
Instant Download Ebook PDF Advanced Piezoelectric Materials Science and Technology PDF Scribd
Instant Download Ebook PDF Advanced Piezoelectric Materials Science and Technology PDF Scribd
You might also like
- Instant Download Ebook PDF Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition PDF Scribdroger.maldonado98596% (56)
- Instant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF Scribdmary.may945100% (49)
- Instant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF Scribdmary.may945100% (49)
- Research Methods in Physical Activity 7th Edition Ebook PDFDocument61 pagesResearch Methods in Physical Activity 7th Edition Ebook PDFdonna.crow358100% (44)
- Instant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF Scribdmary.may945100% (44)
- Instant Download Ebook PDF Advanced Organic Chemistry by David e Lewis PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Organic Chemistry by David e Lewis PDF Scribdroger.maldonado985100% (50)
- Instant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF Scribdmary.may945100% (44)
- Physics of Semiconductor Devices: Third EditionDocument5 pagesPhysics of Semiconductor Devices: Third EditionakashNo ratings yet
- Instant Download Ebook PDF Advanced Pediatric Assessment Second Edition 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Pediatric Assessment Second Edition 2nd Edition PDF Scribdroger.maldonado985100% (46)
- Instant Download Ebook PDF Advances of Dna Computing in Cryptography PDF ScribdDocument47 pagesInstant Download Ebook PDF Advances of Dna Computing in Cryptography PDF Scribdmary.may945100% (55)
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF Scribdmary.may945100% (47)
- Instant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF ScribdDocument42 pagesInstant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF Scribdmary.may945100% (50)
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF Scribdmary.may945100% (51)
- Instant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF ScribdDocument47 pagesInstant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF Scribdmary.may945100% (46)
- Instant Download Ebook PDF Advanced Optical Communication Systems and Networks PDF ScribdDocument26 pagesInstant Download Ebook PDF Advanced Optical Communication Systems and Networks PDF Scribdroger.maldonado985100% (51)
- Instant Download Ebook PDF Advanced Mathematical and Computational Tools in Metrology and Testing X PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Mathematical and Computational Tools in Metrology and Testing X PDF Scribdroger.maldonado985100% (50)
- Instant Download Ebook PDF Advanced Managerial Accounting For Tulane University Custom PDF ScribdDocument42 pagesInstant Download Ebook PDF Advanced Managerial Accounting For Tulane University Custom PDF Scribdroger.maldonado985100% (50)
- Instant Download Ebook PDF Advanced Introduction To Cultural Economics Elgar Advanced Introductions Series PDF ScribdDocument47 pagesInstant Download Ebook PDF Advanced Introduction To Cultural Economics Elgar Advanced Introductions Series PDF Scribdroger.maldonado985100% (47)
- Dwnload Full Concepts of Genetics Books A La Carte Edition 11th Edition Klug Test Bank PDFDocument35 pagesDwnload Full Concepts of Genetics Books A La Carte Edition 11th Edition Klug Test Bank PDFmaryjomacklemus100% (21)
- Dwnload Full Concepts of Genetics 10th Edition Klug Test Bank PDFDocument35 pagesDwnload Full Concepts of Genetics 10th Edition Klug Test Bank PDFmaryjomacklemus100% (19)
- Research Methods Statistics and Applications Second Edition Ebook PDF VersionDocument62 pagesResearch Methods Statistics and Applications Second Edition Ebook PDF Versiondonna.crow358100% (48)
- Dwnload Full Mindtap General Chemistry 4 Terms 24 Months Instant Access 1st Edition Vining Test Bank PDFDocument35 pagesDwnload Full Mindtap General Chemistry 4 Terms 24 Months Instant Access 1st Edition Vining Test Bank PDFhhagyalexik100% (14)
- Dwnload Full Conceptual and Historical Issues in Psychology 1st Edition Piekkola Test Bank PDFDocument35 pagesDwnload Full Conceptual and Historical Issues in Psychology 1st Edition Piekkola Test Bank PDFjameschavezh5w100% (21)
- Dwnload Full Concepts of Programming Languages 10th Edition Sebesta Solutions Manual PDFDocument35 pagesDwnload Full Concepts of Programming Languages 10th Edition Sebesta Solutions Manual PDFmaryjomacklemus100% (18)
- Concepts of Genetics 12th Edition Klug Test BanDwnload Full Concepts of Genetics 12th Edition Klug Test Bank PDFDocument35 pagesConcepts of Genetics 12th Edition Klug Test BanDwnload Full Concepts of Genetics 12th Edition Klug Test Bank PDFmaryjomacklemus100% (17)
- Dwnload Full Mind and Heart of The Negotiator 6th Edition Leigh Thompson Solutions Manual PDFDocument36 pagesDwnload Full Mind and Heart of The Negotiator 6th Edition Leigh Thompson Solutions Manual PDFblackinghemmeldsu0100% (11)
- Speech Acts and Other Topics in Pragmatics 1St Edition Marina Sbisa All ChapterDocument67 pagesSpeech Acts and Other Topics in Pragmatics 1St Edition Marina Sbisa All Chapterglenn.price788100% (6)
- Dwnload Full Conceptual Foundations The Bridge To Professional Nursing Practice 6th Edition Friberg Test Bank PDFDocument36 pagesDwnload Full Conceptual Foundations The Bridge To Professional Nursing Practice 6th Edition Friberg Test Bank PDFjameschavezh5w100% (22)
- Review Questions and Answers For Veterinary Technicians e Book 5th Edition Ebook PDFDocument62 pagesReview Questions and Answers For Veterinary Technicians e Book 5th Edition Ebook PDFdonna.crow358100% (44)
- Sperm Morphology of Domestic Animals J H Koziol All ChapterDocument67 pagesSperm Morphology of Domestic Animals J H Koziol All Chapterglenn.price788100% (6)
- Research Design Qualitative Quantitative and Mixed Methods Approaches 5th Edition Ebook PDFDocument62 pagesResearch Design Qualitative Quantitative and Mixed Methods Approaches 5th Edition Ebook PDFgeorgia.walsh984100% (46)
- Dwnload Full Concepts of Genetics 3rd Edition Brooker Test Bank PDFDocument35 pagesDwnload Full Concepts of Genetics 3rd Edition Brooker Test Bank PDFmaryjomacklemus100% (17)
- Full Download Ebook Ebook PDF Mcsa Guide To Networking With Windows Server 2016 Exam 70 741 PDFDocument41 pagesFull Download Ebook Ebook PDF Mcsa Guide To Networking With Windows Server 2016 Exam 70 741 PDFyolanda.richards657100% (47)
- Textbook Tao of Trauma A Practitioner S Guide For Integrating Five Element Theory and Trauma Treatment Alaine D Duncan Ebook All Chapter PDFDocument53 pagesTextbook Tao of Trauma A Practitioner S Guide For Integrating Five Element Theory and Trauma Treatment Alaine D Duncan Ebook All Chapter PDFkeith.martin541100% (2)
- Dwnload Full Concepts of Database Management 9th Edition Starks Solutions Manual PDFDocument35 pagesDwnload Full Concepts of Database Management 9th Edition Starks Solutions Manual PDFmaryjomacklemus100% (20)
- Managerial Economics 4th EditionDocument57 pagesManagerial Economics 4th Editionmaria.bowman208100% (46)
- (Ebook PDF) (Ebook PDF) Advanced Piezoelectric Materials: Science and Technology All ChapterDocument43 pages(Ebook PDF) (Ebook PDF) Advanced Piezoelectric Materials: Science and Technology All Chapternartgeyer5100% (5)
- Full Download Ebook PDF Nanomaterials For Solar Cell Applications by Sabu Thomas PDFDocument41 pagesFull Download Ebook PDF Nanomaterials For Solar Cell Applications by Sabu Thomas PDFdarlene.marin926100% (35)
- TLKS10 PDFDocument70 pagesTLKS10 PDFCommon E-Mail IDNo ratings yet
- Full Download PDF of (Ebook PDF) Organic Structure Analysis (Topics in Organic Chemistry) 2nd Edition All ChapterDocument43 pagesFull Download PDF of (Ebook PDF) Organic Structure Analysis (Topics in Organic Chemistry) 2nd Edition All Chaptervengarelgen48100% (8)
- Organic Structure Analysis Topics in Organic Chemistry 2Nd Edition Full ChapterDocument41 pagesOrganic Structure Analysis Topics in Organic Chemistry 2Nd Edition Full Chapterpok.maroney137100% (25)
- (Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and RemediationDocument42 pages(Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and Remediationfranklin.mayer855100% (46)
- (Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and RemediationDocument43 pages(Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and Remediationpugllohman80100% (7)
- Organic Ferroelectric Materials and Applications (Woodhead Publishing Series in Electronic and Optical Materials) 1st Edition Kamal Asadi (Editor)Document54 pagesOrganic Ferroelectric Materials and Applications (Woodhead Publishing Series in Electronic and Optical Materials) 1st Edition Kamal Asadi (Editor)sisleykerols8100% (5)
- Nano IntroDocument12 pagesNano Introdrakshaykumar.nano100% (1)
- J. Walter Schultze, Tetsuya Osaka, Madhav DattaDocument588 pagesJ. Walter Schultze, Tetsuya Osaka, Madhav DattaAhmed AbassNo ratings yet
- PHI Book PDFDocument12 pagesPHI Book PDFSreerajNo ratings yet
- Physics of Semiconductor Devices: Third EditionDocument5 pagesPhysics of Semiconductor Devices: Third EditionRafael Becker MacielNo ratings yet
- Physics of Semiconductor Devices: Third EditionDocument5 pagesPhysics of Semiconductor Devices: Third EditionZafar IqbalNo ratings yet
- Finalmodifiedsateoftheart 2Document70 pagesFinalmodifiedsateoftheart 2Muqsit Muhammad Hanif100% (1)
- PDF Advances in Thin Film Solar Cells Second Edition Dharmadasa Ebook Full ChapterDocument53 pagesPDF Advances in Thin Film Solar Cells Second Edition Dharmadasa Ebook Full Chapterstanley.mullins394100% (6)
- Wide Band Gap SemiconductorsDocument45 pagesWide Band Gap SemiconductorspawaniitkgpNo ratings yet
- Diode LasersDocument456 pagesDiode Laserswlltld100% (29)
- Synthesis and Characterization of Nano Banana Fibre Reinforced Polymer Nano CompositesDocument133 pagesSynthesis and Characterization of Nano Banana Fibre Reinforced Polymer Nano CompositesBoopathi RajaNo ratings yet
- Final Report UGC 30122019Document137 pagesFinal Report UGC 30122019Vishnu PNo ratings yet
- Solid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Chunwen Sun All ChapterDocument67 pagesSolid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Chunwen Sun All Chapterraymond.benson235100% (3)
- Nanoelectronics PDFDocument347 pagesNanoelectronics PDFJoyline GermineNo ratings yet
- Nanowire Energy Storage Devices Synthesis Characterization and Applications Liqiang Mai Full ChapterDocument67 pagesNanowire Energy Storage Devices Synthesis Characterization and Applications Liqiang Mai Full Chapterjames.lamblin744100% (10)
- Solid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH Full Chapter PDFDocument69 pagesSolid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH Full Chapter PDFseydyabzeta9100% (5)
- Solid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH All ChapterDocument67 pagesSolid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH All Chapterroy.morey622100% (7)
- MY ThesisDocument39 pagesMY ThesisSantosh SainiNo ratings yet
- Ferroelectric Devices: Kenji UchinoDocument10 pagesFerroelectric Devices: Kenji UchinoMANAS KUMAR RATHNo ratings yet
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF Scribdmary.may945100% (47)
- Instant Download Ebook PDF Advances of Dna Computing in Cryptography PDF ScribdDocument47 pagesInstant Download Ebook PDF Advances of Dna Computing in Cryptography PDF Scribdmary.may945100% (55)
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF Scribdmary.may945100% (51)
- Instant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF ScribdDocument47 pagesInstant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF Scribdmary.may945100% (46)
- Instant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF ScribdDocument42 pagesInstant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF Scribdmary.may945100% (50)
- The Human Element at WorkDocument5 pagesThe Human Element at Workyog_uict9248No ratings yet
- A Study of The Exposure To Wood Dust and Potential Impact On Lung FunctionDocument9 pagesA Study of The Exposure To Wood Dust and Potential Impact On Lung FunctionIin Sakinah DewiNo ratings yet
- LTL-X Software Manual - UKDocument19 pagesLTL-X Software Manual - UKHanif Yusfaula ZNo ratings yet
- Agrirobot PDFDocument103 pagesAgrirobot PDFMuhamad Azlan ShahNo ratings yet
- (Book) Zero EnergyDocument155 pages(Book) Zero EnergycacaNo ratings yet
- Chart Patterns: Symmetrical Triangles The Ascending TriangleDocument8 pagesChart Patterns: Symmetrical Triangles The Ascending TriangleGene Stanley100% (1)
- Grade 6 Worksheet 2Document2 pagesGrade 6 Worksheet 2Ramocles FernandoNo ratings yet
- Chapter 6 Financial AssetsDocument6 pagesChapter 6 Financial AssetsJoyce Mae D. FloresNo ratings yet
- SolidCAM 2015 IMachining FAQDocument55 pagesSolidCAM 2015 IMachining FAQhed_panNo ratings yet
- Unit-14 Maintenance BookDocument57 pagesUnit-14 Maintenance Bookrama_subbuNo ratings yet
- Unveiling The Cosmic Canvas: Pre-Order AstroDunia's 2024 Investment OdysseyDocument2 pagesUnveiling The Cosmic Canvas: Pre-Order AstroDunia's 2024 Investment OdysseyastroduniaNo ratings yet
- Celebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)Document8 pagesCelebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)RIZKINo ratings yet
- DR - Nitish Kumar - CV ..Document6 pagesDR - Nitish Kumar - CV ..ABHISHEK SINGHNo ratings yet
- TechTalk Updated IEST-RP-CC012 A Must ReadDocument4 pagesTechTalk Updated IEST-RP-CC012 A Must ReadShivkumar Sharma100% (1)
- AI Business IdeasDocument12 pagesAI Business IdeasYasir ButtNo ratings yet
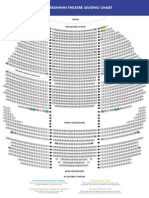
- The Gershwin Theatre Seating Chart: StageDocument1 pageThe Gershwin Theatre Seating Chart: StageCharles DavidsonNo ratings yet
- Abhishek Shukla Project Reporton (Power Purchase)Document57 pagesAbhishek Shukla Project Reporton (Power Purchase)beast singhNo ratings yet
- Y8 History 2020Document44 pagesY8 History 2020mahaNo ratings yet
- Caspah - Kamunda 1593513704 ADocument42 pagesCaspah - Kamunda 1593513704 Ajoseph wamulumeNo ratings yet
- Risk Management in Islamic BankingDocument17 pagesRisk Management in Islamic BankingEdi SusiloNo ratings yet
- Illinois State Board of Education: General InformationDocument40 pagesIllinois State Board of Education: General InformationLeslie AtkinsonNo ratings yet
- Stat Fax 3300 Chemistry AnalyzerDocument2 pagesStat Fax 3300 Chemistry AnalyzermohamedNo ratings yet
- Hendricks, David W - Fundamentals of Water Treatment Unit Processes - Physical, Chemical, and Biological-CRC Press (2011)Document930 pagesHendricks, David W - Fundamentals of Water Treatment Unit Processes - Physical, Chemical, and Biological-CRC Press (2011)Héctor RomeroNo ratings yet
- Phrasal Verb LESSON FINAL 1701874327225Document67 pagesPhrasal Verb LESSON FINAL 1701874327225bgt dfgNo ratings yet
- Laguna State Polytechnic University: Bachelor of Science in Agricultural EducationDocument14 pagesLaguna State Polytechnic University: Bachelor of Science in Agricultural EducationmutedchildNo ratings yet
- Diaphragm and Lung Ultrasound To Predict Weaning Outcome: Systematic Review and Meta-AnalysisDocument11 pagesDiaphragm and Lung Ultrasound To Predict Weaning Outcome: Systematic Review and Meta-AnalysisPablo IgnacioNo ratings yet
- Luci Hulme Research AnalysisDocument16 pagesLuci Hulme Research Analysisapi-358990183No ratings yet
- DHS Coast Guard LetterDocument13 pagesDHS Coast Guard LetterThe Hill NewspaperNo ratings yet
- 8 SWOT Analysis Tools For Small Businesses: 1. SmartsheetDocument3 pages8 SWOT Analysis Tools For Small Businesses: 1. SmartsheetSantu BiswaaNo ratings yet
- Assignment Name: Identifying Characteristics of Some Family With 5 ExamplesDocument4 pagesAssignment Name: Identifying Characteristics of Some Family With 5 ExamplesAbdullah Al MamunNo ratings yet
























































































Download as pdf or txt
You might also like
- Instant Download Ebook PDF Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition PDF Scribdroger.maldonado98596% (56)
- Instant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF Scribdmary.may945100% (49)
- Instant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advances in Sport and Exercise Psychology 4th Edition PDF Scribdmary.may945100% (49)
- Research Methods in Physical Activity 7th Edition Ebook PDFDocument61 pagesResearch Methods in Physical Activity 7th Edition Ebook PDFdonna.crow358100% (44)
- Instant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF Scribdmary.may945100% (44)
- Instant Download Ebook PDF Advanced Organic Chemistry by David e Lewis PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Organic Chemistry by David e Lewis PDF Scribdroger.maldonado985100% (50)
- Instant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Public Speaking A Leaders Guide 2nd Edition PDF Scribdmary.may945100% (44)
- Physics of Semiconductor Devices: Third EditionDocument5 pagesPhysics of Semiconductor Devices: Third EditionakashNo ratings yet
- Instant Download Ebook PDF Advanced Pediatric Assessment Second Edition 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Pediatric Assessment Second Edition 2nd Edition PDF Scribdroger.maldonado985100% (46)
- Instant Download Ebook PDF Advances of Dna Computing in Cryptography PDF ScribdDocument47 pagesInstant Download Ebook PDF Advances of Dna Computing in Cryptography PDF Scribdmary.may945100% (55)
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF Scribdmary.may945100% (47)
- Instant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF ScribdDocument42 pagesInstant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF Scribdmary.may945100% (50)
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF Scribdmary.may945100% (51)
- Instant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF ScribdDocument47 pagesInstant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF Scribdmary.may945100% (46)
- Instant Download Ebook PDF Advanced Optical Communication Systems and Networks PDF ScribdDocument26 pagesInstant Download Ebook PDF Advanced Optical Communication Systems and Networks PDF Scribdroger.maldonado985100% (51)
- Instant Download Ebook PDF Advanced Mathematical and Computational Tools in Metrology and Testing X PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Mathematical and Computational Tools in Metrology and Testing X PDF Scribdroger.maldonado985100% (50)
- Instant Download Ebook PDF Advanced Managerial Accounting For Tulane University Custom PDF ScribdDocument42 pagesInstant Download Ebook PDF Advanced Managerial Accounting For Tulane University Custom PDF Scribdroger.maldonado985100% (50)
- Instant Download Ebook PDF Advanced Introduction To Cultural Economics Elgar Advanced Introductions Series PDF ScribdDocument47 pagesInstant Download Ebook PDF Advanced Introduction To Cultural Economics Elgar Advanced Introductions Series PDF Scribdroger.maldonado985100% (47)
- Dwnload Full Concepts of Genetics Books A La Carte Edition 11th Edition Klug Test Bank PDFDocument35 pagesDwnload Full Concepts of Genetics Books A La Carte Edition 11th Edition Klug Test Bank PDFmaryjomacklemus100% (21)
- Dwnload Full Concepts of Genetics 10th Edition Klug Test Bank PDFDocument35 pagesDwnload Full Concepts of Genetics 10th Edition Klug Test Bank PDFmaryjomacklemus100% (19)
- Research Methods Statistics and Applications Second Edition Ebook PDF VersionDocument62 pagesResearch Methods Statistics and Applications Second Edition Ebook PDF Versiondonna.crow358100% (48)
- Dwnload Full Mindtap General Chemistry 4 Terms 24 Months Instant Access 1st Edition Vining Test Bank PDFDocument35 pagesDwnload Full Mindtap General Chemistry 4 Terms 24 Months Instant Access 1st Edition Vining Test Bank PDFhhagyalexik100% (14)
- Dwnload Full Conceptual and Historical Issues in Psychology 1st Edition Piekkola Test Bank PDFDocument35 pagesDwnload Full Conceptual and Historical Issues in Psychology 1st Edition Piekkola Test Bank PDFjameschavezh5w100% (21)
- Dwnload Full Concepts of Programming Languages 10th Edition Sebesta Solutions Manual PDFDocument35 pagesDwnload Full Concepts of Programming Languages 10th Edition Sebesta Solutions Manual PDFmaryjomacklemus100% (18)
- Concepts of Genetics 12th Edition Klug Test BanDwnload Full Concepts of Genetics 12th Edition Klug Test Bank PDFDocument35 pagesConcepts of Genetics 12th Edition Klug Test BanDwnload Full Concepts of Genetics 12th Edition Klug Test Bank PDFmaryjomacklemus100% (17)
- Dwnload Full Mind and Heart of The Negotiator 6th Edition Leigh Thompson Solutions Manual PDFDocument36 pagesDwnload Full Mind and Heart of The Negotiator 6th Edition Leigh Thompson Solutions Manual PDFblackinghemmeldsu0100% (11)
- Speech Acts and Other Topics in Pragmatics 1St Edition Marina Sbisa All ChapterDocument67 pagesSpeech Acts and Other Topics in Pragmatics 1St Edition Marina Sbisa All Chapterglenn.price788100% (6)
- Dwnload Full Conceptual Foundations The Bridge To Professional Nursing Practice 6th Edition Friberg Test Bank PDFDocument36 pagesDwnload Full Conceptual Foundations The Bridge To Professional Nursing Practice 6th Edition Friberg Test Bank PDFjameschavezh5w100% (22)
- Review Questions and Answers For Veterinary Technicians e Book 5th Edition Ebook PDFDocument62 pagesReview Questions and Answers For Veterinary Technicians e Book 5th Edition Ebook PDFdonna.crow358100% (44)
- Sperm Morphology of Domestic Animals J H Koziol All ChapterDocument67 pagesSperm Morphology of Domestic Animals J H Koziol All Chapterglenn.price788100% (6)
- Research Design Qualitative Quantitative and Mixed Methods Approaches 5th Edition Ebook PDFDocument62 pagesResearch Design Qualitative Quantitative and Mixed Methods Approaches 5th Edition Ebook PDFgeorgia.walsh984100% (46)
- Dwnload Full Concepts of Genetics 3rd Edition Brooker Test Bank PDFDocument35 pagesDwnload Full Concepts of Genetics 3rd Edition Brooker Test Bank PDFmaryjomacklemus100% (17)
- Full Download Ebook Ebook PDF Mcsa Guide To Networking With Windows Server 2016 Exam 70 741 PDFDocument41 pagesFull Download Ebook Ebook PDF Mcsa Guide To Networking With Windows Server 2016 Exam 70 741 PDFyolanda.richards657100% (47)
- Textbook Tao of Trauma A Practitioner S Guide For Integrating Five Element Theory and Trauma Treatment Alaine D Duncan Ebook All Chapter PDFDocument53 pagesTextbook Tao of Trauma A Practitioner S Guide For Integrating Five Element Theory and Trauma Treatment Alaine D Duncan Ebook All Chapter PDFkeith.martin541100% (2)
- Dwnload Full Concepts of Database Management 9th Edition Starks Solutions Manual PDFDocument35 pagesDwnload Full Concepts of Database Management 9th Edition Starks Solutions Manual PDFmaryjomacklemus100% (20)
- Managerial Economics 4th EditionDocument57 pagesManagerial Economics 4th Editionmaria.bowman208100% (46)
- (Ebook PDF) (Ebook PDF) Advanced Piezoelectric Materials: Science and Technology All ChapterDocument43 pages(Ebook PDF) (Ebook PDF) Advanced Piezoelectric Materials: Science and Technology All Chapternartgeyer5100% (5)
- Full Download Ebook PDF Nanomaterials For Solar Cell Applications by Sabu Thomas PDFDocument41 pagesFull Download Ebook PDF Nanomaterials For Solar Cell Applications by Sabu Thomas PDFdarlene.marin926100% (35)
- TLKS10 PDFDocument70 pagesTLKS10 PDFCommon E-Mail IDNo ratings yet
- Full Download PDF of (Ebook PDF) Organic Structure Analysis (Topics in Organic Chemistry) 2nd Edition All ChapterDocument43 pagesFull Download PDF of (Ebook PDF) Organic Structure Analysis (Topics in Organic Chemistry) 2nd Edition All Chaptervengarelgen48100% (8)
- Organic Structure Analysis Topics in Organic Chemistry 2Nd Edition Full ChapterDocument41 pagesOrganic Structure Analysis Topics in Organic Chemistry 2Nd Edition Full Chapterpok.maroney137100% (25)
- (Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and RemediationDocument42 pages(Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and Remediationfranklin.mayer855100% (46)
- (Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and RemediationDocument43 pages(Ebook PDF) Biomass, Biofuels, Biochemicals: Microbial Electrochemical Technology: Sustainable Platform For Fuels, Chemicals and Remediationpugllohman80100% (7)
- Organic Ferroelectric Materials and Applications (Woodhead Publishing Series in Electronic and Optical Materials) 1st Edition Kamal Asadi (Editor)Document54 pagesOrganic Ferroelectric Materials and Applications (Woodhead Publishing Series in Electronic and Optical Materials) 1st Edition Kamal Asadi (Editor)sisleykerols8100% (5)
- Nano IntroDocument12 pagesNano Introdrakshaykumar.nano100% (1)
- J. Walter Schultze, Tetsuya Osaka, Madhav DattaDocument588 pagesJ. Walter Schultze, Tetsuya Osaka, Madhav DattaAhmed AbassNo ratings yet
- PHI Book PDFDocument12 pagesPHI Book PDFSreerajNo ratings yet
- Physics of Semiconductor Devices: Third EditionDocument5 pagesPhysics of Semiconductor Devices: Third EditionRafael Becker MacielNo ratings yet
- Physics of Semiconductor Devices: Third EditionDocument5 pagesPhysics of Semiconductor Devices: Third EditionZafar IqbalNo ratings yet
- Finalmodifiedsateoftheart 2Document70 pagesFinalmodifiedsateoftheart 2Muqsit Muhammad Hanif100% (1)
- PDF Advances in Thin Film Solar Cells Second Edition Dharmadasa Ebook Full ChapterDocument53 pagesPDF Advances in Thin Film Solar Cells Second Edition Dharmadasa Ebook Full Chapterstanley.mullins394100% (6)
- Wide Band Gap SemiconductorsDocument45 pagesWide Band Gap SemiconductorspawaniitkgpNo ratings yet
- Diode LasersDocument456 pagesDiode Laserswlltld100% (29)
- Synthesis and Characterization of Nano Banana Fibre Reinforced Polymer Nano CompositesDocument133 pagesSynthesis and Characterization of Nano Banana Fibre Reinforced Polymer Nano CompositesBoopathi RajaNo ratings yet
- Final Report UGC 30122019Document137 pagesFinal Report UGC 30122019Vishnu PNo ratings yet
- Solid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Chunwen Sun All ChapterDocument67 pagesSolid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Chunwen Sun All Chapterraymond.benson235100% (3)
- Nanoelectronics PDFDocument347 pagesNanoelectronics PDFJoyline GermineNo ratings yet
- Nanowire Energy Storage Devices Synthesis Characterization and Applications Liqiang Mai Full ChapterDocument67 pagesNanowire Energy Storage Devices Synthesis Characterization and Applications Liqiang Mai Full Chapterjames.lamblin744100% (10)
- Solid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH Full Chapter PDFDocument69 pagesSolid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH Full Chapter PDFseydyabzeta9100% (5)
- Solid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH All ChapterDocument67 pagesSolid Oxide Fuel Cells From Electrolyte Based To Electrolyte Free Devices Wiley VCH All Chapterroy.morey622100% (7)
- MY ThesisDocument39 pagesMY ThesisSantosh SainiNo ratings yet
- Ferroelectric Devices: Kenji UchinoDocument10 pagesFerroelectric Devices: Kenji UchinoMANAS KUMAR RATHNo ratings yet
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults PDF Scribdmary.may945100% (47)
- Instant Download Ebook PDF Advances of Dna Computing in Cryptography PDF ScribdDocument47 pagesInstant Download Ebook PDF Advances of Dna Computing in Cryptography PDF Scribdmary.may945100% (55)
- Instant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Advanced Practice Nursing in The Care of Older Adults 2nd Edition PDF Scribdmary.may945100% (51)
- Instant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF ScribdDocument47 pagesInstant Download Ebook PDF Advanced Sales Management Handbook and Cases PDF Scribdmary.may945100% (46)
- Instant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF ScribdDocument42 pagesInstant Download Ebook PDF Advanced Practice Nursing Essentials For Role Development 4th Edition PDF Scribdmary.may945100% (50)
- The Human Element at WorkDocument5 pagesThe Human Element at Workyog_uict9248No ratings yet
- A Study of The Exposure To Wood Dust and Potential Impact On Lung FunctionDocument9 pagesA Study of The Exposure To Wood Dust and Potential Impact On Lung FunctionIin Sakinah DewiNo ratings yet
- LTL-X Software Manual - UKDocument19 pagesLTL-X Software Manual - UKHanif Yusfaula ZNo ratings yet
- Agrirobot PDFDocument103 pagesAgrirobot PDFMuhamad Azlan ShahNo ratings yet
- (Book) Zero EnergyDocument155 pages(Book) Zero EnergycacaNo ratings yet
- Chart Patterns: Symmetrical Triangles The Ascending TriangleDocument8 pagesChart Patterns: Symmetrical Triangles The Ascending TriangleGene Stanley100% (1)
- Grade 6 Worksheet 2Document2 pagesGrade 6 Worksheet 2Ramocles FernandoNo ratings yet
- Chapter 6 Financial AssetsDocument6 pagesChapter 6 Financial AssetsJoyce Mae D. FloresNo ratings yet
- SolidCAM 2015 IMachining FAQDocument55 pagesSolidCAM 2015 IMachining FAQhed_panNo ratings yet
- Unit-14 Maintenance BookDocument57 pagesUnit-14 Maintenance Bookrama_subbuNo ratings yet
- Unveiling The Cosmic Canvas: Pre-Order AstroDunia's 2024 Investment OdysseyDocument2 pagesUnveiling The Cosmic Canvas: Pre-Order AstroDunia's 2024 Investment OdysseyastroduniaNo ratings yet
- Celebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)Document8 pagesCelebrity's Self-Disclosure On Twitter and Parasocial Relationships (Mediating Soc Presence)RIZKINo ratings yet
- DR - Nitish Kumar - CV ..Document6 pagesDR - Nitish Kumar - CV ..ABHISHEK SINGHNo ratings yet
- TechTalk Updated IEST-RP-CC012 A Must ReadDocument4 pagesTechTalk Updated IEST-RP-CC012 A Must ReadShivkumar Sharma100% (1)
- AI Business IdeasDocument12 pagesAI Business IdeasYasir ButtNo ratings yet
- The Gershwin Theatre Seating Chart: StageDocument1 pageThe Gershwin Theatre Seating Chart: StageCharles DavidsonNo ratings yet
- Abhishek Shukla Project Reporton (Power Purchase)Document57 pagesAbhishek Shukla Project Reporton (Power Purchase)beast singhNo ratings yet
- Y8 History 2020Document44 pagesY8 History 2020mahaNo ratings yet
- Caspah - Kamunda 1593513704 ADocument42 pagesCaspah - Kamunda 1593513704 Ajoseph wamulumeNo ratings yet
- Risk Management in Islamic BankingDocument17 pagesRisk Management in Islamic BankingEdi SusiloNo ratings yet
- Illinois State Board of Education: General InformationDocument40 pagesIllinois State Board of Education: General InformationLeslie AtkinsonNo ratings yet
- Stat Fax 3300 Chemistry AnalyzerDocument2 pagesStat Fax 3300 Chemistry AnalyzermohamedNo ratings yet
- Hendricks, David W - Fundamentals of Water Treatment Unit Processes - Physical, Chemical, and Biological-CRC Press (2011)Document930 pagesHendricks, David W - Fundamentals of Water Treatment Unit Processes - Physical, Chemical, and Biological-CRC Press (2011)Héctor RomeroNo ratings yet
- Phrasal Verb LESSON FINAL 1701874327225Document67 pagesPhrasal Verb LESSON FINAL 1701874327225bgt dfgNo ratings yet
- Laguna State Polytechnic University: Bachelor of Science in Agricultural EducationDocument14 pagesLaguna State Polytechnic University: Bachelor of Science in Agricultural EducationmutedchildNo ratings yet
- Diaphragm and Lung Ultrasound To Predict Weaning Outcome: Systematic Review and Meta-AnalysisDocument11 pagesDiaphragm and Lung Ultrasound To Predict Weaning Outcome: Systematic Review and Meta-AnalysisPablo IgnacioNo ratings yet
- Luci Hulme Research AnalysisDocument16 pagesLuci Hulme Research Analysisapi-358990183No ratings yet
- DHS Coast Guard LetterDocument13 pagesDHS Coast Guard LetterThe Hill NewspaperNo ratings yet
- 8 SWOT Analysis Tools For Small Businesses: 1. SmartsheetDocument3 pages8 SWOT Analysis Tools For Small Businesses: 1. SmartsheetSantu BiswaaNo ratings yet
- Assignment Name: Identifying Characteristics of Some Family With 5 ExamplesDocument4 pagesAssignment Name: Identifying Characteristics of Some Family With 5 ExamplesAbdullah Al MamunNo ratings yet