Download as pdf or txt
You might also like
- Cockney MonologuesDocument2 pagesCockney MonologuesLaReceHawkins86% (7)
- The Ultimate Guide To Drum Programming - EDMProdDocument32 pagesThe Ultimate Guide To Drum Programming - EDMProdSteveJones100% (4)
- IFA Coaching Session PlannerDocument2 pagesIFA Coaching Session Plannerabdesslam chamamiNo ratings yet
- DI Abdomen P 102 189 PART 1 SEC 2Document88 pagesDI Abdomen P 102 189 PART 1 SEC 2tudoranluciana1No ratings yet
- Dysphagia (ENT Posting)Document36 pagesDysphagia (ENT Posting)rajhiniNo ratings yet
- Dysphagia: DR (Prof.) A B Singh Unit Department of General Surgery Patna Medical College & HospitalDocument48 pagesDysphagia: DR (Prof.) A B Singh Unit Department of General Surgery Patna Medical College & HospitalAswin Rajasekaran100% (1)
- Gastrointestinal System: Symptomatology of TheDocument85 pagesGastrointestinal System: Symptomatology of TheAbdelrahman MokhtarNo ratings yet
- Dysphagia: Dr. Sameeah A. Rashid MBCHB, DMRD, Fibms College of Medicine, Hawler Medical UniversityDocument35 pagesDysphagia: Dr. Sameeah A. Rashid MBCHB, DMRD, Fibms College of Medicine, Hawler Medical UniversityDarawan MirzaNo ratings yet
- GIT - EsophagusDocument5 pagesGIT - EsophagussebarikattaNo ratings yet
- Clinical Approach To Patient With Gastrointestinal DiseaseDocument5 pagesClinical Approach To Patient With Gastrointestinal DiseasePriyanka SamalNo ratings yet
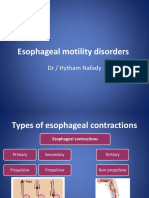
- Esophageal Motility Disorders: DR / Hytham NafadyDocument31 pagesEsophageal Motility Disorders: DR / Hytham NafadyRabie MeramNo ratings yet
- Nursing Management of Git Problems: Oral and Esophageal DisordersDocument18 pagesNursing Management of Git Problems: Oral and Esophageal Disorderslcpot_se7en7505100% (2)
- PD 3.2 Alterations in GI Function Part 1Document6 pagesPD 3.2 Alterations in GI Function Part 1Kim DeeNo ratings yet
- Pathology of EsophagusDocument59 pagesPathology of EsophagusDoc On CallNo ratings yet
- 323 Diseases of the EsophagusDocument17 pages323 Diseases of the Esophaguscccarrot.carrot3No ratings yet
- GI Sympt Mokhtar (2015)Document85 pagesGI Sympt Mokhtar (2015)Abdelrahman MokhtarNo ratings yet
- Gastrointestinal Diseases Part2Document8 pagesGastrointestinal Diseases Part2sarguss14No ratings yet
- Esophagous Stomach Small Intestine PathologyDocument58 pagesEsophagous Stomach Small Intestine PathologytahaNo ratings yet
- Barium Swallow: DR Akash Bhosale Jr1Document66 pagesBarium Swallow: DR Akash Bhosale Jr1Aakash BhosaleNo ratings yet
- HerniaDocument17 pagesHerniaIndro WibowoNo ratings yet
- Esophageal ConditionsDocument43 pagesEsophageal ConditionsMICHAEL SAKALANo ratings yet
- Intestinal Obstruction: MSU Medical Students. Batch 2. Group 2Document31 pagesIntestinal Obstruction: MSU Medical Students. Batch 2. Group 2Qp Nizam100% (2)
- Wa0001Document41 pagesWa0001Riya ShindeNo ratings yet
- 3i HIRURGIJA - ŽELUCA I CRIJEVA Nejra Kikanović, Naida Kikanović I Indir Kulanić1275776300763Document20 pages3i HIRURGIJA - ŽELUCA I CRIJEVA Nejra Kikanović, Naida Kikanović I Indir Kulanić1275776300763Basketball is my loveNo ratings yet
- Surgical Diseases of The EsophagusDocument35 pagesSurgical Diseases of The Esophagusmogesie1995No ratings yet
- Clinical Approach To A Patient With Dysphagia: Medicine UpdateDocument3 pagesClinical Approach To A Patient With Dysphagia: Medicine UpdateAnonymous XFDJfsGviNo ratings yet
- Vermicular AppendixDocument3 pagesVermicular AppendixMuhaimin AbdullahNo ratings yet
- Gs Toronto Nots PdaDocument34 pagesGs Toronto Nots PdaAhmed AttiaNo ratings yet
- Apr 28 Ultrasound Chawla PDFDocument85 pagesApr 28 Ultrasound Chawla PDFAna-Maria PopaNo ratings yet
- GIT Fully DoneDocument14 pagesGIT Fully DoneTirtha Taposh100% (1)
- Pediatric Surgery (1st Edition)Document60 pagesPediatric Surgery (1st Edition)baratniloy1No ratings yet
- Dysphagia: Dr. Ravi Gadani MS, FmasDocument39 pagesDysphagia: Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- Git ReviewDocument173 pagesGit Reviewesra1altahirNo ratings yet
- Dysphagia: Ian Paul Titus DM FRCSDocument59 pagesDysphagia: Ian Paul Titus DM FRCSGiovanni HenryNo ratings yet
- Contrasted Studies GITDocument91 pagesContrasted Studies GITolumNo ratings yet
- Dysphagia DiseaseDocument212 pagesDysphagia DiseaseAprita NurkarimaNo ratings yet
- Dysphagia: DR Navin Shukla Associate Professor Department of E.N.T&H.N.SDocument64 pagesDysphagia: DR Navin Shukla Associate Professor Department of E.N.T&H.N.SNavin ShuklaNo ratings yet
- Paraoesophageal HerniaDocument1 pageParaoesophageal HerniamuhammadridhwanNo ratings yet
- Esophageal Disorders AtfDocument30 pagesEsophageal Disorders AtfMaryamNo ratings yet
- Intestinal ObstructionDocument27 pagesIntestinal ObstructionAna AvilaNo ratings yet
- Gastrointestinal Tract PathologyDocument12 pagesGastrointestinal Tract PathologyTurinawe Bin ByensiNo ratings yet
- Oesophagus StomachDocument28 pagesOesophagus Stomachwanja91No ratings yet
- THE Gastro-Intestinal TractDocument51 pagesTHE Gastro-Intestinal TractandrewNo ratings yet
- CASE PRESENTATION Nadhirah RahimDocument60 pagesCASE PRESENTATION Nadhirah RahimNadhirah Rahim100% (1)
- Esophageal DisordersDocument37 pagesEsophageal DisordersDanielle FosterNo ratings yet
- BOWEL DISEASES YeniDocument226 pagesBOWEL DISEASES YeniIsmail BayraktaroğluNo ratings yet
- Radiology EssentialsDocument308 pagesRadiology EssentialsDeborah Anasthasia PakpahanNo ratings yet
- BariumswallowDocument48 pagesBariumswallowCintyaRolitaNo ratings yet
- Dysphagia: Departemen THT-KL Fakultas Kedokteran Universitas Padjadjaran 2016Document31 pagesDysphagia: Departemen THT-KL Fakultas Kedokteran Universitas Padjadjaran 2016Sherlyn YeeNo ratings yet
- DysphagiaDocument29 pagesDysphagiaRahul Kumar VermaNo ratings yet
- Intestinal ObstructionDocument56 pagesIntestinal ObstructionGiovanna AlguNo ratings yet
- Acute Intestinal ObstructionDocument38 pagesAcute Intestinal ObstructiondinahzrNo ratings yet
- 1.3 DysphagiaDocument37 pages1.3 Dysphagiavk4bftgg2kNo ratings yet
- Hirschsprung Disease FarieDocument38 pagesHirschsprung Disease FarieFarie Farihan67% (3)
- Lapkas Hi 4-6-18Document41 pagesLapkas Hi 4-6-18kalvinNo ratings yet
- Colonic LesionsDocument89 pagesColonic Lesionsjagadeesan_ushaNo ratings yet
- Differential Diagnosis of DysphagiaDocument20 pagesDifferential Diagnosis of Dysphagiat5sccj2bpzNo ratings yet
- Radiology GitDocument6 pagesRadiology GitShms GaneemNo ratings yet
- Intestinal ObstructionDocument35 pagesIntestinal Obstructionwht89100% (1)
- Chapter 17 - Gastrointestinal TractDocument29 pagesChapter 17 - Gastrointestinal TractAgnieszka WisniewskaNo ratings yet
- AppenDocument25 pagesAppenFernando AnibanNo ratings yet
- Gastroesophageal Reflux Disease: L. V. Borisova Docent., Ph. DDocument32 pagesGastroesophageal Reflux Disease: L. V. Borisova Docent., Ph. DSalma Mohamed RezkNo ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- TL-WN722N (UN) (US) V2 Datasheet PDFDocument4 pagesTL-WN722N (UN) (US) V2 Datasheet PDFBender :DNo ratings yet
- Buy Xanax Online To Treat With Stress and Anxiety - Order Xanax OnlineDocument5 pagesBuy Xanax Online To Treat With Stress and Anxiety - Order Xanax OnlinelorendesuzaNo ratings yet
- 2013 848evo DucatiOmahaDocument140 pages2013 848evo DucatiOmahaFabian Alejandro Ramos SandovalNo ratings yet
- Highway Engineering I: Chapter Four Geometrical Design of HighwayDocument39 pagesHighway Engineering I: Chapter Four Geometrical Design of Highwaysirajt300No ratings yet
- Trades About To Happen - David Weiss - Notes FromDocument3 pagesTrades About To Happen - David Weiss - Notes FromUma Maheshwaran100% (1)
- Getting The Call From Stockholm: My Karolinska Institutet ExperienceDocument31 pagesGetting The Call From Stockholm: My Karolinska Institutet ExperienceucsfmededNo ratings yet
- Vikram-Betal Case StudyDocument5 pagesVikram-Betal Case StudyRavi SawantNo ratings yet
- Abcp Offering CircularDocument2 pagesAbcp Offering Circulartom99922No ratings yet
- PW Group Project Proposal Final DraftDocument4 pagesPW Group Project Proposal Final DraftZher Min0% (1)
- The Russian Military Today and Tomorrow: Essays in Memory of Mary FitzgeraldDocument474 pagesThe Russian Military Today and Tomorrow: Essays in Memory of Mary FitzgeraldSSI-Strategic Studies Institute-US Army War College100% (1)
- Punsalan, Jr. vs. Vda. de LacsamanaDocument11 pagesPunsalan, Jr. vs. Vda. de LacsamanaLoubert BartolomeNo ratings yet
- Group2 Non Executive ResultsDocument3 pagesGroup2 Non Executive ResultsGottimukkala MuralikrishnaNo ratings yet
- Writing Project: A. Write A 800 - 1,000 Words Essay or Monograph in A Word Processor in FormatDocument4 pagesWriting Project: A. Write A 800 - 1,000 Words Essay or Monograph in A Word Processor in FormatEbri OjeNo ratings yet
- Examen Blanc Et Corrige 3ASLLE Anglais 2e Sujet 2017Document4 pagesExamen Blanc Et Corrige 3ASLLE Anglais 2e Sujet 2017dila sailNo ratings yet
- Types of Mutual FundDocument5 pagesTypes of Mutual FundGourav BulandiNo ratings yet
- My Job at The Crescent Falls Diner and EssayDocument6 pagesMy Job at The Crescent Falls Diner and EssayAsya Faudhatul InayyahNo ratings yet
- Mass Transfer in Fermentation ProcessDocument5 pagesMass Transfer in Fermentation ProcessSimone Bassan Zuicker ElizeuNo ratings yet
- RunEco EP600 Datasheet 2018Document2 pagesRunEco EP600 Datasheet 2018widnu wirasetiaNo ratings yet
- F5 Exam Report June 2012Document3 pagesF5 Exam Report June 2012Muhammad Khaleel RashidNo ratings yet
- Lucies Farm Data Protection ComplaintDocument186 pagesLucies Farm Data Protection ComplaintcraigwalshNo ratings yet
- (Lovebook care - Anh) Đề thi thử THPTQG trường THPT Chuyên Cao Bằng lần 1Document16 pages(Lovebook care - Anh) Đề thi thử THPTQG trường THPT Chuyên Cao Bằng lần 1Dương Viết ĐạtNo ratings yet
- International Documentary Festival of Ierapetra Awards - 2016 ProgrammeDocument26 pagesInternational Documentary Festival of Ierapetra Awards - 2016 ProgrammeZois PagNo ratings yet
- Nanda 1Document4 pagesNanda 1Ethel GeorgeNo ratings yet
- Java Cheat Sheet & Quick ReferenceDocument16 pagesJava Cheat Sheet & Quick Referencedad dunnoNo ratings yet
- Passive Form (1) This Test Comes From - The Site To Learn English (Test N°5733)Document2 pagesPassive Form (1) This Test Comes From - The Site To Learn English (Test N°5733)Maria Rajendran MNo ratings yet
- 11th Bio NotesDocument167 pages11th Bio NotesKomalNo ratings yet
- Passive VoiceDocument2 pagesPassive VoiceJoseph HopperNo ratings yet