Download as pdf or txt
You might also like
- Olympus Mju-1 Parts ListDocument8 pagesOlympus Mju-1 Parts ListMalaNo ratings yet
- Truck Crane 1: GT-900XLDocument270 pagesTruck Crane 1: GT-900XLJulio Ramos100% (1)
- Colloidalt Gold and Silver - Production of Colloidal Gold With Electrolysis and Green SynthesisDocument14 pagesColloidalt Gold and Silver - Production of Colloidal Gold With Electrolysis and Green SynthesisDevon Narok100% (1)
- Imágenes de RM de Trauma MuscularDocument23 pagesImágenes de RM de Trauma Muscularmicamart.94No ratings yet
- Mendiguchia2012 PDFDocument10 pagesMendiguchia2012 PDFJose Antonio Fernández GómezNo ratings yet
- 4 Imaging Review of Groin Pain in Elite Athletes An Anatomic Approach To Imaging Findings 3214658300Document11 pages4 Imaging Review of Groin Pain in Elite Athletes An Anatomic Approach To Imaging Findings 3214658300César ArveláezNo ratings yet
- 2021 Article 572Document9 pages2021 Article 572Ous TNo ratings yet
- Biomechanics, Evaluation, and Management of Subaxial Cervical Spine Injuries - A Comprehensive Review of The LiteratureDocument9 pagesBiomechanics, Evaluation, and Management of Subaxial Cervical Spine Injuries - A Comprehensive Review of The Literaturebruna.c.moscatelNo ratings yet
- Explanation Using: Injuries PreviouslyDocument7 pagesExplanation Using: Injuries PreviouslyjannilshansenNo ratings yet
- Fracturas PatologicasDocument20 pagesFracturas PatologicasSamantha AriasNo ratings yet
- Lesão Isquiotibiais Metodos e Exercícios de Recuperação - Métodos de DiagnósticoDocument15 pagesLesão Isquiotibiais Metodos e Exercícios de Recuperação - Métodos de DiagnósticojoaoaesfigueiredoNo ratings yet
- BrJSportsMed 2012 Mendiguchia Bjsports 2012 091250Document11 pagesBrJSportsMed 2012 Mendiguchia Bjsports 2012 091250emavassNo ratings yet
- Meniscal Injury: I. Basic Science and EvaluationDocument9 pagesMeniscal Injury: I. Basic Science and EvaluationJulioNo ratings yet
- Hamstring RehabilitationDocument29 pagesHamstring RehabilitationOscar NgNo ratings yet
- Mendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFDocument11 pagesMendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFJuan PalomoNo ratings yet
- Wang 2020Document9 pagesWang 2020JoseNo ratings yet
- HHS Public Access: Hamstring Injuries in The Athlete: Diagnosis, Treatment, and Return To PlayDocument17 pagesHHS Public Access: Hamstring Injuries in The Athlete: Diagnosis, Treatment, and Return To PlayhanifaNo ratings yet
- MCL RehaDocument15 pagesMCL RehaH HanNo ratings yet
- Fractures of Distal Radius An OverviewDocument8 pagesFractures of Distal Radius An OverviewNandani NarineNo ratings yet
- Imaging of The Athletic HipDocument6 pagesImaging of The Athletic HipAbdul Wahid ShaikhNo ratings yet
- Chronic Groin Pain in An Amateur Soccer Player: Case ReportDocument2 pagesChronic Groin Pain in An Amateur Soccer Player: Case ReportAndreas Arie WidiadiaksaNo ratings yet
- Br+J+Sports+Med 2012 Mendiguchia Bjsports 2012 091250Document11 pagesBr+J+Sports+Med 2012 Mendiguchia Bjsports 2012 091250Kostas LiougkosNo ratings yet
- Subtrochanteric Femur Fractures: Current Review of ManagementDocument7 pagesSubtrochanteric Femur Fractures: Current Review of ManagementErmiNo ratings yet
- Lisfranc Fracture Dislocation Current TreatmentDocument15 pagesLisfranc Fracture Dislocation Current TreatmentLoy LoyNo ratings yet
- Imaging in Football Medicine: Perennial FavouritesDocument11 pagesImaging in Football Medicine: Perennial FavouritesTeuku Ona AriefNo ratings yet
- Rehabilitation of Knee Injuries: Robert C. Manske and Mark V. PaternoDocument23 pagesRehabilitation of Knee Injuries: Robert C. Manske and Mark V. PaternoYMatosNo ratings yet
- MCL RehaDocument15 pagesMCL RehaIlham Amal MNo ratings yet
- WilliamsDocument12 pagesWilliamsValeriaNo ratings yet
- Fractures of Distal Radius: An Overview: Family PracticeDocument8 pagesFractures of Distal Radius: An Overview: Family Practicesuci triana putriNo ratings yet
- Athletic Injuries of The ThoracicDocument20 pagesAthletic Injuries of The ThoracicGrado CristianNo ratings yet
- Acromioclavicular Joint Injuries: Evidence-Based Treatment: Review ArticleDocument14 pagesAcromioclavicular Joint Injuries: Evidence-Based Treatment: Review ArticleAlejandra JimenezNo ratings yet
- 2016 Article 9341 PDFDocument8 pages2016 Article 9341 PDFJulenda CintarinovaNo ratings yet
- Ankle Sprains: Evaluation, Rehabilitation, and Prevention: Raining Revention AND EhabilitationDocument7 pagesAnkle Sprains: Evaluation, Rehabilitation, and Prevention: Raining Revention AND EhabilitationtanyasisNo ratings yet
- Fractura Cadera 1Document22 pagesFractura Cadera 1Júlia LedesmaNo ratings yet
- 2010 - Elbow Instability - JBJSDocument12 pages2010 - Elbow Instability - JBJSharpreet singhNo ratings yet
- Baltes 2019 Clinical Approach To Common Foot and Ankle Stress Fractures in AthleticsDocument5 pagesBaltes 2019 Clinical Approach To Common Foot and Ankle Stress Fractures in AthleticsKen Van AlsenoyNo ratings yet
- Computerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersDocument11 pagesComputerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersMasithaNo ratings yet
- Management of Pediatric Ankle FracturesDocument10 pagesManagement of Pediatric Ankle FracturesDeborah SalinasNo ratings yet
- Research in Prevention and Rehabilitation of Ham 2017 Journal of Sport and HDocument2 pagesResearch in Prevention and Rehabilitation of Ham 2017 Journal of Sport and HSisi WeeraNo ratings yet
- Common Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauDocument7 pagesCommon Pediatric Elbow Fractures: Erin S. Hart Allison Turner Maurice Albright Brian E. GrottkauFino SopianNo ratings yet
- 2020 Article 9639Document8 pages2020 Article 9639Luis Briones Lau.LiNo ratings yet
- Subtrochanteric Femur Fractures: Asheesh Bedi, MD, T. Toan Le, MDDocument11 pagesSubtrochanteric Femur Fractures: Asheesh Bedi, MD, T. Toan Le, MDMd.Shafiul EzazNo ratings yet
- Initial Management of Acute Spinal Cord Injury: Stephen Bonner MRCP FRCA FFICM Caroline Smith FRCADocument8 pagesInitial Management of Acute Spinal Cord Injury: Stephen Bonner MRCP FRCA FFICM Caroline Smith FRCAMinaz PatelNo ratings yet
- Classification of Pelvic Fractures and Its Clinical RelevanceDocument6 pagesClassification of Pelvic Fractures and Its Clinical RelevanceMohamed AzeemNo ratings yet
- Sports-Related Wrist and Hand Injuries: A ReviewDocument15 pagesSports-Related Wrist and Hand Injuries: A ReviewMaddy WolsmenNo ratings yet
- Lisfranc InjuryDocument99 pagesLisfranc InjurySubodh PathakNo ratings yet
- 1 s2.0 S1440244023005091 MainDocument7 pages1 s2.0 S1440244023005091 MainDeivisonNo ratings yet
- Mar2012 CC LaPradeDocument13 pagesMar2012 CC LaPradeJavierLarenasNo ratings yet
- Stav SoucasnyDocument14 pagesStav SoucasnyTommysNo ratings yet
- Muscular Calf Injuries in RunnersDocument5 pagesMuscular Calf Injuries in RunnersDaniel Damacena FisioterapiaNo ratings yet
- Jsa 0000000000000162Document8 pagesJsa 0000000000000162Mohammed AliNo ratings yet
- Orthopaedic Traumatology Fundamental Principles AnDocument9 pagesOrthopaedic Traumatology Fundamental Principles AnZain Ul AbidinNo ratings yet
- Kfuri 2018Document12 pagesKfuri 2018Arthur TeixeiraNo ratings yet
- Knee Pain H and P PDFDocument6 pagesKnee Pain H and P PDFKKNo ratings yet
- 10.1177 1941738111429419Document12 pages10.1177 1941738111429419refniNo ratings yet
- Classifications in Brief, Thoracolumbar Injury Classification and Injury Severity Score System (Tlics)Document7 pagesClassifications in Brief, Thoracolumbar Injury Classification and Injury Severity Score System (Tlics)armapecaNo ratings yet
- JAAOSNov2017-The Posteromedial Corner of The Knee Anatomy-DOLDDocument11 pagesJAAOSNov2017-The Posteromedial Corner of The Knee Anatomy-DOLDseatrrtleNo ratings yet
- Safe Management of Acute Cervical Spine Injuries: Instructional Lecture: TraumaDocument11 pagesSafe Management of Acute Cervical Spine Injuries: Instructional Lecture: TraumaDonate 049No ratings yet
- An Overview of The Named Wrist Fractures: Jenna A. Saxton, DO, Justin R. Montgomery, MD, and Paul J. Spicer, MDDocument6 pagesAn Overview of The Named Wrist Fractures: Jenna A. Saxton, DO, Justin R. Montgomery, MD, and Paul J. Spicer, MDmedicNo ratings yet
- TraumaDocument51 pagesTraumaKumail KhandwalaNo ratings yet
- Jumper's Knee: Joseph M. David, MS, Pt1Document5 pagesJumper's Knee: Joseph M. David, MS, Pt1Hanako HanabiNo ratings yet
- Stress Analyses Around Holes in Composite Laminates Using Boundary Element MethodDocument10 pagesStress Analyses Around Holes in Composite Laminates Using Boundary Element MethodpdhurveyNo ratings yet
- Fake Braces HarDocument53 pagesFake Braces Harsarinah safli100% (1)
- Acknowledgement: ReferencesDocument7 pagesAcknowledgement: Referencesdwayne420No ratings yet
- Methods For Assessing The Stability of Slopes During Earthquakes-A RetrospectiveDocument20 pagesMethods For Assessing The Stability of Slopes During Earthquakes-A Retrospectiveilijarsk100% (1)
- Material and DesignDocument2 pagesMaterial and DesignrafadannNo ratings yet
- Electrical Work QuatationDocument3 pagesElectrical Work Quatationkiran100% (1)
- Desastres Naturales y Plagas Del Valle ElquiDocument40 pagesDesastres Naturales y Plagas Del Valle ElquiWalter Foral LiebschNo ratings yet
- E-12 Rudder Angle System Sperry RAI PDFDocument116 pagesE-12 Rudder Angle System Sperry RAI PDFAlexandra DuduNo ratings yet
- GE 15 - Week 4 To 5Document26 pagesGE 15 - Week 4 To 5Kent YapNo ratings yet
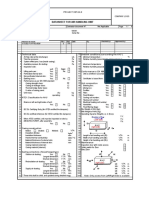
- AHU Datasheet Sample Detailed Page 1 of 6 1635440149Document1 pageAHU Datasheet Sample Detailed Page 1 of 6 1635440149alim khanNo ratings yet
- Teletek Rreater Panel ManualDocument20 pagesTeletek Rreater Panel Manualiphonekaan34No ratings yet
- Mirroring Men and Masculinity in Joanne Harris' Chocolat and The Lollipop ShoesDocument50 pagesMirroring Men and Masculinity in Joanne Harris' Chocolat and The Lollipop ShoesBasneen Hudha AshrafNo ratings yet
- Integrar 430 AutopilotDocument4 pagesIntegrar 430 Autopilotnelson vasquezNo ratings yet
- Soal Smart Comp Latihan2Document5 pagesSoal Smart Comp Latihan2Rafil FriasmarNo ratings yet
- Leviton 49253-Xxx 4925C-XxM Five-Ring Horizontal Cable ManagerDocument2 pagesLeviton 49253-Xxx 4925C-XxM Five-Ring Horizontal Cable ManagerJosé Luis RobalinoNo ratings yet
- Control 4Document17 pagesControl 4muhamed mahmoodNo ratings yet
- Why Does Belt Tension Matter?: Why It Matters and How It Affects Belt LifeDocument2 pagesWhy Does Belt Tension Matter?: Why It Matters and How It Affects Belt LifeMinh AnhNo ratings yet
- R and RC Firing CircuitsDocument3 pagesR and RC Firing CircuitsDeepa Mary Sobha70% (10)
- GMP Slide Kuliah 2019 - Rev 1Document77 pagesGMP Slide Kuliah 2019 - Rev 1Asta HidayatNo ratings yet
- Nitriding & Nitrocarburising: Mikael Fällström Bodycote AGI NEEDocument51 pagesNitriding & Nitrocarburising: Mikael Fällström Bodycote AGI NEEPushparaj Vignesh100% (1)
- Quiz 2 PDFDocument7 pagesQuiz 2 PDFRuth Montebon0% (1)
- Inert Gas SystemDocument69 pagesInert Gas SystemKishore Gopal89% (9)
- Engineer'S Manual: SeriesDocument126 pagesEngineer'S Manual: SeriesAnonymous hMyP30F6mNo ratings yet
- Sk75ur-2 Cab Interference Prevention SystemDocument17 pagesSk75ur-2 Cab Interference Prevention Systemmichele lugaresiNo ratings yet
- Guide To Slide in Bridge ConstructionDocument168 pagesGuide To Slide in Bridge ConstructionpassingtimeNo ratings yet
- GeneralPhysics1 - Q2 - Mod2Lesson1Newton's Law of Universal Gravitation, Gravitational Field, and Gravitational Potential EnergyDocument28 pagesGeneralPhysics1 - Q2 - Mod2Lesson1Newton's Law of Universal Gravitation, Gravitational Field, and Gravitational Potential EnergyJose GulitiwNo ratings yet
- Inflation AccountingDocument9 pagesInflation AccountingyasheshgaglaniNo ratings yet