FEBRUARY 2015 www.ccnonline.org
You might also like
- Surviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionFrom EverandSurviving Cancer, COVID-19, and Disease: The Repurposed Drug RevolutionNo ratings yet
- Oppe Fppe ToolkitDocument71 pagesOppe Fppe ToolkitFaisal Hamdi100% (1)
- Concise Definitive Review: Stress Ulcer ProphylaxisDocument11 pagesConcise Definitive Review: Stress Ulcer ProphylaxisMuhammad Umar RazaNo ratings yet
- Reducing Inappropriate Polypharmacy The Process of DeprescribingDocument8 pagesReducing Inappropriate Polypharmacy The Process of DeprescribingThiago SartiNo ratings yet
- 21 Iajps21102017 PDFDocument9 pages21 Iajps21102017 PDFBaru Chandrasekhar RaoNo ratings yet
- Artigo 2Document13 pagesArtigo 2Paulo TononNo ratings yet
- Li Et Al-2020-Cochrane Database of Systematic ReviewsDocument4 pagesLi Et Al-2020-Cochrane Database of Systematic Reviewswilliam lozaNo ratings yet
- Reconciliacao MedicamentosaDocument22 pagesReconciliacao MedicamentosapchrispimNo ratings yet
- Improving Primary Care in Rural Alabama With A Pharmacy InitiativeDocument7 pagesImproving Primary Care in Rural Alabama With A Pharmacy InitiativeBasilharbi HammadNo ratings yet
- 2013 Surgical Prophylaxis ASHP, IDSA, SHEA, SISDocument8 pages2013 Surgical Prophylaxis ASHP, IDSA, SHEA, SISMara Medina - BorleoNo ratings yet
- Factors Associated With Complementary Therapy Use in People Living With HIV/AIDS Receiving Antiretroviral TherapyDocument16 pagesFactors Associated With Complementary Therapy Use in People Living With HIV/AIDS Receiving Antiretroviral TherapyUmiyanti AzizahNo ratings yet
- Evidence Based Research PaperDocument22 pagesEvidence Based Research PaperMegan McCarthy80% (5)
- Predicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelDocument10 pagesPredicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelRiska Resty WasitaNo ratings yet
- 529-Einstein 5 3 1 246-251Document7 pages529-Einstein 5 3 1 246-251Gatwech DechNo ratings yet
- Anti Fungi CosDocument9 pagesAnti Fungi CospilarNo ratings yet
- Antifungicos PDFDocument9 pagesAntifungicos PDFpilarNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundPsiquiatría CESAMENo ratings yet
- Improving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientsDocument13 pagesImproving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientstotoksaptantoNo ratings yet
- British Journal of Clinical PharmacologyDocument6 pagesBritish Journal of Clinical PharmacologyJunerey Hume Torres RodriguezNo ratings yet
- 2014 1 Moesm1 EsmDocument51 pages2014 1 Moesm1 EsmJesus RmNo ratings yet
- Ats-Idsa 2016 Hap VapDocument51 pagesAts-Idsa 2016 Hap VapAlhafiz KarimNo ratings yet
- Medical Treatment of EpilepsyDocument17 pagesMedical Treatment of EpilepsyArbey Aponte PuertoNo ratings yet
- Hap Vap Guidelines 2016 PDFDocument51 pagesHap Vap Guidelines 2016 PDFJerryEddyaPutraBoerNo ratings yet
- Prescribing Patterns of Drugs in Outpatient Department of Paediatrics in Tertiary Care HospitalDocument12 pagesPrescribing Patterns of Drugs in Outpatient Department of Paediatrics in Tertiary Care HospitalAleena Maria KurisinkalNo ratings yet
- Describing in Cancer Patient - A Concise ReviewDocument12 pagesDescribing in Cancer Patient - A Concise ReviewEric LiangNo ratings yet
- Antipsychotics For Preventing Delirium in Hospitalized AdultsDocument12 pagesAntipsychotics For Preventing Delirium in Hospitalized AdultsLuis CsrNo ratings yet
- JMCP 2023 29 1 58Document11 pagesJMCP 2023 29 1 58Javier Martin Bartolo GarciaNo ratings yet
- UlcerDocument5 pagesUlcerabriyahNo ratings yet
- Preoperative Management of Medications For Rheumatologic and HIV DiseasesDocument21 pagesPreoperative Management of Medications For Rheumatologic and HIV DiseasesjuanpbagurNo ratings yet
- Medications and Pregnancy The Role of Community PHDocument15 pagesMedications and Pregnancy The Role of Community PHJaikapil KachhawaNo ratings yet
- Vacunacion en Esclerosis MultipleDocument12 pagesVacunacion en Esclerosis MultipleMichael Bailey LavagninoNo ratings yet
- Homeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisDocument10 pagesHomeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisCarlos Arturo Vera VásquezNo ratings yet
- Endocarditis: un estudio de cohorte multicéntrico, retrospectivoDocument8 pagesEndocarditis: un estudio de cohorte multicéntrico, retrospectivoMelendi NavarroNo ratings yet
- Artigo Lancet Medicamentos AnsiedadeDocument10 pagesArtigo Lancet Medicamentos AnsiedadeRebecca DiasNo ratings yet
- Assessment of Knowledge, Attitude, and Practice of Self-Medication Among Harar Health Sciences College Students, Harar, Eastern EthiopiaDocument6 pagesAssessment of Knowledge, Attitude, and Practice of Self-Medication Among Harar Health Sciences College Students, Harar, Eastern EthiopiaAzra SyafiraNo ratings yet
- The Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaDocument11 pagesThe Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaSabrina JonesNo ratings yet
- Antipsychotic Use in Pregnancy and The Risk For Congenital MalformationsDocument9 pagesAntipsychotic Use in Pregnancy and The Risk For Congenital MalformationsRirin WinataNo ratings yet
- A Prospective Study On Antibiotics-Associated Spontaneous Adverse Drug Reaction Monitoring and Reporting in A Tertiary Care HospitalDocument8 pagesA Prospective Study On Antibiotics-Associated Spontaneous Adverse Drug Reaction Monitoring and Reporting in A Tertiary Care HospitalNurul Hikmah12No ratings yet
- PICU DDIsDocument8 pagesPICU DDIsFAHAD KHANNo ratings yet
- Routine Amoxicillin For Uncomplicated Severe Acute Malnutrition in ChildrenDocument10 pagesRoutine Amoxicillin For Uncomplicated Severe Acute Malnutrition in ChildrenMc'onethree BrownNo ratings yet
- Introduction To Complementary Alternative and Trad PDFDocument10 pagesIntroduction To Complementary Alternative and Trad PDFAazie ZonaNo ratings yet
- Anesthesia Books 2019 Bonica's-2001-3000Document845 pagesAnesthesia Books 2019 Bonica's-2001-3000rosangelaNo ratings yet
- 1268 PDFDocument5 pages1268 PDFCMargs ConceptsNo ratings yet
- Review: Lancet Infect Dis 2014Document12 pagesReview: Lancet Infect Dis 2014Nguyễn Đức LongNo ratings yet
- Deprescribing Tools: A Review of The Types of Tools Available To Aid Deprescribing in Clinical PracticeDocument10 pagesDeprescribing Tools: A Review of The Types of Tools Available To Aid Deprescribing in Clinical PracticeandresadarvegNo ratings yet
- Use of Sedation in Palliative CareDocument13 pagesUse of Sedation in Palliative Careuriel_rojas_41No ratings yet
- e012244.fullDocument8 pagese012244.fullmuhammad.stu.appsyNo ratings yet
- Anesthesia Books 2019 Bonica's-2001-3000Document1,000 pagesAnesthesia Books 2019 Bonica's-2001-3000rosangelaNo ratings yet
- 1642-Article Text-7699-1-10-20200623Document5 pages1642-Article Text-7699-1-10-20200623mtgnzgaNo ratings yet
- The Development & Evaluation of Onc Pal GuidelineDocument8 pagesThe Development & Evaluation of Onc Pal GuidelineEric LiangNo ratings yet
- Ractice Nsights: The Critical Care Pharmacist: An Essential Intensive Care PractitionerDocument5 pagesRactice Nsights: The Critical Care Pharmacist: An Essential Intensive Care PractitionerDaniela HernandezNo ratings yet
- HPV Vaccine Programmes - Current Scenario and Recommendations in IndiaDocument3 pagesHPV Vaccine Programmes - Current Scenario and Recommendations in Indiash19782001No ratings yet
- SDOM Promising TherapiesDocument16 pagesSDOM Promising TherapiesdarlingcarvajalduqueNo ratings yet
- Jorgensen 2017Document6 pagesJorgensen 2017jessicapxeNo ratings yet
- Amer Peds Recomm Re Psy Drugs and PregnancyDocument10 pagesAmer Peds Recomm Re Psy Drugs and Pregnancyscribd4kmhNo ratings yet
- Ceph 2161 1459 4 153Document9 pagesCeph 2161 1459 4 153Zihan ZetiraNo ratings yet
- Use of Complementary and Alternative Medicines During The Third TrimesterDocument8 pagesUse of Complementary and Alternative Medicines During The Third Trimesteraisyalfi pratimiNo ratings yet
- Research in Social and Administrative Pharmacy: Amy Byrne, Sharon Byrne, Kieran DaltonDocument9 pagesResearch in Social and Administrative Pharmacy: Amy Byrne, Sharon Byrne, Kieran DaltonDede KurniawanNo ratings yet
- Drug Related Problems in Clinical Practice: A Cross Sectional Study On Their Prevalence, Risk Factors and Associated Pharmaceutical InterventionsDocument11 pagesDrug Related Problems in Clinical Practice: A Cross Sectional Study On Their Prevalence, Risk Factors and Associated Pharmaceutical InterventionsNandika Puteri TrisaniNo ratings yet
- Essential Pharmacology For Inpatient CareFrom EverandEssential Pharmacology For Inpatient CareRating: 4.5 out of 5 stars4.5/5 (7)
- User's Guide to Natural Therapies for Cancer Prevention and ControlFrom EverandUser's Guide to Natural Therapies for Cancer Prevention and ControlRating: 5 out of 5 stars5/5 (1)
- ORDINANCE TEMPLATE - First 1000 DaysDocument15 pagesORDINANCE TEMPLATE - First 1000 DaysGiezlRamos-PolcaNo ratings yet
- Manual For Medicines Good DispensingDocument114 pagesManual For Medicines Good DispensingJosh SorianoNo ratings yet
- Clinical Trial Design: Sugato Banerjee PHDDocument18 pagesClinical Trial Design: Sugato Banerjee PHDGopal KhodveNo ratings yet
- No.1202/PGD/Exams/2020 Date: 12.02.2020Document2 pagesNo.1202/PGD/Exams/2020 Date: 12.02.2020GOVARDHANNo ratings yet
- Status of Vacancy BedsDocument3 pagesStatus of Vacancy BedsAni PaulNo ratings yet
- Factory Efficiency Comes To The Hospital - The New York TimesDocument7 pagesFactory Efficiency Comes To The Hospital - The New York Timesprasanna020391No ratings yet
- Member Guide: Enhanced Sahtak PlanDocument35 pagesMember Guide: Enhanced Sahtak PlanmaniiscribdNo ratings yet
- DR Seuss - The Tooth Book - ENDocument15 pagesDR Seuss - The Tooth Book - ENLovely OwensNo ratings yet
- IAP MonitoringDocument10 pagesIAP MonitoringPangpang CpNo ratings yet
- Tuscola County Health DepartmentDocument2 pagesTuscola County Health DepartmentCourtney BennettNo ratings yet
- Anaesthesia For Cervical CerclageDocument7 pagesAnaesthesia For Cervical CerclageRamya SelvamNo ratings yet
- Diet Module 5 - 2019Document94 pagesDiet Module 5 - 2019Nithya NagrajNo ratings yet
- Association Between Low Back Pain and Various Everyday PerformancesDocument9 pagesAssociation Between Low Back Pain and Various Everyday Performancesshaik chandiniNo ratings yet
- Society For Obstetric Anesthesia and Perinatology .95413Document16 pagesSociety For Obstetric Anesthesia and Perinatology .95413dhana iphoneNo ratings yet
- PST Chapter I Overview of Education in Healthcare and ChangeDocument11 pagesPST Chapter I Overview of Education in Healthcare and ChangeXerxes PhemenineNo ratings yet
- Guide For Foreign Doctors Working in FinlandDocument10 pagesGuide For Foreign Doctors Working in FinlandNick BourNo ratings yet
- P.G. Curriculum M.S. General Surgery Index: 1. GoalsDocument14 pagesP.G. Curriculum M.S. General Surgery Index: 1. GoalsBharathi S BhatNo ratings yet
- Natural CuresDocument390 pagesNatural Cureskousalya_bala100% (3)
- Test Bank For Essentials For Nursing Practice 8th Edition Patricia A Potter Anne Griffin Perry Patricia Stockert Amy HallDocument14 pagesTest Bank For Essentials For Nursing Practice 8th Edition Patricia A Potter Anne Griffin Perry Patricia Stockert Amy Hallmichellesmallmatfqcendg100% (32)
- WBMBSDocument6 pagesWBMBSEugene Oteng-NtimNo ratings yet
- ao2016-0033-PHIC Pooling DistDocument5 pagesao2016-0033-PHIC Pooling DistAccount AlugrivNo ratings yet
- ScheduleDocument7 pagesScheduleapi-296878004No ratings yet
- First Aid Training in The Work Place (Preview and Practice) ProposalDocument4 pagesFirst Aid Training in The Work Place (Preview and Practice) ProposalIan AriNo ratings yet
- 4th Best of AUA 2019 Annual Meeting-Program - FinalDocument4 pages4th Best of AUA 2019 Annual Meeting-Program - FinalAbdelfattahHabibNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanAlea PutiNo ratings yet
- Informe - Relative, Primary and Secondary Clauses - PNF Fisioterapia.Document5 pagesInforme - Relative, Primary and Secondary Clauses - PNF Fisioterapia.ArantzaNo ratings yet
- Study Prepared For The Liberal Party of Canada Finds Covid-19 Vaccines Don't Reduce Hospitalization and Death in Those Under 60Document26 pagesStudy Prepared For The Liberal Party of Canada Finds Covid-19 Vaccines Don't Reduce Hospitalization and Death in Those Under 60Jim HoftNo ratings yet
- Case ShouldiceDocument3 pagesCase ShouldiceThắng ViếtNo ratings yet
- Total Gallium JB15939XXDocument18 pagesTotal Gallium JB15939XXAsim AliNo ratings yet