Download as pdf or txt
You might also like
- Your 5 Moments For Hand Hygiene PosterDocument1 pageYour 5 Moments For Hand Hygiene PosterAniruddha Bagchi100% (1)
- SleepFoundation SleepDiaryDocument1 pageSleepFoundation SleepDiarySahar MalikNo ratings yet
- SleepFoundation SleepDiaryDocument1 pageSleepFoundation SleepDiaryJowel HossainNo ratings yet
- Kami ExportDocument1 pageKami Exportjohn mamaNo ratings yet
- SleepFoundation SleepDiaryDocument1 pageSleepFoundation SleepDiaryIsabela MacapugayNo ratings yet
- SleepDiaryv6 PDFDocument2 pagesSleepDiaryv6 PDFTiara MardalifaNo ratings yet
- Sleep Diary: How To Use The National Sleep Foundation Sleep DiaryDocument4 pagesSleep Diary: How To Use The National Sleep Foundation Sleep DiaryLeon MakNo ratings yet
- DATEDocument1 pageDATEDante Duruin UrmatamNo ratings yet
- Sleep Diary PDFDocument1 pageSleep Diary PDFrobNo ratings yet
- Sleep LogDocument1 pageSleep LogSanskriti BagariaNo ratings yet
- Revision TimetableDocument1 pageRevision TimetableJeremy DudleyNo ratings yet
- One Week Sleep DiaryDocument2 pagesOne Week Sleep DiaryainiNo ratings yet
- UntitledDocument1 pageUntitledMaria José Cruz OlivaNo ratings yet
- Inside Booklet For Summer 2019Document8 pagesInside Booklet For Summer 2019Sindangan Adventist CenterChurch ChoirNo ratings yet
- GlosTema4Ing1 CorregidoDocument5 pagesGlosTema4Ing1 CorregidoAna LinaresNo ratings yet
- Class Preparation FormatsDocument3 pagesClass Preparation FormatsImplere SomnisNo ratings yet
- SleepDocument15 pagesSleepapi-508753814No ratings yet
- Biological Engineering Weekly Goal SettingDocument10 pagesBiological Engineering Weekly Goal SettingalyssacortezxNo ratings yet
- Sleep and Dreams Log: For Two Weeks, Keep This Log Daily. Be As Detailed As PossibleDocument4 pagesSleep and Dreams Log: For Two Weeks, Keep This Log Daily. Be As Detailed As PossibleEvan MaurNo ratings yet
- Hora RioDocument1 pageHora RioJorge ArcadioNo ratings yet
- SFU 5 Day Challenge - Are You Ready - !Document7 pagesSFU 5 Day Challenge - Are You Ready - !Jehovani Tena SánchezNo ratings yet
- MG - Check ListDocument1 pageMG - Check ListMg WillemseNo ratings yet
- Time Management - Jaylyne Mcduffie - Sheet1Document1 pageTime Management - Jaylyne Mcduffie - Sheet1api-707168417No ratings yet
- Sleep DiaryDocument3 pagesSleep Diaryhonor dobbieNo ratings yet
- Schedule of ClassesDocument5 pagesSchedule of Classes2022-09-103No ratings yet
- Fixed Commitment CalendarDocument1 pageFixed Commitment CalendarNASRIAH JAMALUDINNo ratings yet
- Timelog & Weekly Calendar VincoyDocument3 pagesTimelog & Weekly Calendar VincoyArive, Lord CedricNo ratings yet
- Your Time: NameDocument2 pagesYour Time: NameuyenNo ratings yet
- What's The TimeDocument34 pagesWhat's The TimeЮлия РоманчукNo ratings yet
- Sleep LogDocument2 pagesSleep LogNadia AhmedNo ratings yet
- 2024 New Excel Calendar With ShiftsDocument24 pages2024 New Excel Calendar With ShiftsYounes AzzirariNo ratings yet
- CBT-I_group_Session 1_revised_7_11_23Document35 pagesCBT-I_group_Session 1_revised_7_11_23lallycNo ratings yet
- APOLDocument3 pagesAPOLmataoyanniegrey11No ratings yet
- Step 1 6 Week CalendarDocument3 pagesStep 1 6 Week CalendarKawther Abdallah0% (1)
- Your English Has Become RustyDocument1 pageYour English Has Become RustyKorchi IlyassNo ratings yet
- Sleep Diary FILLABLEDocument1 pageSleep Diary FILLABLETATA STEELNo ratings yet
- BEEP 5tema1 New BeepDocument2 pagesBEEP 5tema1 New BeepKarola CosmeNo ratings yet
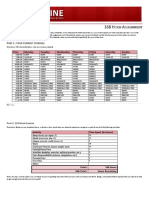
- 168 Hour Assignment (Compatible Version)Document3 pages168 Hour Assignment (Compatible Version)DawnNo ratings yet
- Insomnia QuestionnaireDocument6 pagesInsomnia QuestionnaireNuradila Athirah LockmanNo ratings yet
- Print AbleDocument1 pagePrint AbleAdrian BarkusNo ratings yet
- L'alphabetDocument20 pagesL'alphabetJinal ShahNo ratings yet
- Calendar - 2024 06 02 - 2024 06 09Document1 pageCalendar - 2024 06 02 - 2024 06 09emenceeNo ratings yet
- Verbs: Interactive Student's VocabularyDocument2 pagesVerbs: Interactive Student's VocabularyLuuppiittaa Saan'z DionneNo ratings yet
- The Daily Plan For Your BabyDocument9 pagesThe Daily Plan For Your BabyIsabela BealcuNo ratings yet
- Schedule DVBSDocument1 pageSchedule DVBSDoble, Christopher JohnNo ratings yet
- تايم فور انجلش - 5 ابتدائي ترم 1 - مذكرة 5Document75 pagesتايم فور انجلش - 5 ابتدائي ترم 1 - مذكرة 5shimaa saeedNo ratings yet
- Control de AseoDocument1 pageControl de AseolaboratorioopticoretinocularNo ratings yet
- Questionnaire Sleep DeprivationDocument1 pageQuestionnaire Sleep Deprivationcharah dalmNo ratings yet
- Every HourDocument1 pageEvery HourdberkNo ratings yet
- Year 3 Maths Worksheets Telling The Time Worksheets 4 Levels of DifficultyDocument8 pagesYear 3 Maths Worksheets Telling The Time Worksheets 4 Levels of DifficultyHatakishore BeheraNo ratings yet
- Nuddbelanger Progress MonitoringDocument6 pagesNuddbelanger Progress Monitoringapi-199087465No ratings yet
- Printable Employee Attendance SheetDocument2 pagesPrintable Employee Attendance Sheetjojofuellas22No ratings yet
- My Daily Time ManagementDocument1 pageMy Daily Time ManagementhumuanniNo ratings yet
- GMF L2 Grammar BoostersDocument18 pagesGMF L2 Grammar BoostersRooNo ratings yet
- Sunday Monday Tuesday Wednesday Thursday Friday Saturday: Sheryl Dela Cruz, 1-11Document1 pageSunday Monday Tuesday Wednesday Thursday Friday Saturday: Sheryl Dela Cruz, 1-11s. dela cruz, BLJDONo ratings yet
- W 11 Sleep DiaryDocument2 pagesW 11 Sleep Diaryapi-272309060No ratings yet
- Homeschooling Take 2Document5 pagesHomeschooling Take 2川上 さくらNo ratings yet
- Jadual Kelas 2020Document6 pagesJadual Kelas 2020ishamNo ratings yet
- Can You Cheat by Sleeping in Bits?Document1 pageCan You Cheat by Sleeping in Bits?The Spooky SerbNo ratings yet
- Summer Camp 1st Week July 2023Document6 pagesSummer Camp 1st Week July 2023RabbiyaNo ratings yet
- Discover Your DietDocument51 pagesDiscover Your DietAkanksha SinghNo ratings yet
- 2 Claim Form A - Other Than PA and TravelDocument3 pages2 Claim Form A - Other Than PA and TravelEkta ChauhanNo ratings yet
- Safety and Health at Work: Original ArticleDocument7 pagesSafety and Health at Work: Original ArticlePipe GonzalezNo ratings yet
- Salwa Maghrabi Teacher Assistant Nursing Department: Prepared byDocument30 pagesSalwa Maghrabi Teacher Assistant Nursing Department: Prepared byPearl DiBerardino100% (1)
- Compliance Program in HealthcareDocument31 pagesCompliance Program in HealthcareJorge Ignacio Muñoz MartinezNo ratings yet
- Safety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingDocument12 pagesSafety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakinglxd.hepNo ratings yet
- Ipc and Food Handling in The Lifecare Hospital Bungoma Catering DepartmentDocument4 pagesIpc and Food Handling in The Lifecare Hospital Bungoma Catering Departmentemma nyongesaNo ratings yet
- Muhlenberg Hospital History TimelineDocument2 pagesMuhlenberg Hospital History TimelineDeborah Joyce DoweNo ratings yet
- DacryocystorhinostomyDocument3 pagesDacryocystorhinostomyNarla SusheelNo ratings yet
- The Tanzania Food, Drugs and Cosmetics Act, 2003Document89 pagesThe Tanzania Food, Drugs and Cosmetics Act, 2003ananthNo ratings yet
- (ENGLISH) Perbandingan Khasiat Cetirizine Dan LoratadinDocument9 pages(ENGLISH) Perbandingan Khasiat Cetirizine Dan Loratadinintan nabilah pratiwiNo ratings yet
- Safety OrganisationDocument16 pagesSafety OrganisationDinesh dhakarNo ratings yet
- Manuskrip Cerobong+Asap LengkapDocument10 pagesManuskrip Cerobong+Asap LengkapRahmad Fahreza SetiawanNo ratings yet
- Weaning From Mechanical Ventilation Using SBT PDFDocument29 pagesWeaning From Mechanical Ventilation Using SBT PDFEdgar Bravo Santibañez100% (1)
- Faith Ezekiel College of Health IdahDocument43 pagesFaith Ezekiel College of Health IdahZedek PeterNo ratings yet
- Startups 8Document2 pagesStartups 8Rafi AzamNo ratings yet
- Chronic Diseases MiasmsDocument143 pagesChronic Diseases MiasmsGajanan R Ghatage100% (3)
- Question NairDocument4 pagesQuestion NairJaisurya SharmaNo ratings yet
- A Review of The Occupational Diseases Reporting System in The Republic of Ireland PDFDocument113 pagesA Review of The Occupational Diseases Reporting System in The Republic of Ireland PDFaymen145771552No ratings yet
- 50 Emergency DrugsDocument70 pages50 Emergency DrugsderizNo ratings yet
- Nursing Theories-1-109-124Document16 pagesNursing Theories-1-109-124putuNo ratings yet
- Term PaperDocument4 pagesTerm PaperIvin KuriakoseNo ratings yet
- KCRHA Five Year Plan MemoDocument23 pagesKCRHA Five Year Plan MemoJeremy HarrisNo ratings yet
- Photography Essay Olivia Livvy MurphyDocument6 pagesPhotography Essay Olivia Livvy Murphyapi-346711892No ratings yet
- First Page PDFDocument1 pageFirst Page PDFEricaNo ratings yet
- Hygiene in Patient Care: Supplementary Resources: Watch The Video ClipsDocument26 pagesHygiene in Patient Care: Supplementary Resources: Watch The Video Clipslee lenaNo ratings yet
- Diageo Marketing Code: Promoting Responsible DrinkingDocument20 pagesDiageo Marketing Code: Promoting Responsible DrinkingZim ZumNo ratings yet
- University of Health Sciences Lahore: Theory Date SheetDocument1 pageUniversity of Health Sciences Lahore: Theory Date SheetNayabNo ratings yet
- SDS ANA Buffer Solution PH 9 21 en 22121512Document9 pagesSDS ANA Buffer Solution PH 9 21 en 22121512haidar baqirNo ratings yet