
05 Tens
05 Tens
You might also like
- Medium Frequency CurrentsDocument24 pagesMedium Frequency CurrentsUmarasad100% (1)
- elecrotherapyد0سعد328250476Document46 pageselecrotherapyد0سعد328250476Syeda Fatima AzmatNo ratings yet
- 7 - Interrupted Direct CurrentDocument59 pages7 - Interrupted Direct CurrentAsad Chaudhary100% (12)
- Pea Electrical Curents For Pain ControlDocument2 pagesPea Electrical Curents For Pain Controlemmanuel.payoNo ratings yet
- Pain Modulation, Pain Control Gate Theory and TENSDocument17 pagesPain Modulation, Pain Control Gate Theory and TENSMeerub ShakilNo ratings yet
- 04/19/2020 Misha Ansari, PT 1Document28 pages04/19/2020 Misha Ansari, PT 1Venkata Nagaraj MummadisettyNo ratings yet
- TensDocument55 pagesTensbikedet268No ratings yet
- Presented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VDocument20 pagesPresented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VAngelic khanNo ratings yet
- High Voltage Pulsed CurrentDocument17 pagesHigh Voltage Pulsed Currentbikedet268No ratings yet
- T.E.N.S. Trancutaneous Electrical Nerve StimulationDocument19 pagesT.E.N.S. Trancutaneous Electrical Nerve Stimulationaarya12No ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation)Document34 pagesTENS (Transcutaneous Electrical Nerve Stimulation)Praneetha NouduriNo ratings yet
- TensDocument3 pagesTensDavid LópezNo ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation) : ElectrotherapyDocument38 pagesTENS (Transcutaneous Electrical Nerve Stimulation) : ElectrotherapyArshad ShaikhNo ratings yet
- Therapeutic Electrical ModalitiesDocument105 pagesTherapeutic Electrical ModalitiesDewan PTNo ratings yet
- Medium Frequency: Interferential TherapyDocument31 pagesMedium Frequency: Interferential TherapyjothiNo ratings yet
- DR Sapna Ali Khan (PT) DPT, MSPTDocument32 pagesDR Sapna Ali Khan (PT) DPT, MSPTCHANGEZ KHAN SARDARNo ratings yet
- Transcutaneus Electrical Nerve Stimulation: Mansi TrivediDocument49 pagesTranscutaneus Electrical Nerve Stimulation: Mansi TrivediAkshaya MistryNo ratings yet
- TensDocument29 pagesTensSwati TiwariNo ratings yet
- Andres Bello University Faculty of Rehabilitation Sciences School of KinesiologyDocument10 pagesAndres Bello University Faculty of Rehabilitation Sciences School of KinesiologyAkkipero123No ratings yet
- IFCDocument22 pagesIFCJulia SalvioNo ratings yet
- Transcutaneous Electrical Nerve Stimulation (TENS) : Physics and PhysiologyDocument6 pagesTranscutaneous Electrical Nerve Stimulation (TENS) : Physics and Physiologydrng48No ratings yet
- Tens LectureDocument19 pagesTens LectureAni Fran SolarNo ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation)Document17 pagesTENS (Transcutaneous Electrical Nerve Stimulation)Ajay Pal NattNo ratings yet
- ELECTRO-ANALGESIA and TENSDocument31 pagesELECTRO-ANALGESIA and TENSManibhadra PandaNo ratings yet
- Electrical StimulationDocument3 pagesElectrical StimulationMarilia FarensenaNo ratings yet
- 13.electrical Stimulation of Nerve and MuscleDocument45 pages13.electrical Stimulation of Nerve and MuscleFaisal Mehboob100% (2)
- Transcutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and EvidenceDocument5 pagesTranscutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and EvidenceLuis Alvarez MoralesNo ratings yet
- Di Dynamic TENSDocument25 pagesDi Dynamic TENSfaiza khurshidNo ratings yet
- (TENS) Anas SirDocument28 pages(TENS) Anas SirrabeyaNo ratings yet
- TENS Lec 5 - 240310 - 223247Document25 pagesTENS Lec 5 - 240310 - 223247memo.dawdNo ratings yet
- High Voltage Galvanic StimulationDocument4 pagesHigh Voltage Galvanic StimulationmichidoodleNo ratings yet
- TENSProtocolby DR Deirdre WalshDocument15 pagesTENSProtocolby DR Deirdre WalshGuy Hill100% (1)
- Interferential Therapy: DefinitionDocument9 pagesInterferential Therapy: DefinitionLowell QuadrosNo ratings yet
- Electrical Muscle StimulationDocument11 pagesElectrical Muscle StimulationElif66No ratings yet
- Medium Frequency CurrentsDocument24 pagesMedium Frequency CurrentsUmarasadNo ratings yet
- 06 Interference CurrentDocument5 pages06 Interference Current楊畯凱No ratings yet
- Intro To CurrentsDocument122 pagesIntro To CurrentsDodo JuniorNo ratings yet
- 07 High Voltage Pulsed CurrentDocument4 pages07 High Voltage Pulsed Current楊畯凱No ratings yet
- Interferential Therapy.Document23 pagesInterferential Therapy.Salman KhanNo ratings yet
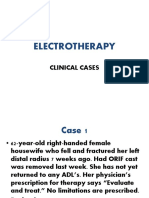
- Electrotherapy: Clinical CasesDocument18 pagesElectrotherapy: Clinical CasesjothiNo ratings yet
- Lecture 6 - Ift, MMF and TensDocument36 pagesLecture 6 - Ift, MMF and Tenscreativefire345No ratings yet
- Electrotherapy 1 Viva QuestionsDocument9 pagesElectrotherapy 1 Viva QuestionsAmaan Shafique100% (2)
- Electronic Muscle StimulationDocument9 pagesElectronic Muscle StimulationAnoop Viswanath100% (1)
- Interferential Therapy LectureDocument24 pagesInterferential Therapy LectureSalman KhanNo ratings yet
- Enraf-Nonius Endomed 484 EN PDFDocument7 pagesEnraf-Nonius Endomed 484 EN PDFAgustya PutriNo ratings yet
- Galvano Terapy Topic - 6Document3 pagesGalvano Terapy Topic - 6Gigi CotoraNo ratings yet
- Batch 06 - Ift PresentationDocument45 pagesBatch 06 - Ift PresentationANANYA MAHARANANo ratings yet
- Lecture 5 - Introduction To Electrical StimulationDocument49 pagesLecture 5 - Introduction To Electrical Stimulationcreativefire345No ratings yet
- Transcutaneous Electrical Nerve StimulationDocument19 pagesTranscutaneous Electrical Nerve StimulationSaleha ZainNo ratings yet
- TensDocument28 pagesTensPaul VkNo ratings yet
- Tens by Sagar Naik, PTDocument17 pagesTens by Sagar Naik, PTkapokNo ratings yet
- Khubab AhmadDocument18 pagesKhubab AhmadRana M ArslanNo ratings yet
- TENS Electrode Placement PDFDocument34 pagesTENS Electrode Placement PDFjamesmhebertNo ratings yet
- Diadynamic CurrentDocument30 pagesDiadynamic CurrentvladNo ratings yet
- DownloadDocument11 pagesDownloadChristopher Chew Dian MingNo ratings yet
- Design Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachFrom EverandDesign Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachNo ratings yet
- Bioactivity study of modified curcumin loaded polymeric nanoparticlesFrom EverandBioactivity study of modified curcumin loaded polymeric nanoparticlesNo ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- Posterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal OriginDocument4 pagesPosterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal Origin楊畯凱No ratings yet
- 01 Musculoskeletal AssessmentDocument10 pages01 Musculoskeletal Assessment楊畯凱100% (1)
- 03 Principle of Electrical StimulationDocument5 pages03 Principle of Electrical Stimulation楊畯凱No ratings yet
- 09 Cervical Spine 1Document14 pages09 Cervical Spine 1楊畯凱No ratings yet
- 10 Thoracolumbar Spine 3Document4 pages10 Thoracolumbar Spine 3楊畯凱No ratings yet
- 02 Retraining Basic and Instrumental Activities of Daily LicingDocument5 pages02 Retraining Basic and Instrumental Activities of Daily Licing楊畯凱No ratings yet
- 04 Electrical Stimulation To Increase Functional ActivityDocument4 pages04 Electrical Stimulation To Increase Functional Activity楊畯凱No ratings yet
- 14 Emergency Sport AssessmentDocument7 pages14 Emergency Sport Assessment楊畯凱No ratings yet
- Shoulder Special TestDocument2 pagesShoulder Special Test楊畯凱No ratings yet
- Shoe and Foot OrthosisDocument9 pagesShoe and Foot Orthosis楊畯凱No ratings yet
- Spinal OrthosisDocument6 pagesSpinal Orthosis楊畯凱No ratings yet
- KneeDocument10 pagesKnee楊畯凱No ratings yet
- Ankle Foot OrthosisDocument4 pagesAnkle Foot Orthosis楊畯凱No ratings yet
- CHAPTER 25 Nitrogen Acquisition and Amino Acid Metabolism I (Amino Acid Synthesis)Document12 pagesCHAPTER 25 Nitrogen Acquisition and Amino Acid Metabolism I (Amino Acid Synthesis)楊畯凱No ratings yet
- Knee and Hip OrthosisDocument4 pagesKnee and Hip Orthosis楊畯凱No ratings yet
- CHAPTER 23 Fatty Acid CatabolismDocument9 pagesCHAPTER 23 Fatty Acid Catabolism楊畯凱No ratings yet
- CHAPTER 24 Lipid BiosynthesisDocument16 pagesCHAPTER 24 Lipid Biosynthesis楊畯凱No ratings yet
- CHAPTER 21 PhotosynthesisDocument12 pagesCHAPTER 21 Photosynthesis楊畯凱No ratings yet
- CHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate PathwayDocument12 pagesCHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate Pathway楊畯凱No ratings yet
- CHAPTER 19 Tricarboxylic Acid CycleDocument11 pagesCHAPTER 19 Tricarboxylic Acid Cycle楊畯凱No ratings yet
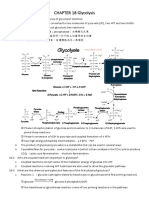
- CHAPTER 18 GlycolysisDocument10 pagesCHAPTER 18 Glycolysis楊畯凱No ratings yet
- CHAPTER 17 The Metabolism An OverviewDocument10 pagesCHAPTER 17 The Metabolism An Overview楊畯凱No ratings yet
- CHAPTER 7 Carbohydrates and The Glyconjugates of Cell SurfaceDocument14 pagesCHAPTER 7 Carbohydrates and The Glyconjugates of Cell Surface楊畯凱No ratings yet
- Escala Balance PPASDocument4 pagesEscala Balance PPASMoraima SoriaNo ratings yet
- AnswerKey ENGLISH Module3 TeachersDocument1 pageAnswerKey ENGLISH Module3 TeachersDionelda AbearNo ratings yet
- Functional Training ExploredDocument16 pagesFunctional Training ExploredOfelia MCoachNo ratings yet
- (Ebook PDF) Equine Ophthalmology 3Rd Edition by Brian C. GilgerDocument41 pages(Ebook PDF) Equine Ophthalmology 3Rd Edition by Brian C. Gilgerjessica.rohrbach136100% (56)
- MS FileDocument8 pagesMS FileFARAH MOHAMMEDNo ratings yet
- Cervical Assessment Form FILLABLE Jun 2020 PDFDocument2 pagesCervical Assessment Form FILLABLE Jun 2020 PDFsanavoraNo ratings yet
- Migraine DiaryDocument1 pageMigraine DiaryEmily KirbyNo ratings yet
- Mock Doc-6Document6 pagesMock Doc-6Heena KhanNo ratings yet
- Detailed Lesson Plan in Nervous SystemDocument8 pagesDetailed Lesson Plan in Nervous Systemjonelllantero032No ratings yet
- 3946 - Anatomy and Physiology V13Document4 pages3946 - Anatomy and Physiology V13monique baptisteNo ratings yet
- Neurological Examination in Spinal Cord Injury NewDocument18 pagesNeurological Examination in Spinal Cord Injury NewPratyush RanjanNo ratings yet
- Book 2 (74-143)Document70 pagesBook 2 (74-143)Shaik NisaNo ratings yet
- NERVOUS SYSTEM-WPS OfficeDocument15 pagesNERVOUS SYSTEM-WPS OfficeJoshua DauzNo ratings yet
- Special Senses ActivityDocument8 pagesSpecial Senses ActivityJerene Denzil NacarNo ratings yet
- HH-I-70 VP Shunt - Care at HomeDocument2 pagesHH-I-70 VP Shunt - Care at HomeIbraheim AlwaraqiNo ratings yet
- The Development of Self and Identity in AdolescenceDocument7 pagesThe Development of Self and Identity in AdolescenceCervettoNo ratings yet
- Muscular SystemDocument9 pagesMuscular SystemFrely Jane PanilagaoNo ratings yet
- Parasympathomimetic AgentsDocument26 pagesParasympathomimetic Agentsrushikesh ugaleNo ratings yet
- Development and Plasticity of The Brain: Chapter OutlineDocument5 pagesDevelopment and Plasticity of The Brain: Chapter OutlineSusie SofrankoNo ratings yet
- PARALLEL@PERFORMANCEPERDEV - Q1 - Mod5 - The Brain Parts Functions and Societal RelationshipDocument3 pagesPARALLEL@PERFORMANCEPERDEV - Q1 - Mod5 - The Brain Parts Functions and Societal RelationshipGynnel NicanorNo ratings yet
- Lab Report NewDocument3 pagesLab Report Newhacebe2685No ratings yet
- Medical ChemistryDocument32 pagesMedical Chemistryabhishek kumar singhNo ratings yet
- Neurolingusitics: Brain & Languages Language & Brain Development The Modular MindDocument1 pageNeurolingusitics: Brain & Languages Language & Brain Development The Modular MindhamizahNo ratings yet
- Managing Lockjaw Disorders in Dogs: TrismusDocument14 pagesManaging Lockjaw Disorders in Dogs: TrismusmiloNo ratings yet
- Central Nervous System ExaminationDocument25 pagesCentral Nervous System ExaminationMaryem RaheemNo ratings yet
- WA0044.encDocument40 pagesWA0044.encmalfed adrianoNo ratings yet
- Ear Histology SeminarDocument30 pagesEar Histology Seminarpeter GireNo ratings yet
- Embryology of EarDocument29 pagesEmbryology of Earaishagani04No ratings yet
- Ebook Fundamental Neuroscience For Basic and Clinical Applications PDF Full Chapter PDFDocument67 pagesEbook Fundamental Neuroscience For Basic and Clinical Applications PDF Full Chapter PDFbertha.senior550100% (39)
- Reading: Part A - Text Booklet: Bird Brains: TextsDocument7 pagesReading: Part A - Text Booklet: Bird Brains: TextsSagiraju SrinuNo ratings yet















































































































Download as pdf or txt
You might also like
- Medium Frequency CurrentsDocument24 pagesMedium Frequency CurrentsUmarasad100% (1)
- elecrotherapyد0سعد328250476Document46 pageselecrotherapyد0سعد328250476Syeda Fatima AzmatNo ratings yet
- 7 - Interrupted Direct CurrentDocument59 pages7 - Interrupted Direct CurrentAsad Chaudhary100% (12)
- Pea Electrical Curents For Pain ControlDocument2 pagesPea Electrical Curents For Pain Controlemmanuel.payoNo ratings yet
- Pain Modulation, Pain Control Gate Theory and TENSDocument17 pagesPain Modulation, Pain Control Gate Theory and TENSMeerub ShakilNo ratings yet
- 04/19/2020 Misha Ansari, PT 1Document28 pages04/19/2020 Misha Ansari, PT 1Venkata Nagaraj MummadisettyNo ratings yet
- TensDocument55 pagesTensbikedet268No ratings yet
- Presented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VDocument20 pagesPresented by Yasha Ali Bangash & Pashmina Khan DPT Batch Ii Semester VAngelic khanNo ratings yet
- High Voltage Pulsed CurrentDocument17 pagesHigh Voltage Pulsed Currentbikedet268No ratings yet
- T.E.N.S. Trancutaneous Electrical Nerve StimulationDocument19 pagesT.E.N.S. Trancutaneous Electrical Nerve Stimulationaarya12No ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation)Document34 pagesTENS (Transcutaneous Electrical Nerve Stimulation)Praneetha NouduriNo ratings yet
- TensDocument3 pagesTensDavid LópezNo ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation) : ElectrotherapyDocument38 pagesTENS (Transcutaneous Electrical Nerve Stimulation) : ElectrotherapyArshad ShaikhNo ratings yet
- Therapeutic Electrical ModalitiesDocument105 pagesTherapeutic Electrical ModalitiesDewan PTNo ratings yet
- Medium Frequency: Interferential TherapyDocument31 pagesMedium Frequency: Interferential TherapyjothiNo ratings yet
- DR Sapna Ali Khan (PT) DPT, MSPTDocument32 pagesDR Sapna Ali Khan (PT) DPT, MSPTCHANGEZ KHAN SARDARNo ratings yet
- Transcutaneus Electrical Nerve Stimulation: Mansi TrivediDocument49 pagesTranscutaneus Electrical Nerve Stimulation: Mansi TrivediAkshaya MistryNo ratings yet
- TensDocument29 pagesTensSwati TiwariNo ratings yet
- Andres Bello University Faculty of Rehabilitation Sciences School of KinesiologyDocument10 pagesAndres Bello University Faculty of Rehabilitation Sciences School of KinesiologyAkkipero123No ratings yet
- IFCDocument22 pagesIFCJulia SalvioNo ratings yet
- Transcutaneous Electrical Nerve Stimulation (TENS) : Physics and PhysiologyDocument6 pagesTranscutaneous Electrical Nerve Stimulation (TENS) : Physics and Physiologydrng48No ratings yet
- Tens LectureDocument19 pagesTens LectureAni Fran SolarNo ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation)Document17 pagesTENS (Transcutaneous Electrical Nerve Stimulation)Ajay Pal NattNo ratings yet
- ELECTRO-ANALGESIA and TENSDocument31 pagesELECTRO-ANALGESIA and TENSManibhadra PandaNo ratings yet
- Electrical StimulationDocument3 pagesElectrical StimulationMarilia FarensenaNo ratings yet
- 13.electrical Stimulation of Nerve and MuscleDocument45 pages13.electrical Stimulation of Nerve and MuscleFaisal Mehboob100% (2)
- Transcutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and EvidenceDocument5 pagesTranscutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and EvidenceLuis Alvarez MoralesNo ratings yet
- Di Dynamic TENSDocument25 pagesDi Dynamic TENSfaiza khurshidNo ratings yet
- (TENS) Anas SirDocument28 pages(TENS) Anas SirrabeyaNo ratings yet
- TENS Lec 5 - 240310 - 223247Document25 pagesTENS Lec 5 - 240310 - 223247memo.dawdNo ratings yet
- High Voltage Galvanic StimulationDocument4 pagesHigh Voltage Galvanic StimulationmichidoodleNo ratings yet
- TENSProtocolby DR Deirdre WalshDocument15 pagesTENSProtocolby DR Deirdre WalshGuy Hill100% (1)
- Interferential Therapy: DefinitionDocument9 pagesInterferential Therapy: DefinitionLowell QuadrosNo ratings yet
- Electrical Muscle StimulationDocument11 pagesElectrical Muscle StimulationElif66No ratings yet
- Medium Frequency CurrentsDocument24 pagesMedium Frequency CurrentsUmarasadNo ratings yet
- 06 Interference CurrentDocument5 pages06 Interference Current楊畯凱No ratings yet
- Intro To CurrentsDocument122 pagesIntro To CurrentsDodo JuniorNo ratings yet
- 07 High Voltage Pulsed CurrentDocument4 pages07 High Voltage Pulsed Current楊畯凱No ratings yet
- Interferential Therapy.Document23 pagesInterferential Therapy.Salman KhanNo ratings yet
- Electrotherapy: Clinical CasesDocument18 pagesElectrotherapy: Clinical CasesjothiNo ratings yet
- Lecture 6 - Ift, MMF and TensDocument36 pagesLecture 6 - Ift, MMF and Tenscreativefire345No ratings yet
- Electrotherapy 1 Viva QuestionsDocument9 pagesElectrotherapy 1 Viva QuestionsAmaan Shafique100% (2)
- Electronic Muscle StimulationDocument9 pagesElectronic Muscle StimulationAnoop Viswanath100% (1)
- Interferential Therapy LectureDocument24 pagesInterferential Therapy LectureSalman KhanNo ratings yet
- Enraf-Nonius Endomed 484 EN PDFDocument7 pagesEnraf-Nonius Endomed 484 EN PDFAgustya PutriNo ratings yet
- Galvano Terapy Topic - 6Document3 pagesGalvano Terapy Topic - 6Gigi CotoraNo ratings yet
- Batch 06 - Ift PresentationDocument45 pagesBatch 06 - Ift PresentationANANYA MAHARANANo ratings yet
- Lecture 5 - Introduction To Electrical StimulationDocument49 pagesLecture 5 - Introduction To Electrical Stimulationcreativefire345No ratings yet
- Transcutaneous Electrical Nerve StimulationDocument19 pagesTranscutaneous Electrical Nerve StimulationSaleha ZainNo ratings yet
- TensDocument28 pagesTensPaul VkNo ratings yet
- Tens by Sagar Naik, PTDocument17 pagesTens by Sagar Naik, PTkapokNo ratings yet
- Khubab AhmadDocument18 pagesKhubab AhmadRana M ArslanNo ratings yet
- TENS Electrode Placement PDFDocument34 pagesTENS Electrode Placement PDFjamesmhebertNo ratings yet
- Diadynamic CurrentDocument30 pagesDiadynamic CurrentvladNo ratings yet
- DownloadDocument11 pagesDownloadChristopher Chew Dian MingNo ratings yet
- Design Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachFrom EverandDesign Development and Analysis of a Nerve Conduction Study System An Auto Controlled Biofeedback ApproachNo ratings yet
- Bioactivity study of modified curcumin loaded polymeric nanoparticlesFrom EverandBioactivity study of modified curcumin loaded polymeric nanoparticlesNo ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- Posterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal OriginDocument4 pagesPosterior, Lateral, and Anterior Hip Pain Due To Musculoskeletal Origin楊畯凱No ratings yet
- 01 Musculoskeletal AssessmentDocument10 pages01 Musculoskeletal Assessment楊畯凱100% (1)
- 03 Principle of Electrical StimulationDocument5 pages03 Principle of Electrical Stimulation楊畯凱No ratings yet
- 09 Cervical Spine 1Document14 pages09 Cervical Spine 1楊畯凱No ratings yet
- 10 Thoracolumbar Spine 3Document4 pages10 Thoracolumbar Spine 3楊畯凱No ratings yet
- 02 Retraining Basic and Instrumental Activities of Daily LicingDocument5 pages02 Retraining Basic and Instrumental Activities of Daily Licing楊畯凱No ratings yet
- 04 Electrical Stimulation To Increase Functional ActivityDocument4 pages04 Electrical Stimulation To Increase Functional Activity楊畯凱No ratings yet
- 14 Emergency Sport AssessmentDocument7 pages14 Emergency Sport Assessment楊畯凱No ratings yet
- Shoulder Special TestDocument2 pagesShoulder Special Test楊畯凱No ratings yet
- Shoe and Foot OrthosisDocument9 pagesShoe and Foot Orthosis楊畯凱No ratings yet
- Spinal OrthosisDocument6 pagesSpinal Orthosis楊畯凱No ratings yet
- KneeDocument10 pagesKnee楊畯凱No ratings yet
- Ankle Foot OrthosisDocument4 pagesAnkle Foot Orthosis楊畯凱No ratings yet
- CHAPTER 25 Nitrogen Acquisition and Amino Acid Metabolism I (Amino Acid Synthesis)Document12 pagesCHAPTER 25 Nitrogen Acquisition and Amino Acid Metabolism I (Amino Acid Synthesis)楊畯凱No ratings yet
- Knee and Hip OrthosisDocument4 pagesKnee and Hip Orthosis楊畯凱No ratings yet
- CHAPTER 23 Fatty Acid CatabolismDocument9 pagesCHAPTER 23 Fatty Acid Catabolism楊畯凱No ratings yet
- CHAPTER 24 Lipid BiosynthesisDocument16 pagesCHAPTER 24 Lipid Biosynthesis楊畯凱No ratings yet
- CHAPTER 21 PhotosynthesisDocument12 pagesCHAPTER 21 Photosynthesis楊畯凱No ratings yet
- CHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate PathwayDocument12 pagesCHAPTER 22 Gluconeogenesis, Glycogen Metabolism, and The Pentose Phosphate Pathway楊畯凱No ratings yet
- CHAPTER 19 Tricarboxylic Acid CycleDocument11 pagesCHAPTER 19 Tricarboxylic Acid Cycle楊畯凱No ratings yet
- CHAPTER 18 GlycolysisDocument10 pagesCHAPTER 18 Glycolysis楊畯凱No ratings yet
- CHAPTER 17 The Metabolism An OverviewDocument10 pagesCHAPTER 17 The Metabolism An Overview楊畯凱No ratings yet
- CHAPTER 7 Carbohydrates and The Glyconjugates of Cell SurfaceDocument14 pagesCHAPTER 7 Carbohydrates and The Glyconjugates of Cell Surface楊畯凱No ratings yet
- Escala Balance PPASDocument4 pagesEscala Balance PPASMoraima SoriaNo ratings yet
- AnswerKey ENGLISH Module3 TeachersDocument1 pageAnswerKey ENGLISH Module3 TeachersDionelda AbearNo ratings yet
- Functional Training ExploredDocument16 pagesFunctional Training ExploredOfelia MCoachNo ratings yet
- (Ebook PDF) Equine Ophthalmology 3Rd Edition by Brian C. GilgerDocument41 pages(Ebook PDF) Equine Ophthalmology 3Rd Edition by Brian C. Gilgerjessica.rohrbach136100% (56)
- MS FileDocument8 pagesMS FileFARAH MOHAMMEDNo ratings yet
- Cervical Assessment Form FILLABLE Jun 2020 PDFDocument2 pagesCervical Assessment Form FILLABLE Jun 2020 PDFsanavoraNo ratings yet
- Migraine DiaryDocument1 pageMigraine DiaryEmily KirbyNo ratings yet
- Mock Doc-6Document6 pagesMock Doc-6Heena KhanNo ratings yet
- Detailed Lesson Plan in Nervous SystemDocument8 pagesDetailed Lesson Plan in Nervous Systemjonelllantero032No ratings yet
- 3946 - Anatomy and Physiology V13Document4 pages3946 - Anatomy and Physiology V13monique baptisteNo ratings yet
- Neurological Examination in Spinal Cord Injury NewDocument18 pagesNeurological Examination in Spinal Cord Injury NewPratyush RanjanNo ratings yet
- Book 2 (74-143)Document70 pagesBook 2 (74-143)Shaik NisaNo ratings yet
- NERVOUS SYSTEM-WPS OfficeDocument15 pagesNERVOUS SYSTEM-WPS OfficeJoshua DauzNo ratings yet
- Special Senses ActivityDocument8 pagesSpecial Senses ActivityJerene Denzil NacarNo ratings yet
- HH-I-70 VP Shunt - Care at HomeDocument2 pagesHH-I-70 VP Shunt - Care at HomeIbraheim AlwaraqiNo ratings yet
- The Development of Self and Identity in AdolescenceDocument7 pagesThe Development of Self and Identity in AdolescenceCervettoNo ratings yet
- Muscular SystemDocument9 pagesMuscular SystemFrely Jane PanilagaoNo ratings yet
- Parasympathomimetic AgentsDocument26 pagesParasympathomimetic Agentsrushikesh ugaleNo ratings yet
- Development and Plasticity of The Brain: Chapter OutlineDocument5 pagesDevelopment and Plasticity of The Brain: Chapter OutlineSusie SofrankoNo ratings yet
- PARALLEL@PERFORMANCEPERDEV - Q1 - Mod5 - The Brain Parts Functions and Societal RelationshipDocument3 pagesPARALLEL@PERFORMANCEPERDEV - Q1 - Mod5 - The Brain Parts Functions and Societal RelationshipGynnel NicanorNo ratings yet
- Lab Report NewDocument3 pagesLab Report Newhacebe2685No ratings yet
- Medical ChemistryDocument32 pagesMedical Chemistryabhishek kumar singhNo ratings yet
- Neurolingusitics: Brain & Languages Language & Brain Development The Modular MindDocument1 pageNeurolingusitics: Brain & Languages Language & Brain Development The Modular MindhamizahNo ratings yet
- Managing Lockjaw Disorders in Dogs: TrismusDocument14 pagesManaging Lockjaw Disorders in Dogs: TrismusmiloNo ratings yet
- Central Nervous System ExaminationDocument25 pagesCentral Nervous System ExaminationMaryem RaheemNo ratings yet
- WA0044.encDocument40 pagesWA0044.encmalfed adrianoNo ratings yet
- Ear Histology SeminarDocument30 pagesEar Histology Seminarpeter GireNo ratings yet
- Embryology of EarDocument29 pagesEmbryology of Earaishagani04No ratings yet
- Ebook Fundamental Neuroscience For Basic and Clinical Applications PDF Full Chapter PDFDocument67 pagesEbook Fundamental Neuroscience For Basic and Clinical Applications PDF Full Chapter PDFbertha.senior550100% (39)
- Reading: Part A - Text Booklet: Bird Brains: TextsDocument7 pagesReading: Part A - Text Booklet: Bird Brains: TextsSagiraju SrinuNo ratings yet