Download as pdf or txt
You might also like
- Drugs Used For Blood Coagulation Disorders - KatzungDocument3 pagesDrugs Used For Blood Coagulation Disorders - Katzungsarguss14100% (6)
- L9 - Anti-Platelet DrugsDocument8 pagesL9 - Anti-Platelet DrugsGoodone OneNo ratings yet
- 9 Anti PlateletDocument15 pages9 Anti PlateletHely PatelNo ratings yet
- Anti-Platelet DrugsDocument10 pagesAnti-Platelet DrugsGoodone OneNo ratings yet
- Anticoagulants/Antiplatelets/Thrombolytics: Uses ActionDocument4 pagesAnticoagulants/Antiplatelets/Thrombolytics: Uses Actionammar amerNo ratings yet
- L P 4 Blood Pharmacology - Final-2022Document26 pagesL P 4 Blood Pharmacology - Final-2022Zakria Al-HadadNo ratings yet
- Principles of Antiplatelet, Anticoagulant and Fibrinolytic TherapiesDocument50 pagesPrinciples of Antiplatelet, Anticoagulant and Fibrinolytic TherapiesAbby LiewNo ratings yet
- Obat Sistem HematologiDocument21 pagesObat Sistem HematologiSuryana AdityaNo ratings yet
- Hematologi Pharmacolog: Hemostasis and Blood Coagulation CascadeDocument19 pagesHematologi Pharmacolog: Hemostasis and Blood Coagulation CascadeDivina ArenaNo ratings yet
- 9 - Anti-Platelet DrugsDocument12 pages9 - Anti-Platelet DrugsGoodone OneNo ratings yet
- 20210524-Kbk-His39-Farmakologi Anti-Trombotik (Antiplatelet)Document31 pages20210524-Kbk-His39-Farmakologi Anti-Trombotik (Antiplatelet)Paul Behring ManurungNo ratings yet
- AnticoagulantDocument34 pagesAnticoagulantTasya FakhiraNo ratings yet
- BDS/MBBS Thrombolytics and Antiplatelet DrugsDocument33 pagesBDS/MBBS Thrombolytics and Antiplatelet DrugsDr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Thrombolytics, Anticoags, Antiplatelets PDFDocument21 pagesThrombolytics, Anticoags, Antiplatelets PDFrachelkdoNo ratings yet
- Drugs Used in Coagulation DisordersDocument11 pagesDrugs Used in Coagulation Disordersshoaib106muhammadNo ratings yet
- Antiplatelet Aggregation DrugsDocument14 pagesAntiplatelet Aggregation Drugs백지원 (소네트리)No ratings yet
- Blood Thinners: Hussein Hallak, PH.DDocument68 pagesBlood Thinners: Hussein Hallak, PH.DIbrahim BarhamNo ratings yet
- PFT Lecture 1Document35 pagesPFT Lecture 1Saifeldein ElimamNo ratings yet
- Blood Thinners: Maher Khdour Clinical Pharmacy, BSC, MSC, PHDDocument68 pagesBlood Thinners: Maher Khdour Clinical Pharmacy, BSC, MSC, PHDYousef JafarNo ratings yet
- Drugs Affecting Blood Cloting 2019Document39 pagesDrugs Affecting Blood Cloting 2019Mutiara RizkiNo ratings yet
- Principles of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocument36 pagesPrinciples of Antiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby Liew100% (1)
- Hematology Unit: Dr. Furqan HashmiDocument32 pagesHematology Unit: Dr. Furqan HashmiabubakarNo ratings yet
- Lecture 6 Pharma DR N AlhasaniDocument9 pagesLecture 6 Pharma DR N Alhasanialialahmedy24No ratings yet
- Direct Thrombin Inhibitors: Pharmacology and Clinical RelevanceDocument11 pagesDirect Thrombin Inhibitors: Pharmacology and Clinical RelevanceKingsley AmamchukwuNo ratings yet
- Anticoagulants:: DefinitionDocument6 pagesAnticoagulants:: DefinitionMunaza FarooqNo ratings yet
- Treatment of Hemostasis DisordersDocument17 pagesTreatment of Hemostasis DisordersDiana HyltonNo ratings yet
- AnticoagulantsTypes, Mode of Action and Preparation of Anticoagulant Bottles.Document40 pagesAnticoagulantsTypes, Mode of Action and Preparation of Anticoagulant Bottles.Arslan Arshad100% (1)
- Pharmacology and Toxicology - Anticoagulants - Medical LibraryDocument8 pagesPharmacology and Toxicology - Anticoagulants - Medical Libraryjean PiedraNo ratings yet
- The Pharma Innovation - Journal: Dabigatran Etexilate: A Drug UpdateDocument8 pagesThe Pharma Innovation - Journal: Dabigatran Etexilate: A Drug UpdateaghniajolandaNo ratings yet
- Anti Clotting, Fibrinolytic, Tests For CoagulationDocument70 pagesAnti Clotting, Fibrinolytic, Tests For CoagulationDr.Gomathi sivakumarNo ratings yet
- Antiplateletdrugs 150203231404 Conversion Gate01 PDFDocument67 pagesAntiplateletdrugs 150203231404 Conversion Gate01 PDFAndrie WigunaNo ratings yet
- Thrombolytics & Anti Platelet DrugsDocument38 pagesThrombolytics & Anti Platelet DrugsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Pharma DR - Hussein Drugs Effecting Hemostasis Lec 1Document31 pagesPharma DR - Hussein Drugs Effecting Hemostasis Lec 1rkh647m7szNo ratings yet
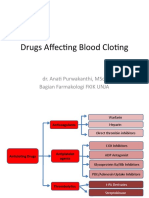
- Obat Yang Mempengaruhi Pembekuan Darah: Dr.i Made Jawi, M.Kes Bagian Farmakologi FK UnudDocument42 pagesObat Yang Mempengaruhi Pembekuan Darah: Dr.i Made Jawi, M.Kes Bagian Farmakologi FK UnudChie ZhumieNo ratings yet
- Anticlotting DrugsDocument70 pagesAnticlotting DrugsZaina Masri100% (1)
- Fibrinolytic and Antiplatelet Drugs 2020 BDS BSCN Online (Compatibility Mode)Document7 pagesFibrinolytic and Antiplatelet Drugs 2020 BDS BSCN Online (Compatibility Mode)ireneNo ratings yet
- Thrombolytic Therapy - Background, Thrombolytic Agents, Thrombolytic Therapy For Acute Myocardial InfarctionDocument27 pagesThrombolytic Therapy - Background, Thrombolytic Agents, Thrombolytic Therapy For Acute Myocardial Infarctiondmcardio21No ratings yet
- Drugs For Coagulation Disorders 2023Document26 pagesDrugs For Coagulation Disorders 2023aguilarjanicaNo ratings yet
- Drugs Used in Disorders of CoagulationDocument60 pagesDrugs Used in Disorders of CoagulationTwinkle MazaredoNo ratings yet
- Anticoagulants: Dr. Hassan Mohamed EnowDocument37 pagesAnticoagulants: Dr. Hassan Mohamed EnowFatimaNo ratings yet
- Anticoagulants: BY: Saleema Allana MSCN, AkusonamDocument35 pagesAnticoagulants: BY: Saleema Allana MSCN, AkusonamDanial HassanNo ratings yet
- AntitrombolitikDocument7 pagesAntitrombolitikadityaNo ratings yet
- Coagulation DisorderDocument38 pagesCoagulation DisorderTsegaye HailuNo ratings yet
- 14 BloodDocument32 pages14 Bloodنور الإسلامNo ratings yet
- Anti Haemostatic MechanismDocument29 pagesAnti Haemostatic MechanismDorin PathakNo ratings yet
- Static58e8b95bf5e231a18a2c2907t93746anticoagulants PDFDocument10 pagesStatic58e8b95bf5e231a18a2c2907t93746anticoagulants PDFNav ThiranNo ratings yet
- Topic HemostasisDocument10 pagesTopic HemostasisFatemeh EshaghizadehNo ratings yet
- 7 Drugs For Coagulation BleedingDocument44 pages7 Drugs For Coagulation Bleedingdiannebdc02No ratings yet
- Cardiovascular Drugs Made EZ: Part 2Document14 pagesCardiovascular Drugs Made EZ: Part 2Kandice ChandlerNo ratings yet
- Fibrinolytics, Anti Fibrinolytics and Anti Platelets: Dr. B.K.Bezbaruah Professor Pharmacology Gauhati Medical CollegeDocument46 pagesFibrinolytics, Anti Fibrinolytics and Anti Platelets: Dr. B.K.Bezbaruah Professor Pharmacology Gauhati Medical CollegeBidyut BanerjeeNo ratings yet
- Principles of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyDocument36 pagesPrinciples of An-Tiplatelet Therapy: DR Htet Htet Htethtet@Imu - Edu.MyAbby LiewNo ratings yet
- Blok 5 Hemostatic DrugDocument39 pagesBlok 5 Hemostatic DrugPutri HusnanNo ratings yet
- DR - Hussam Lec 3 Drugs Affecting Blood 2023 4Document13 pagesDR - Hussam Lec 3 Drugs Affecting Blood 2023 4ManWol JangNo ratings yet
- Hemostasis and Blood CoagulationDocument11 pagesHemostasis and Blood CoagulationRinta MoonNo ratings yet
- Blue Print Pharma - 240506 - 144035 - 623-658Document36 pagesBlue Print Pharma - 240506 - 144035 - 623-658ushiraNo ratings yet
- 9 - Anticoagulant Drugs (Final)Document17 pages9 - Anticoagulant Drugs (Final)wllmaanka4No ratings yet
- L8 Anti Coagulant DrugsDocument10 pagesL8 Anti Coagulant DrugsamanabduwahabNo ratings yet
- Anti-Coagulants, Anti-Platelets, FibrinolyticsDocument1 pageAnti-Coagulants, Anti-Platelets, FibrinolyticsGerardLum100% (1)
- Fast Facts for Patients: Thrombotic Thrombocytopenic Purpura: Prompt action saves livesFrom EverandFast Facts for Patients: Thrombotic Thrombocytopenic Purpura: Prompt action saves livesNo ratings yet
- Gastric Outlet, Small and Large Bowel ObstructionDocument16 pagesGastric Outlet, Small and Large Bowel ObstructionGoodone OneNo ratings yet
- 9 - Anti-Platelet DrugsDocument12 pages9 - Anti-Platelet DrugsGoodone OneNo ratings yet
- Anti-Platelet DrugsDocument10 pagesAnti-Platelet DrugsGoodone OneNo ratings yet
- L9 - Anti-Platelet DrugsDocument8 pagesL9 - Anti-Platelet DrugsGoodone OneNo ratings yet
- L6 - OmentumDocument12 pagesL6 - OmentumGoodone OneNo ratings yet
- Molecular BiologyDocument57 pagesMolecular BiologyGoodone OneNo ratings yet
- Procrastination: The Poor Time Management Among University StudentsDocument8 pagesProcrastination: The Poor Time Management Among University StudentsGoodone OneNo ratings yet
- Thesis Statement For Robotic SurgeryDocument5 pagesThesis Statement For Robotic Surgerychristydavismobile100% (3)
- ATLS Powerpoint YoDocument29 pagesATLS Powerpoint YobharatNo ratings yet
- ALS AlgorithmDocument22 pagesALS AlgorithmBookwormNo ratings yet
- Cerebral HemorrhageDocument10 pagesCerebral HemorrhageJayd Lorenz Vicente ChuanNo ratings yet
- Anus Chapter Sabiston SurgeryDocument16 pagesAnus Chapter Sabiston SurgeryJanny2009No ratings yet
- TULUA Lipoabdominoplasty 2020Document18 pagesTULUA Lipoabdominoplasty 2020Antonio Cardenas100% (1)
- Practical Procedures: Emergency DC Cardioversion Indications For DC CardioversionDocument2 pagesPractical Procedures: Emergency DC Cardioversion Indications For DC CardioversionLorenzo Loris ParmeggianiNo ratings yet
- March 2022 RecallsDocument292 pagesMarch 2022 RecallsNguyễn Nhật HoàngNo ratings yet
- Contemporary Outcomes of Percutaneous Closure of Patent Ductus Arteriosus in Adolescents and Adults PDFDocument8 pagesContemporary Outcomes of Percutaneous Closure of Patent Ductus Arteriosus in Adolescents and Adults PDFMuhammad IrfanNo ratings yet
- BlepharoplastyDocument23 pagesBlepharoplastyNur baitiNo ratings yet
- Cis DocumentDocument21 pagesCis Documentyoga.crossfit.kickboxingNo ratings yet
- Congenital Hypertrpphic Pyloric StenosisDocument30 pagesCongenital Hypertrpphic Pyloric StenosisParul VarshneyNo ratings yet
- The Heart 2017Document5 pagesThe Heart 2017Chowdhury Mohammed Tawhid TasneefNo ratings yet
- Inspiration 7i Ventilator BrochureDocument6 pagesInspiration 7i Ventilator BrochureAgung WicaksanaNo ratings yet
- Belser 1998Document19 pagesBelser 1998Maria Jose GodoyNo ratings yet
- ATLSDocument34 pagesATLSalice DillerudNo ratings yet
- Koding Revisi IIIDocument40 pagesKoding Revisi IIIrizky triyadiNo ratings yet
- Central Venous Pressure MonitoringDocument2 pagesCentral Venous Pressure MonitoringpauchanmnlNo ratings yet
- 2-Meninges and SinusesDocument62 pages2-Meninges and SinusesMajd HallakNo ratings yet
- Amirali Karim Is No More With UsDocument5 pagesAmirali Karim Is No More With UsMuhidin Issa MichuziNo ratings yet
- Peripheral Nerve Blocks and Peri Operative Pain Relief 2nd EdDocument269 pagesPeripheral Nerve Blocks and Peri Operative Pain Relief 2nd EdAna Alonso100% (1)
- Emergency Care in Aesthetic Medicine Practice: Mohd Shakir Bathusha Plastic SurgeonDocument96 pagesEmergency Care in Aesthetic Medicine Practice: Mohd Shakir Bathusha Plastic SurgeonRangetha ShiniNo ratings yet
- Surgical Ablative Procedures Venous Insufficiency Varicose VeinsDocument30 pagesSurgical Ablative Procedures Venous Insufficiency Varicose VeinsMohammed IbrahimNo ratings yet
- A Comparative Study of Low Dose Hyperbaric Bupivacine With Fentanyl and Hyperbaric Bupivacaine in Spinal Anaesthesia For Below Umbilical SurgeriesDocument1 pageA Comparative Study of Low Dose Hyperbaric Bupivacine With Fentanyl and Hyperbaric Bupivacaine in Spinal Anaesthesia For Below Umbilical SurgeriesTahirNo ratings yet
- Circulatory System (The Heart) 2Document20 pagesCirculatory System (The Heart) 2anuNo ratings yet
- Vascular Supply To The BrainDocument38 pagesVascular Supply To The BrainGhea Putri Hendriani100% (1)
- PolitraumaDocument9 pagesPolitraumaemo230485No ratings yet
- Anaesthesia - 2024 - Mitchell - Principles For Management of Hip Fracture For Older Adults Taking Direct OralDocument11 pagesAnaesthesia - 2024 - Mitchell - Principles For Management of Hip Fracture For Older Adults Taking Direct Oralhelen.ashton5No ratings yet
- A Modification of The Swenson Operation For Congenital MegacolonDocument8 pagesA Modification of The Swenson Operation For Congenital MegacolonGunduz AgaNo ratings yet
- UF-870AG Catalog 10P PDFDocument6 pagesUF-870AG Catalog 10P PDFAbu Bakr M. SaeedNo ratings yet