Download as pdf or txt
You might also like
- NAPLEX Cheat SheetDocument4 pagesNAPLEX Cheat SheetWil Lester67% (6)
- CEPE Printable BDSM ChecklistDocument17 pagesCEPE Printable BDSM Checklistdeseusnow4980100% (1)
- Business Plan CircularCarbon 01.08.Document42 pagesBusiness Plan CircularCarbon 01.08.lepezNo ratings yet
- Top 300 Drugs Pocket Reference Guide (2021 Edition)From EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Rating: 5 out of 5 stars5/5 (1)
- MIMS Summary Table-G6PDDocument1 pageMIMS Summary Table-G6PDenchanteresse100% (3)
- Cancer Foye's Principles of Medicinal Chemistry-1219-1286Document68 pagesCancer Foye's Principles of Medicinal Chemistry-1219-1286minhxuan100% (3)
- ACB Scale - Legal Size PDFDocument2 pagesACB Scale - Legal Size PDFMarina Swanson0% (1)
- Drugs Acting On Body SystemsDocument3 pagesDrugs Acting On Body SystemsKim AlexisNo ratings yet
- Anti Cancer DrugsDocument3 pagesAnti Cancer DrugsDheaNo ratings yet
- PCS Controlled Drugs ListDocument1 pagePCS Controlled Drugs ListRosa ValenteNo ratings yet
- Classification of The DrugsDocument50 pagesClassification of The DrugsGlena SalamNo ratings yet
- Directly Acting ExpectorantsDocument6 pagesDirectly Acting ExpectorantsRoma Ann ManahanNo ratings yet
- Peripheral Nervous System (PNS) Central Nervous System (CNS) Efferent Division Afferent DivisionDocument31 pagesPeripheral Nervous System (PNS) Central Nervous System (CNS) Efferent Division Afferent Divisionapi-19916399No ratings yet
- CNS Drugs (May 21)Document95 pagesCNS Drugs (May 21)Angela Marie JoseNo ratings yet
- 1.beta Blockers: List of Different Groups of MedicationsDocument18 pages1.beta Blockers: List of Different Groups of MedicationsJayshree ParmarNo ratings yet
- Tier Zero ListDocument1 pageTier Zero ListJorgeNo ratings yet
- Anti-Cholinergic Drugs: DR Naser Ashraf TadviDocument23 pagesAnti-Cholinergic Drugs: DR Naser Ashraf TadviVivek PandeyNo ratings yet
- Prednisolone Drug Lnteraction ListDocument4 pagesPrednisolone Drug Lnteraction Listmohammed almaaziNo ratings yet
- Hand Book of Agro Chemical Industries (Insecticides & Pesticides)Document23 pagesHand Book of Agro Chemical Industries (Insecticides & Pesticides)Deepak BhanjiNo ratings yet
- Opioids by MDocument24 pagesOpioids by Mwww.munnamichel20No ratings yet
- Chapter - 2 Source of DrugsDocument22 pagesChapter - 2 Source of DrugsahmadNo ratings yet
- Anticholinergics Study Drug ListDocument1 pageAnticholinergics Study Drug ListDrima Edi100% (1)
- Pharmacology Module-7Document6 pagesPharmacology Module-7maurizemedija15No ratings yet
- Pharmacology Important QuestionsDocument19 pagesPharmacology Important Questionseveryday211998No ratings yet
- Drug ListDocument18 pagesDrug ListKara MissGiggles BakerNo ratings yet
- Analgetics OpiodDocument30 pagesAnalgetics OpiodDiany LiemNo ratings yet
- Cancer Drugs Pharmacology TableDocument11 pagesCancer Drugs Pharmacology TableAmin InanNo ratings yet
- KU PPB 423 Lesson 2 - Introduction To Antineoplastic AgentsDocument9 pagesKU PPB 423 Lesson 2 - Introduction To Antineoplastic AgentsPharmswipe KenyaNo ratings yet
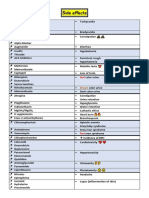
- Side EffectsDocument2 pagesSide EffectsFahad AlkenaniNo ratings yet
- Side Effects: BrownDocument2 pagesSide Effects: BrownAfsal Ur FriendNo ratings yet
- Drugs For Cancer TherapyDocument102 pagesDrugs For Cancer TherapyPUTRI CHRISTIANTI TELAUMBANUA 1No ratings yet
- List of Anti-Cancer Drugs 15 Nov 2016 FinalDocument3 pagesList of Anti-Cancer Drugs 15 Nov 2016 FinallalsinghsanasamNo ratings yet
- Pharmacology: Andrea Q. Carigma, R.PH., M.D. February 2015Document63 pagesPharmacology: Andrea Q. Carigma, R.PH., M.D. February 2015Leonibel GhloeNo ratings yet
- 2 Pharmacology of ChemotherapeuticsDocument34 pages2 Pharmacology of ChemotherapeuticsTilaye GebruNo ratings yet
- سندDocument10 pagesسندAshkan AbbasiNo ratings yet
- Pesticide PoisoningDocument34 pagesPesticide PoisoningappealingashishNo ratings yet
- Photosensitising Agents: PhotosensitisationDocument26 pagesPhotosensitising Agents: PhotosensitisationMagesh SNo ratings yet
- Pesticide PoisoningDocument34 pagesPesticide PoisoningpreethiNo ratings yet
- 4,5,6) Parasympatholytic DrugsDocument52 pages4,5,6) Parasympatholytic Drugsmoranggames2No ratings yet
- AlkaloidsDocument8 pagesAlkaloidsKristina NizabelaNo ratings yet
- Antiprotozoal and AntihelminticDocument36 pagesAntiprotozoal and AntihelminticDiriba feyisaNo ratings yet
- Pyrazole DerivativesDocument8 pagesPyrazole DerivativesReysmaNo ratings yet
- 03 Sulphonamides 2Document25 pages03 Sulphonamides 2Abeer SarayraNo ratings yet
- Anti Cancer ChemotherapyDocument103 pagesAnti Cancer ChemotherapyMourian AmanNo ratings yet
- Compounds of TyrosineDocument27 pagesCompounds of TyrosineMahi AgrawalNo ratings yet
- Brand Name of DrugsDocument37 pagesBrand Name of Drugsgaurang mediaNo ratings yet
- Drugs in LactationDocument36 pagesDrugs in Lactationcorzpun168678100% (1)
- G6PDDocument2 pagesG6PDHaramrit SinghNo ratings yet
- Toxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiDocument40 pagesToxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiTan Geok EngNo ratings yet
- Lecture 4Document12 pagesLecture 4kaleem ullahNo ratings yet
- Drug ListDocument3 pagesDrug ListluciNo ratings yet
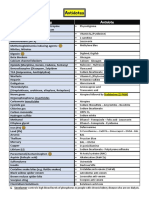
- AntidotesDocument1 pageAntidotesFahad AlkenaniNo ratings yet
- Antidotes: Poison/Drug AntidoteDocument1 pageAntidotes: Poison/Drug AntidoteAfsal Ur FriendNo ratings yet
- Revision Guide Made Simple For Pharmacy Technicians 3rd Edition: 3rd EditionFrom EverandRevision Guide Made Simple For Pharmacy Technicians 3rd Edition: 3rd EditionNo ratings yet
- Revision Guide Made Simple For Pharmacy Technicians - PTCB: 4th EditionFrom EverandRevision Guide Made Simple For Pharmacy Technicians - PTCB: 4th EditionNo ratings yet
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- 2022 Larimer County General Election Sample BallotDocument4 pages2022 Larimer County General Election Sample BallotColoradoanNo ratings yet
- The Environment (Protection) Act, 1986Document38 pagesThe Environment (Protection) Act, 1986Anugya JhaNo ratings yet
- Defensive - Driving TrainingDocument43 pagesDefensive - Driving Trainingmuhammad.younisNo ratings yet
- UR AirlinesDocument2 pagesUR Airlinesmusts jokerrNo ratings yet
- Notice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Document2 pagesNotice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Justia.comNo ratings yet
- Fireye Flame Scanner UV1A6 (Sc-102 PDFDocument8 pagesFireye Flame Scanner UV1A6 (Sc-102 PDFld_ganeshNo ratings yet
- Itp - For Heat ExchangerDocument3 pagesItp - For Heat ExchangerSuraj ShettyNo ratings yet
- SDS FileDocument7 pagesSDS FilemrkhuderNo ratings yet
- Parle AgroDocument3 pagesParle AgroKumar GautamNo ratings yet
- Abu Dhabi Guid To Water Supply RegulationsDocument72 pagesAbu Dhabi Guid To Water Supply RegulationsAdlan100% (8)
- How To Grow A Truly Great BeardDocument3 pagesHow To Grow A Truly Great BeardWALEED HASSANNo ratings yet
- Hvled New High Power Factor PSR LED Drivers: Hvled807Pf Hvled815PfDocument22 pagesHvled New High Power Factor PSR LED Drivers: Hvled807Pf Hvled815PfMARCoONo ratings yet
- S&P Debt Rating DefinitionsDocument6 pagesS&P Debt Rating DefinitionsilyakostNo ratings yet
- Meet The Parents Part 1Document3 pagesMeet The Parents Part 1Anna Rumyantzeva0% (1)
- Anorexia Nervosa: Eating DisorderDocument21 pagesAnorexia Nervosa: Eating DisorderFrances Oscar GaviolaNo ratings yet
- Ob13 Tif07Document20 pagesOb13 Tif07Lamis Alahmadi100% (1)
- Canoeing: Araracap, Cachuela, Huerto, Nueva Arcena, Asahan, Loyola, SeguiroDocument34 pagesCanoeing: Araracap, Cachuela, Huerto, Nueva Arcena, Asahan, Loyola, SeguiroGreth NuevaNo ratings yet
- InventoriesDocument1 pageInventoriesLet it beNo ratings yet
- Permitted Services (27 Sep)Document5 pagesPermitted Services (27 Sep)maweijiaNo ratings yet
- Ritu CharyaDocument1 pageRitu Charyayuvi087No ratings yet
- Critical SkillsDocument5 pagesCritical SkillsJosiah MwashitaNo ratings yet
- GEAR BOX Service ManualDocument66 pagesGEAR BOX Service ManualJon Mo86% (7)
- Autism Spectrum and Open-MindednessDocument2 pagesAutism Spectrum and Open-MindednessJaime MontoyaNo ratings yet
- Icasi 2018 Sonproceedingve Ozet KitabcigiDocument726 pagesIcasi 2018 Sonproceedingve Ozet KitabcigiIlo Ruiz100% (1)
- Updated DXN Presentation1Document56 pagesUpdated DXN Presentation1xs2vicky100% (1)
- Evidencia Científica Sobre La FlexibilidadDocument28 pagesEvidencia Científica Sobre La Flexibilidadsulei222No ratings yet
- Corrguard Si PDFDocument18 pagesCorrguard Si PDFyolia16100% (1)
- Welcome Madison 2013 2014Document97 pagesWelcome Madison 2013 2014Alexander León PuelloNo ratings yet






















































![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-2-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)