Download as pdf or txt
You might also like
- Mechanical Ventilation Made EasyDocument5 pagesMechanical Ventilation Made EasypraveenbhavniNo ratings yet
- Esophageal Varices Concept MapDocument2 pagesEsophageal Varices Concept MapSureen Regular100% (1)
- STUDENT-Sepsis - Fundamental - Reasoning Fillable-1Document5 pagesSTUDENT-Sepsis - Fundamental - Reasoning Fillable-1Laura PoultneyNo ratings yet
- Case Study 3Document5 pagesCase Study 3api-644492588100% (1)
- IPD - Kelas AC - Perdarahan Sal. Cerna - Dr. Hery Djagat - 28 Agustus 2018Document75 pagesIPD - Kelas AC - Perdarahan Sal. Cerna - Dr. Hery Djagat - 28 Agustus 2018evanoNo ratings yet
- Body Fluid Analysis Table-2017Document2 pagesBody Fluid Analysis Table-2017Afrasiab KhanNo ratings yet
- Complications of Cirrhosis: Update 2015: M.pinzani@ucl - Ac.ukDocument24 pagesComplications of Cirrhosis: Update 2015: M.pinzani@ucl - Ac.ukNovita ApramadhaNo ratings yet
- Heart Failure: Peter A. Mccullough, MD, MPH, Facc, Facp, Faha, FCCPDocument54 pagesHeart Failure: Peter A. Mccullough, MD, MPH, Facc, Facp, Faha, FCCPDenisse Tinajero SánchezNo ratings yet
- Peptic Ulcer Disease UpdatedDocument19 pagesPeptic Ulcer Disease UpdatedKiara GovenderNo ratings yet
- Approach To Lower GI BleedingDocument86 pagesApproach To Lower GI BleedingwassupporamaNo ratings yet
- SYOK - Desi Surya IniDocument40 pagesSYOK - Desi Surya IniDesi Suryani DewiNo ratings yet
- IMS All Seminars FinalDocument21 pagesIMS All Seminars Finaljwxxi11No ratings yet
- Neurology SummaryDocument57 pagesNeurology SummaryMajed AlamiNo ratings yet
- Syndrome of Inappropriate Antidiuresis From Pathophysiology To ManagementDocument43 pagesSyndrome of Inappropriate Antidiuresis From Pathophysiology To ManagementArley SuarezNo ratings yet
- SPARCtoolDocument1 pageSPARCtoolqerat88No ratings yet
- Syndrome of Inappropriate Antidiuresis: From Pathophysiology To ManagementDocument43 pagesSyndrome of Inappropriate Antidiuresis: From Pathophysiology To ManagementDanny VarjãoNo ratings yet
- Wednesday HarvardDocument61 pagesWednesday HarvardNational Press FoundationNo ratings yet
- UGI BLEED-OfficeDocument24 pagesUGI BLEED-OfficeVishal PNo ratings yet
- Congenital Valvular StenosisDocument46 pagesCongenital Valvular StenosisInsan IlmanNo ratings yet
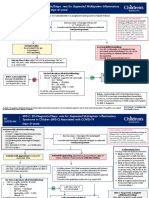
- MIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenDocument8 pagesMIS-C: Clinic-Diagnostic/Dispo Recs For Multisystem Inflammatory Syndrome in ChildrenJosselle Sempio CalientaNo ratings yet
- AK Tripathi, Kamal Sawlani - Essentials of Medicine For Dental Students - 2nd Edition - WWW - Thedentalhub.org - inDocument302 pagesAK Tripathi, Kamal Sawlani - Essentials of Medicine For Dental Students - 2nd Edition - WWW - Thedentalhub.org - inemanNo ratings yet
- 3 Abses SerebelumDocument3 pages3 Abses SerebelumseruniallisaaslimNo ratings yet
- ACC Anticoagulation For AFib in CLL Patients Interactive V05 GoldDocument22 pagesACC Anticoagulation For AFib in CLL Patients Interactive V05 GoldhibaNo ratings yet
- Vascular CatastropheDocument3 pagesVascular CatastropheJesily JoyNo ratings yet
- CCS Heart Failure Guidelines: 2014 Update On New Therapies, Biomarkers, Anemia Management, and Complex CasesDocument88 pagesCCS Heart Failure Guidelines: 2014 Update On New Therapies, Biomarkers, Anemia Management, and Complex CaseseliasNo ratings yet
- Laboratory Studies: FecalysisDocument2 pagesLaboratory Studies: FecalysisKris TejereroNo ratings yet
- Retinal Vein OcclusionDocument1 pageRetinal Vein Occlusionmart0830No ratings yet
- DR Sutarmawan Acute Presentation of Valve SletnosisDocument33 pagesDR Sutarmawan Acute Presentation of Valve SletnosisArniNo ratings yet
- Week 13 Disorders of Secondary Hemostasis LecDocument8 pagesWeek 13 Disorders of Secondary Hemostasis LecCzarina Mae IlaganNo ratings yet
- Cardiac SurgeryDocument110 pagesCardiac SurgeryChristopher McAndrew100% (1)
- OPTO 309 Other Retinal Vascular DisordersDocument5 pagesOPTO 309 Other Retinal Vascular DisorderscaponsharranerizaNo ratings yet
- Abd Distension & Ascites-1, All NewDocument34 pagesAbd Distension & Ascites-1, All NewANENA RHODANo ratings yet
- Upper Gi BleedDocument12 pagesUpper Gi BleedTaha KamranNo ratings yet
- Hemolytic Anemia's Thalassemia (REZAMAGHAMI)Document57 pagesHemolytic Anemia's Thalassemia (REZAMAGHAMI)Siavash HosseinjanzadehNo ratings yet
- Severe Aortic Stenosis and TavrDocument67 pagesSevere Aortic Stenosis and TavrnaimNo ratings yet
- AMLS Mobile Reference GuideDocument6 pagesAMLS Mobile Reference GuideLim Jun Bin100% (1)
- Aortic Stenosis BY ISRARDocument50 pagesAortic Stenosis BY ISRARAkramNo ratings yet
- Diabetic RetinopathyDocument1 pageDiabetic RetinopathyshakyaNo ratings yet
- K9. Penyakit Kardiovaskuler BawaanDocument70 pagesK9. Penyakit Kardiovaskuler Bawaanjulis muharamNo ratings yet
- Arrythmia Management in Primary CareDocument51 pagesArrythmia Management in Primary CarecelinamannaNo ratings yet
- AnemiaDocument2 pagesAnemiaRed DiggerNo ratings yet
- Handout StudentsDocument2 pagesHandout Studentsapi-588254706No ratings yet
- Epidemiology Clinical Features Diagnosis Treatment EndocarditisDocument1 pageEpidemiology Clinical Features Diagnosis Treatment EndocarditisSolomon Seth SallforsNo ratings yet
- 20.guidelines AnaemiaDocument5 pages20.guidelines AnaemiaRed DevilNo ratings yet
- Syok Hipovolemik (1) SalinanDocument34 pagesSyok Hipovolemik (1) SalinanyusufNo ratings yet
- UWORLDDocument1 pageUWORLDmerontesfaye51No ratings yet
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- Abd Distension & Ascites-2, All You NeedDocument36 pagesAbd Distension & Ascites-2, All You NeedANENA RHODANo ratings yet
- Int - med.Fet.3.EGRTACOS-Manejo Retraso Crecimiento Intrauterino.Document11 pagesInt - med.Fet.3.EGRTACOS-Manejo Retraso Crecimiento Intrauterino.zaaaidaNo ratings yet
- Abnormal FBC 1.16 Feb 2016Document5 pagesAbnormal FBC 1.16 Feb 2016jyothi vallabhaneniNo ratings yet
- Novine U Lecenju HTA Ber HemiDocument62 pagesNovine U Lecenju HTA Ber HemispalemaxNo ratings yet
- Acute Myeloid Leukemia (Drug Study)Document3 pagesAcute Myeloid Leukemia (Drug Study)Krisianne Mae Lorenzo FranciscoNo ratings yet
- Giant Cell Arteritis: Basic InformationDocument3 pagesGiant Cell Arteritis: Basic Informationjenny grovesNo ratings yet
- Kawasaki - Lab&drug, NCPDocument18 pagesKawasaki - Lab&drug, NCPJayzee ServantesNo ratings yet
- AULIA AHMAD G2A009130 Bab8KTI PDFDocument11 pagesAULIA AHMAD G2A009130 Bab8KTI PDFMargotNo ratings yet
- Mahmood Care BlanDocument5 pagesMahmood Care Blanmahmood asafraNo ratings yet
- Anticoag Peri Op ManagementDocument16 pagesAnticoag Peri Op Managementlokeswara reddyNo ratings yet
- HaemorrhageDocument19 pagesHaemorrhageSrishti SrivastavaNo ratings yet
- UPPER GASTROINTESTINAL BLEEDING Simp HemoroidDocument44 pagesUPPER GASTROINTESTINAL BLEEDING Simp HemoroidKomang YudaNo ratings yet
- LeukemiaDocument1 pageLeukemiaFabshkieee 3No ratings yet
- Anticoagulation TherapyFrom EverandAnticoagulation TherapyJoe F. LauNo ratings yet
- Biomarkers in Various DiseasesDocument3 pagesBiomarkers in Various DiseasespraveenbhavniNo ratings yet
- Chronic Liver DiseaseDocument6 pagesChronic Liver DiseasepraveenbhavniNo ratings yet
- Bed Idden Format For PatientsDocument1 pageBed Idden Format For PatientspraveenbhavniNo ratings yet
- Programme Schedule Workshop-1Document4 pagesProgramme Schedule Workshop-1Ram PattnaikNo ratings yet
- Ortho Final ExamDocument40 pagesOrtho Final ExamMariane GumbanNo ratings yet
- 1 s2.0 S2473952921007515 MainDocument10 pages1 s2.0 S2473952921007515 MainAndreea RacovitaNo ratings yet
- Pash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportDocument3 pagesPash Syndrome Co-Existing With Rheumatic Heart Disease and Severe Mitral Valve Regurgitation: A Rare Case ReportIJAR JOURNALNo ratings yet
- ACLS MedicationsDocument31 pagesACLS MedicationsDrNorNo ratings yet
- How To Write A Research Paper On Prostate CancerDocument4 pagesHow To Write A Research Paper On Prostate Cancertus0zaz1b1g3No ratings yet
- Diploma in DiabetologyDocument8 pagesDiploma in Diabetologydawood260No ratings yet
- Pap SmearDocument24 pagesPap SmearAavash PradhanNo ratings yet
- Autogenic TrainingDocument5 pagesAutogenic Trainingking.fahmie23100% (1)
- E Scleroderma Ye Scleroderma LikeDocument31 pagesE Scleroderma Ye Scleroderma LikeHmn07No ratings yet
- Physical, Leisure, and Daily Living Activities In.3Document11 pagesPhysical, Leisure, and Daily Living Activities In.3yogithajeganathan5197No ratings yet
- Interstitial Lung Diseases2Document186 pagesInterstitial Lung Diseases2Mohamed HefnyNo ratings yet
- Neck Trauma DR Hauwa Shitu 1Document40 pagesNeck Trauma DR Hauwa Shitu 1Hauwa shitu.B100% (1)
- Health Ass.Document6 pagesHealth Ass.Rashmi Devrani VyasNo ratings yet
- (Diabetes) PresentationDocument13 pages(Diabetes) Presentationsabanayyar56No ratings yet
- ATI MedSurg Respiratory System Practice QuestionsDocument19 pagesATI MedSurg Respiratory System Practice QuestionsHHNo ratings yet
- Domestic Violence and AbuseDocument7 pagesDomestic Violence and AbuseKate20100% (1)
- HEALTH 8: Communicable DiseaseDocument31 pagesHEALTH 8: Communicable DiseaseElissah S PabilonaNo ratings yet
- Epiglottitis - AMBOSSDocument10 pagesEpiglottitis - AMBOSSSadikNo ratings yet
- Jain (2003) - Fibromyalgia Syndrome Canadian Clinical Working Case Definition, Diagnostic and Treatment Protocols - A Consensus DocumentDocument106 pagesJain (2003) - Fibromyalgia Syndrome Canadian Clinical Working Case Definition, Diagnostic and Treatment Protocols - A Consensus DocumentLuciana AraújoNo ratings yet
- Mineral, Vitamin, and Herbal SupplementsDocument18 pagesMineral, Vitamin, and Herbal SupplementsismailcemNo ratings yet
- HePatic AbscessDocument67 pagesHePatic AbscessCharlie Mignonette BalaNo ratings yet
- PHAR 233 - Pathophysiology of Infectious DiseasesDocument89 pagesPHAR 233 - Pathophysiology of Infectious DiseasesLina RamojNo ratings yet
- IIRP IG Result 22112023Document11 pagesIIRP IG Result 22112023icmrbharthNo ratings yet
- Medicare GuideDocument3 pagesMedicare GuideyigaplusoneNo ratings yet
- Pivotmed Webinar - Dyspnea in Adult - Approach and Early Management by Dr. Irandi Putra P, PHD, SPP (K), FAPSRDocument36 pagesPivotmed Webinar - Dyspnea in Adult - Approach and Early Management by Dr. Irandi Putra P, PHD, SPP (K), FAPSRMochamad Fadel AuliaNo ratings yet
- NCM 101A 13 Areas of AssessmentDocument4 pagesNCM 101A 13 Areas of AssessmentGladys JhayeNo ratings yet
- Indicador Gabs AtualizadoDocument2 pagesIndicador Gabs AtualizadoBiXus Estrategas EmpresarialesNo ratings yet