Download as xlsx, pdf, or txt
You might also like
- S-990-5131-312 - 1 Progress Measurement ProcedureDocument17 pagesS-990-5131-312 - 1 Progress Measurement ProcedureMahadevan Mahalingam100% (4)
- Saudi Aramco Test Report: Internal Cleanliness Report (Piping Systems & Equip) SATR-A-2008 30-Oct-17 MechDocument2 pagesSaudi Aramco Test Report: Internal Cleanliness Report (Piping Systems & Equip) SATR-A-2008 30-Oct-17 MechJagdishNo ratings yet
- CISA Exam-Testing Concept-Elements of PKI i.e CA/RA/CRL/CPS (Domain-5)From EverandCISA Exam-Testing Concept-Elements of PKI i.e CA/RA/CRL/CPS (Domain-5)Rating: 4 out of 5 stars4/5 (2)
- S-000-5660-051 - B Field Design Change Notice ProcedureDocument6 pagesS-000-5660-051 - B Field Design Change Notice ProcedureMahadevan MahalingamNo ratings yet
- S-000-5140-012 - 0 Coordination Procedure PDFDocument15 pagesS-000-5140-012 - 0 Coordination Procedure PDFMahadevan MahalingamNo ratings yet
- S-000-5138-302 - B Design Change Procedure PDFDocument6 pagesS-000-5138-302 - B Design Change Procedure PDFMahadevan MahalingamNo ratings yet
- Saudi Aramco Test Report: Re-Instatement Punch List Form (Punch List by The Contractor) SATR-A-2011 25-May-05 MechDocument1 pageSaudi Aramco Test Report: Re-Instatement Punch List Form (Punch List by The Contractor) SATR-A-2011 25-May-05 MechAnonymous S9qBDVkyNo ratings yet
- Saic-N - 2002Document1 pageSaic-N - 2002SUNIL RAJPUTNo ratings yet
- In-Process Inspection Report For Fire Proofing: Saudi Aramco Test ReportDocument2 pagesIn-Process Inspection Report For Fire Proofing: Saudi Aramco Test ReportnadeemNo ratings yet
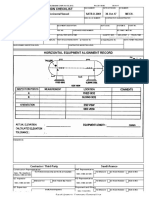
- Saudi Aramco Inspection Checklist: Alignment Inspection Record-Horizontal Vessel SATR-D-2001 24-Jul-18 MechDocument2 pagesSaudi Aramco Inspection Checklist: Alignment Inspection Record-Horizontal Vessel SATR-D-2001 24-Jul-18 Mechnadeem shaikhNo ratings yet
- Saudi Aramco Test Report: Ultrasonic Test Report - TKY Joints SATR-NDE-2005 24-Jul-18 NdeDocument3 pagesSaudi Aramco Test Report: Ultrasonic Test Report - TKY Joints SATR-NDE-2005 24-Jul-18 Ndenadeem shaikhNo ratings yet
- Saudi Aramco Test Report: Refrigerant Pipe Vacuum Test SATR-K-4004 15-Dec-09 HvacDocument1 pageSaudi Aramco Test Report: Refrigerant Pipe Vacuum Test SATR-K-4004 15-Dec-09 HvacWaleed MedhatNo ratings yet
- Saudi Aramco Test Report: Internal Cleanliness Report (Piping Systems & Equip) SATR-A-2008 24-Mar-16 MechDocument2 pagesSaudi Aramco Test Report: Internal Cleanliness Report (Piping Systems & Equip) SATR-A-2008 24-Mar-16 MechSajid ShaikhNo ratings yet
- SF188 Rev 1 - Welder Qualification Test CertificateDocument1 pageSF188 Rev 1 - Welder Qualification Test CertificateMike BoyesNo ratings yet
- Saudi Aramco Test Report: Internal Cleanliness Report (Piping Systems & Equip) SATR-A-2008 24-Jul-18 MechDocument2 pagesSaudi Aramco Test Report: Internal Cleanliness Report (Piping Systems & Equip) SATR-A-2008 24-Jul-18 Mechnadeem0% (1)
- Satr D 2001Document2 pagesSatr D 2001Shahzad HussainNo ratings yet
- Satr Nde 2002Document1 pageSatr Nde 2002nadeem shaikhNo ratings yet
- Satr K 4004Document1 pageSatr K 4004Bander Al–kouhlaniNo ratings yet
- SAIC-A-1014 - Preweld Qualification of HDPE WelderDocument1 pageSAIC-A-1014 - Preweld Qualification of HDPE WelderwalidNo ratings yet
- Saudi Aramco Test Report: Welding Rod Oven Calibration/Verification ReportDocument2 pagesSaudi Aramco Test Report: Welding Rod Oven Calibration/Verification ReportJoni Carino Suni100% (1)
- Saic B 2002Document1 pageSaic B 2002usmanNo ratings yet
- Release Structure For Intumescent Fireproofing (FP) : Saudi Aramco Test ReportDocument2 pagesRelease Structure For Intumescent Fireproofing (FP) : Saudi Aramco Test ReportnadeemNo ratings yet
- 4.lorry LoaderDocument3 pages4.lorry LoaderSHARAFUDHEEN TKNo ratings yet
- Satr H 1003Document2 pagesSatr H 1003Thouseef MaNo ratings yet
- Expansion TankDocument2 pagesExpansion TankSHARAFUDHEEN TKNo ratings yet
- Saudi Aramco Test ReportDocument2 pagesSaudi Aramco Test ReportMoghal AliNo ratings yet
- 4.lorry LoaderDocument3 pages4.lorry LoaderSHARAFUDHEEN TKNo ratings yet
- Saudi Aramco Test Report: Emergency Eyewash/Shower Functional Test Report SATR-B-4001 24-Jul-18 PlumbDocument2 pagesSaudi Aramco Test Report: Emergency Eyewash/Shower Functional Test Report SATR-B-4001 24-Jul-18 PlumbnadeemNo ratings yet
- Saudi Aramco Test Report: Adhesion Test of Fbe Coating SATR-H-2010 CoatDocument2 pagesSaudi Aramco Test Report: Adhesion Test of Fbe Coating SATR-H-2010 CoatnasirNo ratings yet
- Saudi Aramco Inspection Checklist: Alignment Inspection Record-Horizontal Vessel SATR-D-2001 22-Jan-18 MechDocument2 pagesSaudi Aramco Inspection Checklist: Alignment Inspection Record-Horizontal Vessel SATR-D-2001 22-Jan-18 MechaneeshNo ratings yet
- Satr A 2008Document2 pagesSatr A 2008Shahzad HussainNo ratings yet
- Concrete PumpsDocument2 pagesConcrete PumpsSHARAFUDHEEN TKNo ratings yet
- Satr-P-3824 Rev 0Document9 pagesSatr-P-3824 Rev 0lovely mirandaNo ratings yet
- Vacuum Box Test Report - Eff.170628Document1 pageVacuum Box Test Report - Eff.170628Jindarat KasemsooksakulNo ratings yet
- Saudi Aramco Test Report: SATR-B-6105 10-Jun-19 Inst Fire Alarm System - Manual Pull Station - Pre-Commissioning TestDocument2 pagesSaudi Aramco Test Report: SATR-B-6105 10-Jun-19 Inst Fire Alarm System - Manual Pull Station - Pre-Commissioning TestSino hydroNo ratings yet
- Satr D 2001Document2 pagesSatr D 2001razzak.me.enggNo ratings yet
- Saudi Aramco Inspection Checklist: Alignment Inspection Record-Horizontal Vessel SATR-D-2001 30-Oct-17 MechDocument2 pagesSaudi Aramco Inspection Checklist: Alignment Inspection Record-Horizontal Vessel SATR-D-2001 30-Oct-17 MechJagdishNo ratings yet
- Welder's Performancequalification (WPQ) FormDocument1 pageWelder's Performancequalification (WPQ) FormAbhinandan BastiNo ratings yet
- Saudi Aramco Test ReportDocument8 pagesSaudi Aramco Test Reportnadeem shaikhNo ratings yet
- PQD. Shotcrete Abdullah Abdin PDFDocument664 pagesPQD. Shotcrete Abdullah Abdin PDFMuhammad Arif KhanNo ratings yet
- Welder's Performancequalification (WPQ) FormDocument1 pageWelder's Performancequalification (WPQ) FormTegar OktoberNo ratings yet
- WPS Format For ISO 9606-1 WelderDocument2 pagesWPS Format For ISO 9606-1 WelderThe Welding Inspections Community100% (1)
- CBNDT Initial Certification Application FormDocument4 pagesCBNDT Initial Certification Application Formmaddage19No ratings yet
- En Iso 9606 1Document1 pageEn Iso 9606 1Ümitcan TanrıkuluNo ratings yet
- Saudi Aramco Test ReportDocument2 pagesSaudi Aramco Test Reportمحمد علي النويصرNo ratings yet
- Saudi Aramco Test ReportDocument7 pagesSaudi Aramco Test ReportziaNo ratings yet
- Satr W 2008Document2 pagesSatr W 2008mohamed hashimNo ratings yet
- Satr B 4001Document2 pagesSatr B 4001razzak.me.enggNo ratings yet
- Satr W 2012Document1 pageSatr W 2012Mohammed Hamed BaganNo ratings yet
- Satr H 2008Document2 pagesSatr H 2008Moghal AliNo ratings yet
- SAIC-W-2009 Revw-Control of Weld Consum - On PlotDocument1 pageSAIC-W-2009 Revw-Control of Weld Consum - On PlotAnonymous S9qBDVkyNo ratings yet
- Saudi Aramco Inspection ChecklistDocument1 pageSaudi Aramco Inspection ChecklistHaroon odoodNo ratings yet
- Saic A 2004Document8 pagesSaic A 2004karthi51289No ratings yet
- Saudi Aramco Test Report: Positive Material Identification (PMI) Report 24-Jul-18 MechDocument2 pagesSaudi Aramco Test Report: Positive Material Identification (PMI) Report 24-Jul-18 MechnadeemNo ratings yet
- Satr A 2001Document8 pagesSatr A 2001razzak.me.enggNo ratings yet
- Lifting GearDocument2 pagesLifting GearSHARAFUDHEEN TKNo ratings yet
- Satr S 4002Document1 pageSatr S 4002Noor Mohamed AzeezNo ratings yet
- SAIC W 2009 Revw Control of Weld Consum (EE) RLC FFDocument1 pageSAIC W 2009 Revw Control of Weld Consum (EE) RLC FFAnonymous S9qBDVkyNo ratings yet
- Chain Sling-Certificate UpdatedDocument1 pageChain Sling-Certificate UpdatedAkhilNo ratings yet
- EQUIPMENT or MACHINERYDocument1 pageEQUIPMENT or MACHINERYSHARAFUDHEEN TKNo ratings yet
- BGAS-CSWIP Welding and Coating Inspection: Certification, Process, Exam Preparation and Q&AFrom EverandBGAS-CSWIP Welding and Coating Inspection: Certification, Process, Exam Preparation and Q&ANo ratings yet
- Total Quality Process Control for Injection MoldingFrom EverandTotal Quality Process Control for Injection MoldingRating: 5 out of 5 stars5/5 (1)
- T3000-Governer CourseDocument53 pagesT3000-Governer CourseMahadevan MahalingamNo ratings yet
- Check List For Circuit Breaker Data SheetsDocument2 pagesCheck List For Circuit Breaker Data SheetsMahadevan MahalingamNo ratings yet
- Gip - 35 - Motor, Generator, NGTDocument1 pageGip - 35 - Motor, Generator, NGTMahadevan MahalingamNo ratings yet
- S-000-5131-301 - 0 Project Excution PlanDocument35 pagesS-000-5131-301 - 0 Project Excution PlanMahadevan Mahalingam100% (2)
- S-000-5710-056 - 0 Systemezation ProcedureDocument28 pagesS-000-5710-056 - 0 Systemezation ProcedureMahadevan Mahalingam100% (4)
- Att 6. Tentative Commissioning Sequence & System PriorityDocument3 pagesAtt 6. Tentative Commissioning Sequence & System PriorityMahadevan MahalingamNo ratings yet
- S-000-5520-051 - 0 Project Quality PlanDocument34 pagesS-000-5520-051 - 0 Project Quality PlanMahadevan Mahalingam100% (1)
- S-990-5131-311 - 0 Project Control ProcedureDocument15 pagesS-990-5131-311 - 0 Project Control ProcedureMahadevan Mahalingam100% (1)
- QCP For Installation of Neutral Earthing Resistor - Rev. 0Document8 pagesQCP For Installation of Neutral Earthing Resistor - Rev. 0Mahadevan MahalingamNo ratings yet
- S-000-5710-056 - 0 Systemezation ProcedureDocument28 pagesS-000-5710-056 - 0 Systemezation ProcedureMahadevan Mahalingam100% (4)
- S-000-5520-179 - QCP For Installation of Generators - Rev. 0Document9 pagesS-000-5520-179 - QCP For Installation of Generators - Rev. 0Mahadevan MahalingamNo ratings yet
- S-000-5520-182 - QCP For Installation of Batteries, Chargers and UPS - Rev. 0Document8 pagesS-000-5520-182 - QCP For Installation of Batteries, Chargers and UPS - Rev. 0Mahadevan MahalingamNo ratings yet
- S-000-5140-112 - 3 Correspondens ProcedureDocument12 pagesS-000-5140-112 - 3 Correspondens ProcedureMahadevan MahalingamNo ratings yet
- S-000-5520-178 - QCP For Installation of Power Transformers - Rev. 0Document9 pagesS-000-5520-178 - QCP For Installation of Power Transformers - Rev. 0Mahadevan MahalingamNo ratings yet
- S-990-5131-311 - 0 Project Control ProcedureDocument15 pagesS-990-5131-311 - 0 Project Control ProcedureMahadevan Mahalingam100% (1)