Download as pdf or txt
You might also like
- CIS Evaluation FrameworkDocument40 pagesCIS Evaluation FrameworkNguyen Phuong LinhNo ratings yet
- Client Info FormDocument2 pagesClient Info FormkamalsalmanNo ratings yet
- Difficulty Breathing Difficulty BreathingDocument2 pagesDifficulty Breathing Difficulty BreathingDonna Amanda VictorinoNo ratings yet
- DateDocument1 pageDateEarn cruzNo ratings yet
- HARLEEN'S Monitoring-SlipDocument2 pagesHARLEEN'S Monitoring-SlipTarleen PandherNo ratings yet
- Atient AME GE Ender Irth ATE Ddress Hone ITY Tate IP Hysician S AME ITY HoneDocument2 pagesAtient AME GE Ender Irth ATE Ddress Hone ITY Tate IP Hysician S AME ITY Hone14-120 RahmaNo ratings yet
- Department of Education: Health Declaration FormDocument1 pageDepartment of Education: Health Declaration Formmalaki ang titik ONo ratings yet
- MAO Self Declaration FormDocument1 pageMAO Self Declaration FormShan Eean TolentinoNo ratings yet
- Daily Health Checklist of Gnhs Personnel Daily Health Checklist of Gnhs PersonnelDocument2 pagesDaily Health Checklist of Gnhs Personnel Daily Health Checklist of Gnhs Personnelargie joy marieNo ratings yet
- Nursing Care Health Assessment FormDocument5 pagesNursing Care Health Assessment FormMelanie Bagasol SisonNo ratings yet
- COVID-19 Form11233Document2 pagesCOVID-19 Form11233ahsanNo ratings yet
- HFMD Health Declaration SlipDocument2 pagesHFMD Health Declaration Slipglaiza mae olivarNo ratings yet
- Nursing Care Health Assessment Form: Instructions For CompletionDocument6 pagesNursing Care Health Assessment Form: Instructions For CompletionJM RomiasNo ratings yet
- Manga National High School Manga National High SchoolDocument1 pageManga National High School Manga National High SchoolSeth LamosteNo ratings yet
- Health Declaration Form EnglishDocument1 pageHealth Declaration Form EnglishDoyTanNo ratings yet
- COVID ASSESSMENT TOOL 3 CopiesDocument3 pagesCOVID ASSESSMENT TOOL 3 Copiesmahather silunganNo ratings yet
- Norsu Health Declaration Form 1 September 2022Document1 pageNorsu Health Declaration Form 1 September 2022Joshua Allen AjetoNo ratings yet
- AOA COVID Exposure QuestionnaireDocument1 pageAOA COVID Exposure QuestionnaireClarisse LucenaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJilli JardiolinNo ratings yet
- Diagnostic English ExamDocument1 pageDiagnostic English ExamScribdTranslationsNo ratings yet
- New Patient Paperwork (FINAL DRAFT)Document4 pagesNew Patient Paperwork (FINAL DRAFT)andrew_sokolNo ratings yet
- Symptom and Exposure QuestionnaireDocument2 pagesSymptom and Exposure QuestionnaireClickon DetroitNo ratings yet
- TESDA COVID-19 Health Status Daily Monitoring TESDA COVID - 19 Health Status Daily MonitoringDocument1 pageTESDA COVID-19 Health Status Daily Monitoring TESDA COVID - 19 Health Status Daily MonitoringMICS TVNo ratings yet
- Workplace Prevention and Control of CovidDocument1 pageWorkplace Prevention and Control of Coviddee dee sevachNo ratings yet
- Covid RegistrationDocument2 pagesCovid RegistrationAthenaNo ratings yet
- Covid Screening ToolDocument1 pageCovid Screening TooljpNo ratings yet
- Declaration Form (COVID)Document1 pageDeclaration Form (COVID)Pamela Joyce MaddumaNo ratings yet
- Health Declaration ChecklistDocument2 pagesHealth Declaration ChecklistCatherine Caluste AlipatNo ratings yet
- Health Survey QuestionnaireDocument3 pagesHealth Survey QuestionnairerevilozabellasophiaNo ratings yet
- Annex B - January 2022 Archi LE DVODocument3 pagesAnnex B - January 2022 Archi LE DVOYanessa Abdukahil MawalicNo ratings yet
- HEALTH DECLARATION SHEET 2022 (Students)Document1 pageHEALTH DECLARATION SHEET 2022 (Students)Mark Anthony Arenas GioketoNo ratings yet
- Health QuestionnaireDocument2 pagesHealth QuestionnaireReihan SadîkNo ratings yet
- Annex B - May 2022 CeleDocument3 pagesAnnex B - May 2022 CeleSinha ElleNo ratings yet
- 11th REVISION HEALTH DECLARATION FORM 11 OCT 2020Document1 page11th REVISION HEALTH DECLARATION FORM 11 OCT 2020TIMMY BOYNo ratings yet
- Health Care Questionnaire For CrewDocument1 pageHealth Care Questionnaire For Crewatin adityaNo ratings yet
- Chronicle Diabetes Assessment FormDocument8 pagesChronicle Diabetes Assessment FormpriyaNo ratings yet
- Health Condition Form Questionnaire - FINALDocument2 pagesHealth Condition Form Questionnaire - FINALLeonardNo ratings yet
- SMI COVID-19 Health Survey Form - RevisedDocument2 pagesSMI COVID-19 Health Survey Form - RevisedJess Rey Q. BaranNo ratings yet
- Children's Health Record: Child Information Health HistoryDocument2 pagesChildren's Health Record: Child Information Health Historyeric wruckNo ratings yet
- Physical Education Physical Fitness Training ProgramDocument15 pagesPhysical Education Physical Fitness Training ProgramPatriciaNo ratings yet
- Employees Health Declaration FormDocument1 pageEmployees Health Declaration FormELENITA VILLANo ratings yet
- Health Statement FormDocument1 pageHealth Statement FormALT IkedaNo ratings yet
- Health Declaration CardDocument2 pagesHealth Declaration CardJasmin AngieNo ratings yet
- QR InboundDocument10 pagesQR InboundSCRAT FUENBELNo ratings yet
- Health FormDocument1 pageHealth FormLinlen ViagedorNo ratings yet
- Developmental History QuestionnaireDocument6 pagesDevelopmental History QuestionnaireMariana RzNo ratings yet
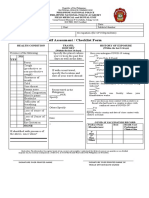
- Self Assessment / Checklist Form: YES NODocument1 pageSelf Assessment / Checklist Form: YES NOdoie kimNo ratings yet
- ISO 05 Student Health Record 1 RevDocument2 pagesISO 05 Student Health Record 1 RevHahaha HihihooNo ratings yet
- Patient Form 2010Document3 pagesPatient Form 2010elliepickNo ratings yet
- Pediatric History FormDocument2 pagesPediatric History FormJim Jose AntonyNo ratings yet
- Inbound 2251609052538566261Document1 pageInbound 2251609052538566261sam.sarip0No ratings yet
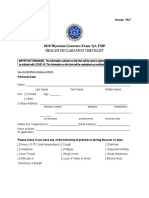
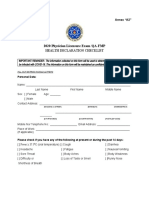
- 2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistDocument3 pages2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistLeera raNo ratings yet
- Annex A2 Health Declaration ChecklistDocument3 pagesAnnex A2 Health Declaration Checklistcandy ricel pascuaNo ratings yet
- 2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistDocument3 pages2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistMueller HintonNo ratings yet
- 2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistDocument3 pages2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistBryan P. GayoNo ratings yet
- 2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistDocument3 pages2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistLei Rivera CabulayNo ratings yet
- 2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistDocument3 pages2020 Physician Licensure Exam /Qa-Fmp: Health Declaration ChecklistNikki DiocampoNo ratings yet
- Child Health and Development QuestionnaireDocument2 pagesChild Health and Development QuestionnaireFrom Accelerated Derrick SmithNo ratings yet
- Certificate of Physical Fitness: IA. History of Any Known Illness / SurgeryDocument5 pagesCertificate of Physical Fitness: IA. History of Any Known Illness / SurgeryPrakash RNo ratings yet
- Gordon S Functional Health Pattern Assessment TooL: EdisonDocument13 pagesGordon S Functional Health Pattern Assessment TooL: EdisonEdison Olad Dangkeo, RN,RM67% (3)
- BST School Policies Health and Safety Policy January 2020Document3 pagesBST School Policies Health and Safety Policy January 2020Nguyen Phuong LinhNo ratings yet
- BusSafetyMinutes July2012Document9 pagesBusSafetyMinutes July2012Nguyen Phuong LinhNo ratings yet
- BST School Policies Privacy and Data Protection Policy December 2019Document3 pagesBST School Policies Privacy and Data Protection Policy December 2019Nguyen Phuong LinhNo ratings yet
- CipaDocument2 pagesCipaNguyen Phuong LinhNo ratings yet
- CIS Introductory WorkshopDocument31 pagesCIS Introductory WorkshopNguyen Phuong LinhNo ratings yet
- Strategic PlanDocument28 pagesStrategic PlanNguyen Phuong LinhNo ratings yet
- Parent Suggestion FormDocument1 pageParent Suggestion FormNguyen Phuong LinhNo ratings yet
- FAQs-for-potential-applicants (GVNN Ung Tuyen)Document4 pagesFAQs-for-potential-applicants (GVNN Ung Tuyen)Nguyen Phuong LinhNo ratings yet
- Safeguarding Policy 2018.183893203Document61 pagesSafeguarding Policy 2018.183893203Nguyen Phuong LinhNo ratings yet
- BUSPH Strategy Map. FinalDocument2 pagesBUSPH Strategy Map. FinalNguyen Phuong LinhNo ratings yet
- Sexting Policy April 2019Document8 pagesSexting Policy April 2019Nguyen Phuong LinhNo ratings yet
- Teacher Performance Evaluation FormDocument3 pagesTeacher Performance Evaluation FormNguyen Phuong LinhNo ratings yet
- School CommunicationDocument1 pageSchool CommunicationNguyen Phuong LinhNo ratings yet
- TQF Draft Rubric - Aug 2018 - v05 1Document2 pagesTQF Draft Rubric - Aug 2018 - v05 1Nguyen Phuong LinhNo ratings yet
- Communicationpolicyf D 2016Document12 pagesCommunicationpolicyf D 2016Nguyen Phuong LinhNo ratings yet
- Food and Healthy Eating Policy March 2018Document5 pagesFood and Healthy Eating Policy March 2018Nguyen Phuong LinhNo ratings yet
- Anchorage School District K-12 Enrollment PacketDocument24 pagesAnchorage School District K-12 Enrollment PacketNguyen Phuong LinhNo ratings yet
- Behaviour Policy 2019.187203519Document18 pagesBehaviour Policy 2019.187203519Nguyen Phuong LinhNo ratings yet
- Fwec FaqDocument2 pagesFwec FaqNguyen Phuong LinhNo ratings yet
- Handbook PICDocument72 pagesHandbook PICNguyen Phuong LinhNo ratings yet
- Looking After Each Other and OurseltDocument3 pagesLooking After Each Other and OurseltNguyen Phuong LinhNo ratings yet
- Digital Art and DesignDocument97 pagesDigital Art and DesignNguyen Phuong LinhNo ratings yet
- Staff Wellbeing Poster PrintDocument1 pageStaff Wellbeing Poster PrintNguyen Phuong LinhNo ratings yet
- Desirable - Features - Presentation (Level Standard)Document4 pagesDesirable - Features - Presentation (Level Standard)Nguyen Phuong LinhNo ratings yet
- Managing The Transition Back To SchoolDocument4 pagesManaging The Transition Back To SchoolNguyen Phuong LinhNo ratings yet
- blf17 - 20 Second School Measuresbl 17 03 17bDocument13 pagesblf17 - 20 Second School Measuresbl 17 03 17bNguyen Phuong LinhNo ratings yet
- Engaging With All Parent and CarersDocument11 pagesEngaging With All Parent and CarersNguyen Phuong LinhNo ratings yet
- AN Activity 9Document1 pageAN Activity 9Nguyen Phuong LinhNo ratings yet