Download as pdf or txt
You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- 300D 310D and 315D Backhoe Loader IntroductionDocument7 pages300D 310D and 315D Backhoe Loader Introductionhenry ibañez100% (1)
- Y8 Textiles WorkbookDocument68 pagesY8 Textiles WorkbookCharlene Joy100% (1)
- Clinical Feature and Etiology of Septic Arthritis and Osteomyelitis in ChildrenDocument5 pagesClinical Feature and Etiology of Septic Arthritis and Osteomyelitis in ChildrenIfit Bagus ApriantonoNo ratings yet
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocument7 pagesNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNo ratings yet
- Our Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicDocument5 pagesOur Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicRonny DoankNo ratings yet
- Ovadia 2007Document7 pagesOvadia 2007uditNo ratings yet
- Research Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal SepsisDocument7 pagesResearch Article: The Analysis of Etiology and Risk Factors For 192 Cases of Neonatal Sepsisflorentina lulutNo ratings yet
- The Management of Septic Arthritis in Children: Journal ReadingDocument6 pagesThe Management of Septic Arthritis in Children: Journal ReadingRaidis PangilinanNo ratings yet
- Pi Is 1201971213002142Document5 pagesPi Is 1201971213002142melisaberlianNo ratings yet
- Xia 2016Document29 pagesXia 2016Dewi PrasetiaNo ratings yet
- Dengue JournalDocument4 pagesDengue JournalRohitKumarNo ratings yet
- PCT 2006 Read For DiscussionDocument8 pagesPCT 2006 Read For DiscussionArnavjyoti DasNo ratings yet
- Is The Diagnosis and Treatment of Childhood Acute Bacterial Meningitis in Turkey EvidentDocument5 pagesIs The Diagnosis and Treatment of Childhood Acute Bacterial Meningitis in Turkey EvidentGarryNo ratings yet
- Master ErysipelasDocument20 pagesMaster Erysipelaszul090No ratings yet
- Rheumatoid Arthritis A Single Center Egyptian Experience CorretedDocument11 pagesRheumatoid Arthritis A Single Center Egyptian Experience CorretedSara EhabNo ratings yet
- AygunDocument5 pagesAygunotheasNo ratings yet
- Sun 2012Document6 pagesSun 2012ntnquynhproNo ratings yet
- 2023 Article 35384Document9 pages2023 Article 35384RoqueAlvaradoNo ratings yet
- Hsu2019 PDFDocument6 pagesHsu2019 PDFrachmadyNo ratings yet
- 10 1016@j Jaad 2019 05 096Document8 pages10 1016@j Jaad 2019 05 096JohnNo ratings yet
- Pinda FynDocument7 pagesPinda FynCaballero X CaballeroNo ratings yet
- Primary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologyDocument6 pagesPrimary Subacute Hematogenous Osteomyelitis in Children: A Clearer Bacteriological EtiologymiNo ratings yet
- TranslateDocument5 pagesTranslatenoviadewaniNo ratings yet
- 2165-Article Text-2597-1-10-20200105Document7 pages2165-Article Text-2597-1-10-20200105IKA 79No ratings yet
- Eritema Nodoso: Causas Más Prevalentes en Pacientes Que Se Hospitalizan para Estudio, y Recomendaciones para El DiagnósticoDocument7 pagesEritema Nodoso: Causas Más Prevalentes en Pacientes Que Se Hospitalizan para Estudio, y Recomendaciones para El DiagnósticoCamilo PerillaNo ratings yet
- Moro Lago2017Document6 pagesMoro Lago2017Yamel MartínezNo ratings yet
- Clinical and Radiographic Features of Cryptococcal Neoformans Meningitis-Associated Immune Reconstitution Inflammatory SyndromeDocument7 pagesClinical and Radiographic Features of Cryptococcal Neoformans Meningitis-Associated Immune Reconstitution Inflammatory SyndromeWendi IochNo ratings yet
- Ijpedi2021 1544553Document6 pagesIjpedi2021 1544553Naresh ReddyNo ratings yet
- Acute Appendicitis in Children PDFDocument6 pagesAcute Appendicitis in Children PDFMusyawarah MelalaNo ratings yet
- Neutropenic Colitis in Children 2011Document4 pagesNeutropenic Colitis in Children 2011IRINA SULEY TIRADO PEREZNo ratings yet
- Ijcp-5481 oDocument6 pagesIjcp-5481 oDebasis ChatterjeeNo ratings yet
- Procalcitonina PDFDocument10 pagesProcalcitonina PDFFrancis MaldonadoNo ratings yet
- Orbital Cellulitis in A Pediatric Population - Experience From A Tertiary CenterDocument3 pagesOrbital Cellulitis in A Pediatric Population - Experience From A Tertiary CenterMuthu V RanNo ratings yet
- The Role of Eosinopenia in The DiagnosisDocument12 pagesThe Role of Eosinopenia in The DiagnosisNurlyanti RustamNo ratings yet
- Immunologic Evaluation of Pediatric Chronic and Recurrent Acute RhinosinusitisDocument7 pagesImmunologic Evaluation of Pediatric Chronic and Recurrent Acute RhinosinusitisandiniNo ratings yet
- SMW 09797 PDFDocument9 pagesSMW 09797 PDFEJ AguilarNo ratings yet
- Journal Read ChiaDocument14 pagesJournal Read ChiaChris Tine ChiaNo ratings yet
- Use of White Blood Cell Count and Negative Appendectomy RateDocument8 pagesUse of White Blood Cell Count and Negative Appendectomy RatePremaKurniaNo ratings yet
- AppbjDocument6 pagesAppbjGilang IrwansyahNo ratings yet
- Complications of Sepsis in Infant. A Case ReportDocument4 pagesComplications of Sepsis in Infant. A Case ReportIntania RatnaNo ratings yet
- Neu-Linf - Neu-Plt Cole AgudaDocument6 pagesNeu-Linf - Neu-Plt Cole Agudajessica MárquezNo ratings yet
- Predictors of Spontaneous Bleeding in DengueDocument4 pagesPredictors of Spontaneous Bleeding in DengueSawettachai JaitaNo ratings yet
- Bhat 2016Document6 pagesBhat 2016andrian dwiNo ratings yet
- Clinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapyDocument10 pagesClinical Presentation and Laboratory Features in Pediatric Typhoid Fever Patient Susceptibility To First-Line Antibiotic TherapySuci ZahraniNo ratings yet
- Serrum Ferritin: A Prognostic Marker in Patients With Sepsis in Pediatric Age Group: A Prospective Cohort StudyDocument4 pagesSerrum Ferritin: A Prognostic Marker in Patients With Sepsis in Pediatric Age Group: A Prospective Cohort StudyclaudyNo ratings yet
- Clinical Presentation of Scrub Typhus During A Major Outbreak in Central NepalDocument5 pagesClinical Presentation of Scrub Typhus During A Major Outbreak in Central NepalArun SedhainNo ratings yet
- Clinical OncologyDocument8 pagesClinical OncologyHector VillaseñorNo ratings yet
- R Art 42778-10Document8 pagesR Art 42778-10Kevin Wladimir ChanchicochaNo ratings yet
- 05 Lugovic Mihic PDFDocument9 pages05 Lugovic Mihic PDFmarkoperic2014No ratings yet
- Ijccm 26 67 2 2Document4 pagesIjccm 26 67 2 2alfanNo ratings yet
- Kjped 60 77Document9 pagesKjped 60 77Labontu IustinaNo ratings yet
- Prospective Analysis of Acute Encephalitis Syndrome: Clinical Characteristics and Patient Outcomes in A Tertiary Care Pediatric SettingDocument7 pagesProspective Analysis of Acute Encephalitis Syndrome: Clinical Characteristics and Patient Outcomes in A Tertiary Care Pediatric SettingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 647 3316 2 PBDocument4 pages647 3316 2 PBHabibur RahmanNo ratings yet
- Ability of Procalcitonin To Predict Bacterial MeningitisDocument20 pagesAbility of Procalcitonin To Predict Bacterial MeningitisGeorge WinchesterNo ratings yet
- Yield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care HospitalDocument5 pagesYield of Blood Cultures in Children Presenting With Febrile Illness in A Tertiary Care Hospitalfaraz.mirza1No ratings yet
- Prognostic Factors of Severe Dengue Infections in Children: AbstrakDocument10 pagesPrognostic Factors of Severe Dengue Infections in Children: Abstrakmaria lisaNo ratings yet
- Img#Document5 pagesImg#AngelNo ratings yet
- Pancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoDocument6 pagesPancytopenia: A Clinico Hematological Study: Gayathri B N, Kadam Satyanarayan RaoYeni PuspitasariNo ratings yet
- Sicca Syndrome in Patients HIVDocument6 pagesSicca Syndrome in Patients HIVkagone walidNo ratings yet
- Procalcitonin and C-Reactive Protein During Systemic Inflammatory Response Syndrome, Sepsis and Organ DysfunctionDocument9 pagesProcalcitonin and C-Reactive Protein During Systemic Inflammatory Response Syndrome, Sepsis and Organ DysfunctionAsri RachmawatiNo ratings yet
- Diagnostic Microbiology and Infectious DiseaseDocument5 pagesDiagnostic Microbiology and Infectious DiseasefranciscoreynaNo ratings yet
- 3HAC052610 AM Functional Safety and SafeMove2 RW 6-En PDFDocument236 pages3HAC052610 AM Functional Safety and SafeMove2 RW 6-En PDFlesnarjp jpNo ratings yet
- September 23, Infer The Purpose of The Poem Listened ToDocument4 pagesSeptember 23, Infer The Purpose of The Poem Listened ToLouelle GonzalesNo ratings yet
- Eng Pedagogy Class CTETDocument33 pagesEng Pedagogy Class CTETntajbun13No ratings yet
- Semantically Partitioned Object Sap BW 7.3Document23 pagesSemantically Partitioned Object Sap BW 7.3smiks50% (2)
- SBAS35029500001ENED002Document20 pagesSBAS35029500001ENED002unklekoNo ratings yet
- 1.2 FMCC221 - Introduction To International Businesss - Part 1Document19 pages1.2 FMCC221 - Introduction To International Businesss - Part 1Bernie D. TeguenosNo ratings yet
- The Radiology Assistant - Fleischner 2017 GuidelineDocument11 pagesThe Radiology Assistant - Fleischner 2017 GuidelineHenry J. Hernández L.No ratings yet
- CaneToadsKakadu 2Document3 pagesCaneToadsKakadu 2Matheesha RajapakseNo ratings yet
- New AccountDocument1 pageNew Account1144abdurrahmanNo ratings yet
- Autumn Activity BookDocument33 pagesAutumn Activity Bookbuzuleacnadya100% (3)
- Dbms Lab Dbms Lab: 23 March 202Document12 pagesDbms Lab Dbms Lab: 23 March 202LOVISH bansalNo ratings yet
- N. Mixture, CombinationDocument2 pagesN. Mixture, CombinationYareniNo ratings yet
- UntitledDocument2 pagesUntitledelleNo ratings yet
- Telegram DocumeDocument21 pagesTelegram Documemilli birhanuNo ratings yet
- Safety Data Sheet Carbon Cathode SolutionDocument11 pagesSafety Data Sheet Carbon Cathode SolutionJeff BanasekNo ratings yet
- Offer For C Check On NT-495-MG Harbour Generator Engine Against Customer Job No. E20006Document1 pageOffer For C Check On NT-495-MG Harbour Generator Engine Against Customer Job No. E20006bkrNo ratings yet
- ContinueDocument3 pagesContinueJúÑi ØrNo ratings yet
- Jobdesc Project Officer Intern TRACK SDGsDocument2 pagesJobdesc Project Officer Intern TRACK SDGssocmed gistiNo ratings yet
- 15p3 Fourier IntegralDocument7 pages15p3 Fourier IntegralBhargav BhalaraNo ratings yet
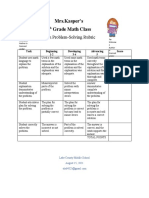
- Problemsolving RubricDocument1 pageProblemsolving Rubricapi-560491685No ratings yet
- Geography P1 May-June 2023 EngDocument20 pagesGeography P1 May-June 2023 Engtanielliagreen0No ratings yet
- 3) 2013 March - The Thing About Ms. Hollis MaynellDocument23 pages3) 2013 March - The Thing About Ms. Hollis MaynellShy TolentinoNo ratings yet
- Assessment System: Take Assessment - EWAN Chapter 8 - CCNA Exploration: Accessing The WAN (Version 4.0)Document9 pagesAssessment System: Take Assessment - EWAN Chapter 8 - CCNA Exploration: Accessing The WAN (Version 4.0)asceric4363No ratings yet
- Biophilic Design: ARC407 DissertationDocument4 pagesBiophilic Design: ARC407 DissertationAaryan JainNo ratings yet
- Indias Gold Market Reform and GrowthDocument149 pagesIndias Gold Market Reform and GrowthtmeygmvzjfnkqcwhgpNo ratings yet
- Rock Mass Characterization by High-Resolution SoniDocument17 pagesRock Mass Characterization by High-Resolution SoniJose AleNo ratings yet
- Cognizant Test 1Document20 pagesCognizant Test 1Veeraragavan SubramaniamNo ratings yet
- US Gasification DatabaseDocument9 pagesUS Gasification DatabaseAhmad DaoodNo ratings yet