Download as docx, pdf, or txt
You might also like
- Ati RN Medsurg 2023 With NGN (100 Questions) Word For WordDocument23 pagesAti RN Medsurg 2023 With NGN (100 Questions) Word For WordNelson MandelaNo ratings yet
- Accelerated ART Intro & Research Base Kip PPT 7-19-2017Document44 pagesAccelerated ART Intro & Research Base Kip PPT 7-19-2017scmesser0% (1)
- Myositis Core Set Measures of Activity Including The Mmt8 and Preliminary Definitions of Improvement 508Document25 pagesMyositis Core Set Measures of Activity Including The Mmt8 and Preliminary Definitions of Improvement 508Anonymous b2k9ABe7eNo ratings yet
- Disease Activity Scoring in RheumatologyDocument28 pagesDisease Activity Scoring in RheumatologyLeo FluxNo ratings yet
- Modified AshworthDocument3 pagesModified Ashworthlft.mayradiazNo ratings yet
- Raso FAST Outcomes INS 2024 E-PosterDocument1 pageRaso FAST Outcomes INS 2024 E-Postermarco.mercieriNo ratings yet
- Activities-Specific Balance Confidence (Abc) ScaleDocument16 pagesActivities-Specific Balance Confidence (Abc) ScaleMochammad Syarif HidayatNo ratings yet
- English-Patient-Rated Tennis Elbow Evaluation-User-Manual June-2010 0Document24 pagesEnglish-Patient-Rated Tennis Elbow Evaluation-User-Manual June-2010 0chandni saxenaNo ratings yet
- What Level of Symptoms Are Patients With Adult Spinal Deformity Prepared To Live With? A Cross Sectional Analysis of The 12 Month Follow Up Data From 1043 PatientsDocument13 pagesWhat Level of Symptoms Are Patients With Adult Spinal Deformity Prepared To Live With? A Cross Sectional Analysis of The 12 Month Follow Up Data From 1043 PatientscsdNo ratings yet
- 194-Article Text-295-1-10-20191216Document6 pages194-Article Text-295-1-10-20191216Helda Aida PermataNo ratings yet
- Moseley Trial: Clinical QuestionDocument5 pagesMoseley Trial: Clinical QuestionDaríoSantiagoVinuezaNo ratings yet
- 2016 - Submaximal Exercise Intensity Modulates Acute Post-Exercise Heart Rate VariabilityDocument10 pages2016 - Submaximal Exercise Intensity Modulates Acute Post-Exercise Heart Rate VariabilityVeronica JanethNo ratings yet
- Clinician-Summary-v 5 0 - FIMDocument3 pagesClinician-Summary-v 5 0 - FIMArivuNo ratings yet
- Assessment Instruments That Examine HealthDocument10 pagesAssessment Instruments That Examine HealthJoRed357No ratings yet
- S158 Proceedings of The 22nd World Meeting of The ISSM: J Sex Med 2022 00:S152 S181Document2 pagesS158 Proceedings of The 22nd World Meeting of The ISSM: J Sex Med 2022 00:S152 S181dr.enzofaversaniNo ratings yet
- Sense of Effort Is Distorted in People With CLBPDocument6 pagesSense of Effort Is Distorted in People With CLBPAntonio MartinezNo ratings yet
- Ankylosing Spondylitis Disease Activity ScoreDocument2 pagesAnkylosing Spondylitis Disease Activity ScoreDebarshi DasNo ratings yet
- Selective Serotonin Reuptake Inhibitor Combined With Dengzhanshengmai Capsule Improves The Fatigue Symptoms - A 12-Week Open-Label Pilot StudyDocument7 pagesSelective Serotonin Reuptake Inhibitor Combined With Dengzhanshengmai Capsule Improves The Fatigue Symptoms - A 12-Week Open-Label Pilot StudyleonieNo ratings yet
- 2 - PDFsam - EurJGeriatricGerontol 2 13 enDocument1 page2 - PDFsam - EurJGeriatricGerontol 2 13 enSuck my PenisNo ratings yet
- FPIN's Help Desk Answers FPIN's Help Desk Answers: Stretching For Prevention of Exercise-Related InjuryDocument1 pageFPIN's Help Desk Answers FPIN's Help Desk Answers: Stretching For Prevention of Exercise-Related InjuryRamón PérezNo ratings yet
- 6 RMD Bssq-DeformityDocument7 pages6 RMD Bssq-Deformityapi-438638588No ratings yet
- The Patient-Rated Elbow Evaluation (PREE) © User Manual: January 2007Document23 pagesThe Patient-Rated Elbow Evaluation (PREE) © User Manual: January 2007tobias septianNo ratings yet
- 3 Principles of Assessment F10-1Document7 pages3 Principles of Assessment F10-1RonNo ratings yet
- Assessment of Acute Stress DisorderDocument13 pagesAssessment of Acute Stress Disordersupport6486100% (1)
- Modi Fied Ashworth Scale and Spasm Frequency Score in Spinal Cord Injury: Reliability and CorrelationDocument7 pagesModi Fied Ashworth Scale and Spasm Frequency Score in Spinal Cord Injury: Reliability and CorrelationPrasasti 19No ratings yet
- THERAPY STUDY: Are The Results of The Trial Valid? (Internal Validity)Document4 pagesTHERAPY STUDY: Are The Results of The Trial Valid? (Internal Validity)Fatimah AlzahraNo ratings yet
- Kunal 30-10-19Document16 pagesKunal 30-10-19HrishikeshNo ratings yet
- Trauma Scoring Systems: Glasgow Coma Score (GCS)Document2 pagesTrauma Scoring Systems: Glasgow Coma Score (GCS)WigunaNo ratings yet
- Management of Lower Extremity Tendinopathy: Samuel SpinelliDocument33 pagesManagement of Lower Extremity Tendinopathy: Samuel SpinelliFrancisco Javier Luza RamosNo ratings yet
- Peripheral Muscle Training With Resistance ExercisDocument8 pagesPeripheral Muscle Training With Resistance ExercisarwitarahayuNo ratings yet
- A59.2.full PosDocument1 pageA59.2.full PosMaharani Adrianto NNo ratings yet
- Final ManuscriptDocument17 pagesFinal ManuscriptSandesh GautamNo ratings yet
- Temporal Pattern of The Repeated Bout Effect of Eccentric Exercise On Delayed-Onset Muscle SorenessDocument5 pagesTemporal Pattern of The Repeated Bout Effect of Eccentric Exercise On Delayed-Onset Muscle SorenessRicardo Pereira NevesNo ratings yet
- Lanjutan StrengteningDocument5 pagesLanjutan Strengtening'fanny Quenhita'No ratings yet
- Teicher ScoreDocument5 pagesTeicher ScoreDarleyEduardoGalarzaCedeñoNo ratings yet
- Modified Trauma ScoringDocument63 pagesModified Trauma ScoringparuNo ratings yet
- Research Article On Sri Vishnu SahasranamamDocument3 pagesResearch Article On Sri Vishnu Sahasranamamgorli vasuNo ratings yet
- The Functional Movement Screen: A Reliability Study: ResearchDocument11 pagesThe Functional Movement Screen: A Reliability Study: ResearchLeonardiniNo ratings yet
- Id 24368Document53 pagesId 24368Miroslav FilistovičNo ratings yet
- Mindfulness-Based Cognitive Therapy For TheDocument19 pagesMindfulness-Based Cognitive Therapy For ThejuliaCasariegoNo ratings yet
- Programme 1615Document29 pagesProgramme 1615Matias RizzoneNo ratings yet
- Assessing The Need For Adenotonsillectomy For Sleep-Disordered Breathing - Aris Rahmanda - PrintOutDocument8 pagesAssessing The Need For Adenotonsillectomy For Sleep-Disordered Breathing - Aris Rahmanda - PrintOutMahrezNo ratings yet
- Amandersson, 1541Document6 pagesAmandersson, 1541sayed imadNo ratings yet
- Apply Journal For ICIPADocument7 pagesApply Journal For ICIPADekdwi KapakNo ratings yet
- Penn Spasm Frequency Scale (PSFS)Document3 pagesPenn Spasm Frequency Scale (PSFS)fi.afifah NurNo ratings yet
- FNP Articulo 1Document3 pagesFNP Articulo 1marleni lucila arista mollaNo ratings yet
- CJP May 06 Muller BC1Document6 pagesCJP May 06 Muller BC1haddig8No ratings yet
- Ji-Hua Xu 2018Document3 pagesJi-Hua Xu 2018Mary FallNo ratings yet
- Prehospital Stroke Assessment Tools and BenefitsDocument55 pagesPrehospital Stroke Assessment Tools and BenefitsDennis soelionganNo ratings yet
- Endoscopy - and - Colonoscopy - in - Patients - With AAADocument2 pagesEndoscopy - and - Colonoscopy - in - Patients - With AAAfahmyhhablassNo ratings yet
- Seiler Haugen Kuffel 2007Document8 pagesSeiler Haugen Kuffel 2007luisgarcialcg23No ratings yet
- Atividade - Aula 5 (20/04/2022) - Validade de Construto - Teste de HipótesesDocument4 pagesAtividade - Aula 5 (20/04/2022) - Validade de Construto - Teste de HipótesesROSANo ratings yet
- Amiaz 2021 Responses To Balance Challenges in Persons With Panic Disorder A Pilot Study ofDocument12 pagesAmiaz 2021 Responses To Balance Challenges in Persons With Panic Disorder A Pilot Study ofJuan Hernández GarcíaNo ratings yet
- Effect of Seamless Nursing For Complications On Cataract PatientsDocument3 pagesEffect of Seamless Nursing For Complications On Cataract Patientsnila choirun nailiNo ratings yet
- Relation Between BEST Test & Biodex in StrokeDocument7 pagesRelation Between BEST Test & Biodex in StrokeBassam EsmailNo ratings yet
- Bmj.l5101.full Stroke PDFDocument15 pagesBmj.l5101.full Stroke PDFMr. LNo ratings yet
- Wheelchair Skills Test (WST) : Assessment OverviewDocument3 pagesWheelchair Skills Test (WST) : Assessment OverviewAndré LuizNo ratings yet
- 2.1.1 Metaanalisis Volumen2d PDFDocument17 pages2.1.1 Metaanalisis Volumen2d PDFMari PaoNo ratings yet
- 6 Minute Walk TestDocument7 pages6 Minute Walk Testriccardo6grassiNo ratings yet
- Neuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodFrom EverandNeuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodNo ratings yet
- Principles and Practice of Systematic Reviews and Meta-AnalysisFrom EverandPrinciples and Practice of Systematic Reviews and Meta-AnalysisNo ratings yet
- Acth Stimulation Testing Protocol CanineDocument2 pagesActh Stimulation Testing Protocol CanineSpital Veterinar AndivetNo ratings yet
- CI-01 - Cancer (Kanser)Document2 pagesCI-01 - Cancer (Kanser)jijiqNo ratings yet
- Path Pancreas McqsDocument4 pagesPath Pancreas McqsUu UuNo ratings yet
- SHC SMUG RibavirinDocument2 pagesSHC SMUG RibavirinMario BulaciosNo ratings yet
- NCM 118 - Lesson 4 (ARDS)Document4 pagesNCM 118 - Lesson 4 (ARDS)Bobby Christian DuronNo ratings yet
- Mapeh BrochureDocument1 pageMapeh BrochureRio PerezNo ratings yet
- 7 DkaDocument28 pages7 DkaFuad Aman AbjNo ratings yet
- COVID19 Flu A&b Ag Combo Rapid Test SELL SHEET OG (1) - CompressedDocument3 pagesCOVID19 Flu A&b Ag Combo Rapid Test SELL SHEET OG (1) - CompressedmlgraziosiNo ratings yet
- Prevention of Substance AbuseDocument5 pagesPrevention of Substance AbuseIsha BhusalNo ratings yet
- EM Calculator Report 137138Document2 pagesEM Calculator Report 137138chaitanya varmaNo ratings yet
- Pediatrics Rapid RevisionDocument72 pagesPediatrics Rapid RevisionWorld MedclickzNo ratings yet
- Lesson 5. Health and NutritionDocument5 pagesLesson 5. Health and NutritionLoveyysolonNo ratings yet
- Annexure 7: Medical Certificate (To Be Issued by A Registered Medical Practitioner) General ExpectationsDocument1 pageAnnexure 7: Medical Certificate (To Be Issued by A Registered Medical Practitioner) General ExpectationsLikithkrishnasai KommareddyNo ratings yet
- FINAL AED Purple Nutrition Book RemovedDocument28 pagesFINAL AED Purple Nutrition Book RemovedOla Conde VIINo ratings yet
- Exam 231Document8 pagesExam 231Wondimu KoyNo ratings yet
- Practice 4Document11 pagesPractice 4Justine Rs Dela TorreNo ratings yet
- 09-02-A Skills Lab Rheuma Monoarthritis DDDocument28 pages09-02-A Skills Lab Rheuma Monoarthritis DDShrouk EldakroryNo ratings yet
- J Care Application Form (New)Document8 pagesJ Care Application Form (New)Chazzy f ChazzyNo ratings yet
- 4 Immunizations1Document37 pages4 Immunizations1خالد المعلميNo ratings yet
- Síndrome Del Intestino Irritable (Caso 1.9)Document10 pagesSíndrome Del Intestino Irritable (Caso 1.9)xixiNo ratings yet
- Test Bank For Drug Use and Abuse 8th EditionDocument25 pagesTest Bank For Drug Use and Abuse 8th EditionGloria Moore100% (30)
- Smith 2021Document4 pagesSmith 2021Sergio Alberto Sulub NavarreteNo ratings yet
- Abdomen Macleod - S - Clinical - Examination - 15thDocument28 pagesAbdomen Macleod - S - Clinical - Examination - 15thwxyngtc4n9No ratings yet
- Review QuestionsDocument8 pagesReview QuestionsRose May OrtegaNo ratings yet
- Colin Pinneo - Research PaperDocument8 pagesColin Pinneo - Research Paperapi-646159875No ratings yet
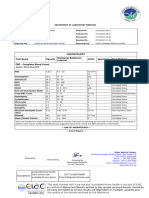
- Lab Report 11528716 20230127122957Document7 pagesLab Report 11528716 20230127122957Ajay KumarNo ratings yet
- Nama-Nama DiagnosaDocument1 pageNama-Nama Diagnosapuskesmas tulungrejoNo ratings yet
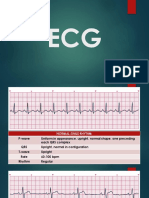
- Ecg HandoutDocument24 pagesEcg HandoutLeah DeeNo ratings yet
- Summary Hivaids SetDocument747 pagesSummary Hivaids Setv8qwxqb2shNo ratings yet