Download as pdf or txt
You might also like
- Biology Investigatory Project On Mendelian DisordersDocument42 pagesBiology Investigatory Project On Mendelian DisordersPrasaanth Rock86% (14)
- Annex I Summary of Product CharacteristicsDocument56 pagesAnnex I Summary of Product Characteristicsvicentiu2003No ratings yet
- dược động họcDocument68 pagesdược động họcKhánh DuyênnNo ratings yet
- Nuwiq Epar Product Information enDocument54 pagesNuwiq Epar Product Information enSutirtha MukhopadhyayNo ratings yet
- Abnormal Uterine BleedingDocument15 pagesAbnormal Uterine BleedingDr-Saja O. DmourNo ratings yet
- Australia Pharmaceutical Market EnvironmentDocument2 pagesAustralia Pharmaceutical Market Environmentdineshmerani123No ratings yet
- The Importance of AdherenceDocument28 pagesThe Importance of AdherenceVijay LaptopNo ratings yet
- Zoladex BC 2019 - ApprovedDocument23 pagesZoladex BC 2019 - ApprovedSiti DaraauliaNo ratings yet
- Gazer PH 2017 Budget Final @40minchDocument114 pagesGazer PH 2017 Budget Final @40minchSamuel DeysiNo ratings yet
- Httpse-Katalog LKPP Go Idjcommon Blob Filedownloaderdownloadid B159767da5c33c0fc558c8a4138Document32 pagesHttpse-Katalog LKPP Go Idjcommon Blob Filedownloaderdownloadid B159767da5c33c0fc558c8a4138Mohamed RawyNo ratings yet
- Critical Appraisal Checklist For An Article On Treatment or PreventionDocument6 pagesCritical Appraisal Checklist For An Article On Treatment or PreventionDewi Hayu KiranaNo ratings yet
- PSF Clinical Pearls For StudentsDocument28 pagesPSF Clinical Pearls For StudentsChandan VishwakarmaNo ratings yet
- Lecture 7, GTNDocument47 pagesLecture 7, GTNreem.khafagyyNo ratings yet
- A Prospective Study of Acute Fissure-In-Ano in Relation To Clinical Diagnosis and ManagementDocument5 pagesA Prospective Study of Acute Fissure-In-Ano in Relation To Clinical Diagnosis and ManagementIJAR JOURNALNo ratings yet
- Thrombolytics: Interventional FellowDocument51 pagesThrombolytics: Interventional Fellowusfcards100% (1)
- Protokol KemoDocument13 pagesProtokol KemoVeysusanNo ratings yet
- Comparatie Radioterapie Adjuvantă-Radioterapie de SalvareDocument11 pagesComparatie Radioterapie Adjuvantă-Radioterapie de SalvareconionicNo ratings yet
- Use of Half-Life InformationDocument5 pagesUse of Half-Life InformationSamehabdulla AbdullaNo ratings yet
- RabiesDocument47 pagesRabiesFrancisco Gangoso Jr.No ratings yet
- 6C Results and DicussionDocument6 pages6C Results and DicussionJessa Mae AsiadoNo ratings yet
- Hebron University - Faculty of Nursing Name: Malik Manasrah Supervisor: Dr. Hussain JabareenDocument37 pagesHebron University - Faculty of Nursing Name: Malik Manasrah Supervisor: Dr. Hussain JabareenMalik ManasrahNo ratings yet
- Clinical Development Programs For Chronic Idiopathic Urticaria Indication For H1-AntihistaminesDocument23 pagesClinical Development Programs For Chronic Idiopathic Urticaria Indication For H1-AntihistaminesfadlNo ratings yet
- Knowledge-Based Planning For SRS: From Quality Control To Full AutomationDocument35 pagesKnowledge-Based Planning For SRS: From Quality Control To Full AutomationJamel YahyaouiNo ratings yet
- NW PepDocument71 pagesNW PepRupali MukhijaNo ratings yet
- Actim PartusDocument6 pagesActim PartusAncuta TiperciucNo ratings yet
- HemaDocument3 pagesHemaJoshuaNo ratings yet
- Use of GTNDocument8 pagesUse of GTNAndrew SuryaNo ratings yet
- Pain and Pain Management in ThalDocument36 pagesPain and Pain Management in ThalKavirNivNo ratings yet
- 1.3.3 Diarrhea-4 Januari-3 JanDocument56 pages1.3.3 Diarrhea-4 Januari-3 JanmaryamNo ratings yet
- HERPES (fINAL)Document3 pagesHERPES (fINAL)Andrea Dora OrtalizNo ratings yet
- Hipertiroidismo en GatosDocument20 pagesHipertiroidismo en GatosBrenda GómezNo ratings yet
- To Assess The Effectiveness of Application of Aloe Vera Gel On Pressure Ulcers Among Patients Admitted in Selected HospitalsDocument4 pagesTo Assess The Effectiveness of Application of Aloe Vera Gel On Pressure Ulcers Among Patients Admitted in Selected HospitalsIJAR JOURNALNo ratings yet
- AANASMintro AttendeeDocument26 pagesAANASMintro AttendeeJere AyerbeNo ratings yet
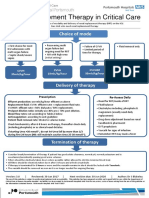
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Profilaxia TEPDocument15 pagesProfilaxia TEPLantoş Filip FernandoNo ratings yet
- Therapy WorksheetDocument3 pagesTherapy WorksheetGokull ShautriNo ratings yet
- Tretinoin Monograph 1feb2014Document6 pagesTretinoin Monograph 1feb2014Milad RostamiNo ratings yet
- HAUT HMV Brazil Grand Rounds April 29 2014Document74 pagesHAUT HMV Brazil Grand Rounds April 29 2014carlosrschusterNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptBella DirkNo ratings yet
- Tugas Farmasi Klinik - Ebm - Kelompok 4Document8 pagesTugas Farmasi Klinik - Ebm - Kelompok 4verra nurmaylindhaNo ratings yet
- Case 2 Pre-Op & Post-Op CareDocument1 pageCase 2 Pre-Op & Post-Op Carecbac1990No ratings yet
- Week 5 THE PROCESS OF REPRODUCTIONDocument22 pagesWeek 5 THE PROCESS OF REPRODUCTIONVonreev OntoyNo ratings yet
- Krishna 26pDocument29 pagesKrishna 26pyanshutradelink.pvtNo ratings yet
- Asma Management 08 - 09 - 07Document81 pagesAsma Management 08 - 09 - 07botolkecapNo ratings yet
- Hormone/Contraceptive Use in O&G: Provera Acute Maintena NceDocument2 pagesHormone/Contraceptive Use in O&G: Provera Acute Maintena Ncekhangsiean89No ratings yet
- Apixaban Eliquis MonographDocument14 pagesApixaban Eliquis MonographTran Minh NgocNo ratings yet
- Emergency Contraception: Joseph B. Stanford, MD, MSPHDocument61 pagesEmergency Contraception: Joseph B. Stanford, MD, MSPHputrakartonoNo ratings yet
- Lab Dept: Hematology Test Name: Reticulocyte Count: General InformationDocument2 pagesLab Dept: Hematology Test Name: Reticulocyte Count: General InformationTanveerNo ratings yet
- Karakteristik Faktor Siklus MenstruasiDocument7 pagesKarakteristik Faktor Siklus MenstruasiMerry NildaweniNo ratings yet
- Afika Alam M Alfian Arsyadi Besta DesmaraDocument14 pagesAfika Alam M Alfian Arsyadi Besta Desmarabenefits35No ratings yet
- Pillar ComparisonDocument1 pagePillar ComparisonSatya PNo ratings yet
- Nursing Care Hours Per Patient DayDocument5 pagesNursing Care Hours Per Patient Dayjo_annamae4413No ratings yet
- Guidance On The Rational Use of RH Kit 3 (Post Rape Management)Document8 pagesGuidance On The Rational Use of RH Kit 3 (Post Rape Management)hiba.khellowNo ratings yet
- Rev PMTCT 2017Document35 pagesRev PMTCT 2017danielNo ratings yet
- Use of The Barthel Index, Activities of Daily Living, in Dermatologic Surgery in Patients Aged 80 Years and OlderDocument6 pagesUse of The Barthel Index, Activities of Daily Living, in Dermatologic Surgery in Patients Aged 80 Years and OldertitinNo ratings yet
- 004 MChirenje Adherence To Daily TruvadaDocument28 pages004 MChirenje Adherence To Daily TruvadaRania El-DesokyNo ratings yet
- Nrg-Gi002 Protocol PresentationDocument16 pagesNrg-Gi002 Protocol Presentationapi-508897697No ratings yet
- Taketomo 2019Document328 pagesTaketomo 2019Oscar AguileraNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Thyroidectomy Diet: A Beginner's 2-Week Step-by-Step Guide After Thyroid Gland Removal, With Sample Recipes and a Meal PlanFrom EverandThyroidectomy Diet: A Beginner's 2-Week Step-by-Step Guide After Thyroid Gland Removal, With Sample Recipes and a Meal PlanNo ratings yet
- IFMBE Proceedings: Series EditorDocument27 pagesIFMBE Proceedings: Series EditorIntan HartandyNo ratings yet
- Translation, Cultural Adaptation, and Validation of Short-Form 6D On The General Population in IndonesiaDocument6 pagesTranslation, Cultural Adaptation, and Validation of Short-Form 6D On The General Population in IndonesiaIntan HartandyNo ratings yet
- Similarity - An Evaluation of Chest X-Ray in The Context of Community-Based Screening of Child Tuberculosis ContactsDocument17 pagesSimilarity - An Evaluation of Chest X-Ray in The Context of Community-Based Screening of Child Tuberculosis ContactsIntan HartandyNo ratings yet
- Yati Soenarto - RACP AucklandDocument34 pagesYati Soenarto - RACP AucklandIntan HartandyNo ratings yet
- High Sensitivity Troponin I: CausesDocument1 pageHigh Sensitivity Troponin I: CausesIntan HartandyNo ratings yet
- Haemophilia 1Document10 pagesHaemophilia 1mahadirrosNo ratings yet
- Management of Bleeding PDFDocument25 pagesManagement of Bleeding PDFGlory Owens AgbonkpoloNo ratings yet
- Dental Management of Hemophiliac ChildDocument6 pagesDental Management of Hemophiliac ChildMelisa RuthNo ratings yet
- NBT 4305Document12 pagesNBT 4305RobsonNo ratings yet
- HEMOPHILIA GuidelinesDocument76 pagesHEMOPHILIA Guidelinesmarco_jacinto1103197No ratings yet
- Care of HemophiliaDocument7 pagesCare of HemophiliaBasant karn100% (4)
- Anti FVIII Antibody and Inhibitor Development Patterns in Hemophili - 2019 - BloDocument3 pagesAnti FVIII Antibody and Inhibitor Development Patterns in Hemophili - 2019 - BloMichael John AguilarNo ratings yet
- Hemophilia ADocument8 pagesHemophilia AroxhencaNo ratings yet
- MCL Loinc ValuesDocument1,291 pagesMCL Loinc ValuesERIKA ANNE CADAWANNo ratings yet
- Hema Q&aDocument126 pagesHema Q&aHoney Lyn AlebioNo ratings yet
- A Brief History of HemophiliaDocument127 pagesA Brief History of HemophiliaApurba SahaNo ratings yet
- Hematologic DisorderDocument16 pagesHematologic Disorderjulesubayubay5428No ratings yet
- Haemophilic ArthritisDocument5 pagesHaemophilic Arthritismanoj ramlal kandoiNo ratings yet
- Hemorrhagic Coagulation DisordersDocument42 pagesHemorrhagic Coagulation DisordersGirum TesfayeNo ratings yet
- CP - Hemophilia 2Document40 pagesCP - Hemophilia 2Reezka PutraNo ratings yet
- HEMOPHILIADocument74 pagesHEMOPHILIASylvia LoongNo ratings yet
- Year 3 Medicine Posting G-1, R-5b, August, 2021Document23 pagesYear 3 Medicine Posting G-1, R-5b, August, 2021BABU BRAMANAPALLE JAGADEESHNo ratings yet
- HemophiliaDocument62 pagesHemophiliamuhirwa Samuel100% (1)
- HemophiliaDocument27 pagesHemophiliaDorothy Pearl Loyola Palabrica100% (1)
- CoagulopathyDocument121 pagesCoagulopathyMegat Mohd Azman AdzmiNo ratings yet
- Paediatrics MCQ QuestionsDocument69 pagesPaediatrics MCQ QuestionsShandev IndoiNo ratings yet
- NCM 109 Finals L10 1Document18 pagesNCM 109 Finals L10 1Leigh Angelika Dela CruzNo ratings yet
- Bleeding Disorder (Paediatrics)Document95 pagesBleeding Disorder (Paediatrics)Nurul Afiqah Mohd YusoffNo ratings yet
- 2 Inherited Bleeding Disorders: Victor S. Blanchette Cathy Sparling Christopher TurnerDocument42 pages2 Inherited Bleeding Disorders: Victor S. Blanchette Cathy Sparling Christopher Turnershinichi kudoNo ratings yet
- Haemophilia - 2022 - Carcao - Low Dose Prophylaxis and Antifibrinolytics Options To Consider With Proven Benefits ForDocument9 pagesHaemophilia - 2022 - Carcao - Low Dose Prophylaxis and Antifibrinolytics Options To Consider With Proven Benefits FordavidNo ratings yet
- J 1365-2516 2012 02820 XDocument208 pagesJ 1365-2516 2012 02820 XSakinah Mar'ie SanadNo ratings yet
- CBU 5th Year Exam Paper 1 2017Document13 pagesCBU 5th Year Exam Paper 1 2017Homeground entertainment100% (3)
- Chapter 6 Prophylaxis in HemophiliaDocument49 pagesChapter 6 Prophylaxis in Hemophiliakalinayak.prasadNo ratings yet
- MonoarthritisDocument7 pagesMonoarthritisSalsa NadillaNo ratings yet