Download as pdf or txt
You might also like
- TNCC Study GuideDocument4 pagesTNCC Study Guidescroasdell83% (6)
- Interactive Code Blue Evaluation FormDocument2 pagesInteractive Code Blue Evaluation FormAyman Ali100% (1)
- ITLS 8e Advanced Pre-Test - Annotated Key PDFDocument10 pagesITLS 8e Advanced Pre-Test - Annotated Key PDFJohn E. Ibrahim100% (1)
- BLSDocument39 pagesBLSShua QuezNo ratings yet
- Airway ManagementDocument42 pagesAirway ManagementKugan KishurNo ratings yet
- Airway - MX DsdsDocument47 pagesAirway - MX DsdsFirdaus BaharuddinNo ratings yet
- Emergency Airway Management: Pat Melanson, MDDocument47 pagesEmergency Airway Management: Pat Melanson, MDFarida IntanNo ratings yet
- Airway MXDocument47 pagesAirway MXansuh22No ratings yet
- Airway Management:: An Introduction and Overview & Massive HemoptysisDocument69 pagesAirway Management:: An Introduction and Overview & Massive Hemoptysiskamel6No ratings yet
- Anesthesia For Maxillofacial ProcedureDocument90 pagesAnesthesia For Maxillofacial ProcedureAnirban Roy100% (1)
- Airway Emergency ManagementDocument47 pagesAirway Emergency ManagementTerefe AlemayehuNo ratings yet
- Airway Management-Dr RistiawanDocument75 pagesAirway Management-Dr RistiawanjavajavuNo ratings yet
- General Anesthesia: IntubationDocument44 pagesGeneral Anesthesia: IntubationMiezu CosminNo ratings yet
- AirwayDocument31 pagesAirwayAlessandro AlfieriNo ratings yet
- Function of The Resp. System: RespirationDocument75 pagesFunction of The Resp. System: RespirationTara Bartorillo SanseverinoNo ratings yet
- Manajemen AirwayDocument91 pagesManajemen AirwayAnonymous niVHtxvPNo ratings yet
- Tatalaksana Jalan NafasDocument49 pagesTatalaksana Jalan NafasSyaiful RochimNo ratings yet
- Airway Managmenat Normal and DifficultDocument49 pagesAirway Managmenat Normal and DifficultHari Om ChaurasiyaNo ratings yet
- Advanced Airway Care: Intensive Care Unit PerspectiveDocument42 pagesAdvanced Airway Care: Intensive Care Unit PerspectiveJeffery Samuel100% (1)
- Brachycephalic SyndromeDocument73 pagesBrachycephalic SyndromevetmedcoyoacanNo ratings yet
- Airwaymanagement 090810125917 Phpapp02Document41 pagesAirwaymanagement 090810125917 Phpapp02AzanReza AbdullehNo ratings yet
- En Pediatric AirwayDocument48 pagesEn Pediatric AirwayRovz J. OkIeNo ratings yet
- Airway Management - IntubationDocument31 pagesAirway Management - IntubationRajaNo ratings yet
- Artificial AirwaysDocument17 pagesArtificial AirwaysSri DarmayantiNo ratings yet
- IntubationDocument34 pagesIntubationFlighterdocNo ratings yet
- Principles of Airway Management.Document68 pagesPrinciples of Airway Management.Shimmering MoonNo ratings yet
- Airway 2010Document69 pagesAirway 2010abdullahNo ratings yet
- Airway TraumaDocument73 pagesAirway TraumaSarah BirechNo ratings yet
- EducationStds AirwayManagementDocument18 pagesEducationStds AirwayManagementZosmasNo ratings yet
- Respiratory Conditions: Nineveh Danielle M. Guioguio, RNDocument63 pagesRespiratory Conditions: Nineveh Danielle M. Guioguio, RNnguioguioNo ratings yet
- Foreign Body Aspiration.Document40 pagesForeign Body Aspiration.dr.hungsonNo ratings yet
- Assessment and Management ofDocument123 pagesAssessment and Management ofshekinahNo ratings yet
- Airway ManagementDocument57 pagesAirway ManagementAndrew JoshuaNo ratings yet
- ACLS Algorithms 2020 (Advanced Cardiac Life Support)Document1 pageACLS Algorithms 2020 (Advanced Cardiac Life Support)evelyn k100% (2)
- Advanced AirwayDocument34 pagesAdvanced Airwayvica_christiaNo ratings yet
- Basic Life SupportDocument101 pagesBasic Life SupportMasyfuk Zuhdi JamhurNo ratings yet
- Endotracheal IntubationDocument43 pagesEndotracheal IntubationBishow100% (2)
- Difficult Airway Management: By: Bereket Habtamu Advisor: Leulayehu AkaluDocument72 pagesDifficult Airway Management: By: Bereket Habtamu Advisor: Leulayehu AkaluagatakassaNo ratings yet
- Perioperatif Anestesi Oral-MaksilofasialDocument73 pagesPerioperatif Anestesi Oral-MaksilofasialWicakKuntoWibowoNo ratings yet
- Gagal Nafas & Kedaduratan Sis - RespDocument53 pagesGagal Nafas & Kedaduratan Sis - Respthe_jokosNo ratings yet
- Tracheostomy Emergencies and ManagementDocument30 pagesTracheostomy Emergencies and ManagementCharles S. Williams RRT, AE-C100% (2)
- Airway Management: Azzam Nawab Mbbs Aanawab@imamu - Edu.saDocument48 pagesAirway Management: Azzam Nawab Mbbs Aanawab@imamu - Edu.sasamhNo ratings yet
- Airway 2Document36 pagesAirway 2Daniel Dwi NugrohoNo ratings yet
- 9 AirwaymanagementDocument31 pages9 Airwaymanagementsara.sms1No ratings yet
- EMT Basic Advanced Airway Management: Pharyngeal Esophageal Airway Device (PEAD) A.K.A. CombitubeDocument86 pagesEMT Basic Advanced Airway Management: Pharyngeal Esophageal Airway Device (PEAD) A.K.A. CombitubeparamitamdNo ratings yet
- Gels I AbDocument65 pagesGels I AbFatahillah NazarNo ratings yet
- Respiratory PresentationDocument137 pagesRespiratory Presentationakoeljames8543No ratings yet
- Foreign Body Aspiration 21Document40 pagesForeign Body Aspiration 21Rinaldi Sani NasutionNo ratings yet
- Difficult AirwayDocument38 pagesDifficult AirwaybrojeemNo ratings yet
- Ett Introduction Edrm 23-24Document52 pagesEtt Introduction Edrm 23-24MahdiyyahNo ratings yet
- Airway ManagmentDocument37 pagesAirway Managmenthashmilaiba847No ratings yet
- Rapid Sequence Intubation ReportDocument55 pagesRapid Sequence Intubation Reportlorkan19100% (1)
- Co Vi Acls - 0Document18 pagesCo Vi Acls - 0Amer ShihadeNo ratings yet
- Respiratory Emergencies Fall06picDocument41 pagesRespiratory Emergencies Fall06pickiruthikasettu46No ratings yet
- Airway ManagementDocument83 pagesAirway ManagementBerliany L Ganie FhatwaNo ratings yet
- Adult NasalDocument14 pagesAdult NasalillirpohnimNo ratings yet
- The Neonatal Airway and Neonatal IntubationDocument32 pagesThe Neonatal Airway and Neonatal IntubationSubas SharmaNo ratings yet
- Airway / Breathing ProtocolsDocument15 pagesAirway / Breathing ProtocolsSbarcea AurelNo ratings yet
- Trauma Resuscitation Acute Care Emerg MedDocument67 pagesTrauma Resuscitation Acute Care Emerg MedsyasyaNo ratings yet
- LECTURE4-Airway Management and Equipment-Dr ManaaDocument68 pagesLECTURE4-Airway Management and Equipment-Dr ManaasnezaimNo ratings yet
- Oakes ACCSDocument167 pagesOakes ACCSKramer ChangNo ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- Check List AmbulanceDocument2 pagesCheck List AmbulanceIrma Giopani PratiwiNo ratings yet
- Pediatric BLSDocument32 pagesPediatric BLSYuni AjahNo ratings yet
- Metode Cardio Pulmonary Resuscitation Untuk Meningkatkan: Survival Rates Pasien Post Cardiac ArrestDocument5 pagesMetode Cardio Pulmonary Resuscitation Untuk Meningkatkan: Survival Rates Pasien Post Cardiac ArrestYesiNo ratings yet
- What Are The Ten New Commandments in Severe Polytrauma Management 1Document8 pagesWhat Are The Ten New Commandments in Severe Polytrauma Management 1antonio dengNo ratings yet
- Review of Medical Physiology 21 EditionDocument4 pagesReview of Medical Physiology 21 EditionMaine Asuncion0% (1)
- Transport of The Critically Ill Patient PDFDocument4 pagesTransport of The Critically Ill Patient PDFaksinuNo ratings yet
- 6504 EapDocument4 pages6504 Eapapi-233075365No ratings yet
- Pit Crew EnglishDocument61 pagesPit Crew EnglishDAVID CARVAJALNo ratings yet
- Module 5 Session 2 TreatmentDocument13 pagesModule 5 Session 2 TreatmentFlorence Danielle DimenNo ratings yet
- Primary Trauma CareDocument48 pagesPrimary Trauma CareKABERA RENENo ratings yet
- Basic Life SupportDocument29 pagesBasic Life SupportRyan-Jay Abolencia100% (3)
- Tiki Taka CK SurgeryDocument50 pagesTiki Taka CK SurgeryEmad MerganNo ratings yet
- Dr. Sagar Shah: Dept of Accident & Emergency Kokilaben Dhirubhai Ambani Hospital and Medical Research InstituteDocument21 pagesDr. Sagar Shah: Dept of Accident & Emergency Kokilaben Dhirubhai Ambani Hospital and Medical Research InstituteSagar ShahNo ratings yet
- Bleeding Control Basic Instructor Presentation NotesDocument62 pagesBleeding Control Basic Instructor Presentation NotesohmyscribderNo ratings yet
- Bls (BHD) : Dr. Rusdian Nurmadi, Mked (An), SpanDocument74 pagesBls (BHD) : Dr. Rusdian Nurmadi, Mked (An), SpanDedi Iskandar4549No ratings yet
- Musculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Document32 pagesMusculosceletal Block: Prof - Dr.Dr. Bambang Pardjianto, SPB., Spbp-Re (K)Irsyad Robani WNo ratings yet
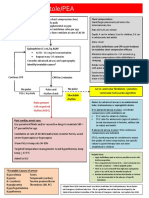
- Asystole/PEA: Epinephrine 0.1 ML/KG ASAPDocument1 pageAsystole/PEA: Epinephrine 0.1 ML/KG ASAPAlejandro MusaNo ratings yet
- Katie Adult Day Center Policies and Procedures Manual 05-036.16Document1 pageKatie Adult Day Center Policies and Procedures Manual 05-036.16superm0mof6No ratings yet
- Tiffany McgeeneyDocument1 pageTiffany Mcgeeneyapi-361448701No ratings yet
- Scenario - Emergency Drill 23.07.2019Document1 pageScenario - Emergency Drill 23.07.2019Ows AnishNo ratings yet
- PediatricDocument4 pagesPediatricIrma Nur Rizka HanifahNo ratings yet
- Adult Cardiac Arrest AlgoritmaDocument1 pageAdult Cardiac Arrest AlgoritmaYouniehacibie Ichisky ChildNo ratings yet
- Shock: Classification and PathophysiologyDocument15 pagesShock: Classification and PathophysiologyAishwaray KohliNo ratings yet
- Bantuan Hidup Dasar: Umum TeknikDocument12 pagesBantuan Hidup Dasar: Umum Teknikayu karimahNo ratings yet
- Dechoker Post Market Surveillance Report - Five Alleged UK Care Home Choking Rescue CasesDocument15 pagesDechoker Post Market Surveillance Report - Five Alleged UK Care Home Choking Rescue CasesACD SkepticNo ratings yet
- Blunt Abdominal Trauma Treatment & Management - Approach Considerations, Prehospital Care, Emergency Department CareDocument8 pagesBlunt Abdominal Trauma Treatment & Management - Approach Considerations, Prehospital Care, Emergency Department CareyunikayunNo ratings yet
- Complete Suite: Plan Comparison ChartDocument33 pagesComplete Suite: Plan Comparison Chartmaestrodevil5842No ratings yet