Download as pdf or txt
You might also like
- Uia UC1901 76146 7Document28 pagesUia UC1901 76146 7That Dude GageNo ratings yet
- Outcome Expectancy and Self-Efficacy Theoretical Implications of An Unresolved ContradictionDocument10 pagesOutcome Expectancy and Self-Efficacy Theoretical Implications of An Unresolved Contradictionashrafzakaria85No ratings yet
- Goldin Et Al 2013 Changes in Positive Self Views Mediate The Effect of Cognitive Behavioral Therapy For Social AnxietyDocument10 pagesGoldin Et Al 2013 Changes in Positive Self Views Mediate The Effect of Cognitive Behavioral Therapy For Social AnxietyIqbal BurhaniNo ratings yet
- ClinicalPsychologicalScience 2013 Goldin 2167702613476867Document11 pagesClinicalPsychologicalScience 2013 Goldin 2167702613476867Elena MathewNo ratings yet
- One-Session Exposure Treatment For Social Anxiety With Specific Fear ofDocument13 pagesOne-Session Exposure Treatment For Social Anxiety With Specific Fear ofcagNo ratings yet
- SCT chapterLuszczynskaSchwarzer2015Document28 pagesSCT chapterLuszczynskaSchwarzer2015Mixcy MabatidNo ratings yet
- Extraversion As A Moderator of The Efficacy of Self-Esteem Maintenance StrategiesDocument15 pagesExtraversion As A Moderator of The Efficacy of Self-Esteem Maintenance StrategiesHusnie Al-mubarok AfandieNo ratings yet
- Acute Stress Reduces Effortful Prosocial BehaviourDocument23 pagesAcute Stress Reduces Effortful Prosocial BehaviourKrishnapriya T SNo ratings yet
- When Every Day Is A High School Reunion: Social Media Comparisons and Self-EsteemDocument23 pagesWhen Every Day Is A High School Reunion: Social Media Comparisons and Self-EsteemLiz SantanaNo ratings yet
- ROL Empty Chair 2Document22 pagesROL Empty Chair 2tbf06720No ratings yet
- Assessing Generalization in Perceived Self-EfficacyDocument9 pagesAssessing Generalization in Perceived Self-EfficacybldzsrnnNo ratings yet
- Recovery From Schizophrenia in Community-Based Psychosocial Rehabilitation Settings Rates and PredictorsDocument15 pagesRecovery From Schizophrenia in Community-Based Psychosocial Rehabilitation Settings Rates and Predictorstitik dyahNo ratings yet
- Research 1Document11 pagesResearch 1Lai BaNo ratings yet
- JurnalDocument17 pagesJurnalHerfanus DuhaNo ratings yet
- RetrieveDocument17 pagesRetrieveMajkaMiaskiewiczNo ratings yet
- Emotional Consequences of Collective Action Participation: Differentiating Self-Directed and Outgroup-Directed EmotionsDocument12 pagesEmotional Consequences of Collective Action Participation: Differentiating Self-Directed and Outgroup-Directed EmotionsFelipeNo ratings yet
- Perceptions of The Therapist in A Virtual World An Exploratory Analog StudyDocument13 pagesPerceptions of The Therapist in A Virtual World An Exploratory Analog StudyDavid Otálvaro Z.No ratings yet
- Asociaciones Concurrentes y Prospectivas Entre Creencias Negativas de Evaluación SocialDocument12 pagesAsociaciones Concurrentes y Prospectivas Entre Creencias Negativas de Evaluación SocialTere OliverosNo ratings yet
- Banduras Social Learning Theoryand Its Importanceinthe Organizational Psychology ContextDocument9 pagesBanduras Social Learning Theoryand Its Importanceinthe Organizational Psychology ContextJuan Carlos Olivo AlonsoNo ratings yet
- NIH Public Access: The Impact of Social Skills Training For Social Anxiety Disorder: A Randomized Controlled TrialDocument29 pagesNIH Public Access: The Impact of Social Skills Training For Social Anxiety Disorder: A Randomized Controlled TrialAnonymous RxjOeoYn9No ratings yet
- Intervencion 2.1.Document12 pagesIntervencion 2.1.Cristina MPNo ratings yet
- Relationships Between Coping Strategies and Burnout Symptoms: A Meta-Analytic ApproachDocument14 pagesRelationships Between Coping Strategies and Burnout Symptoms: A Meta-Analytic ApproachLavinia DamianNo ratings yet
- Research ProposalDocument4 pagesResearch ProposalAntonette Africa MercadoNo ratings yet
- Terenzi Liu Et Al 2021Document12 pagesTerenzi Liu Et Al 2021joshua80No ratings yet
- Implicit Bias Training ImageryDocument14 pagesImplicit Bias Training ImageryEstela MedinaNo ratings yet
- Self-Compassion and Competition in Athlete Mental Health: December 2019Document8 pagesSelf-Compassion and Competition in Athlete Mental Health: December 2019Roxana BejanNo ratings yet
- Imp 2Document6 pagesImp 2juandellibroNo ratings yet
- Problem-Solving Appraisal and Psychological Adjustment: January 2012Document87 pagesProblem-Solving Appraisal and Psychological Adjustment: January 2012Wilson Rafael Cosi ChoqqueNo ratings yet
- Fpsyg 2019 02909Document21 pagesFpsyg 2019 02909Makanudo.No ratings yet
- Social Anxiety and Fear of Causing Discomfort To Others Diagnostic Specificity Symptom Correlates and CBT Treatment OutcomeDocument19 pagesSocial Anxiety and Fear of Causing Discomfort To Others Diagnostic Specificity Symptom Correlates and CBT Treatment OutcomeAdrián Mantero OjedaNo ratings yet
- Jyoti Meditation Article 2016Document16 pagesJyoti Meditation Article 2016Aarohi PatilNo ratings yet
- Busch Et Al. 2018 andDocument10 pagesBusch Et Al. 2018 andsaul fabianoNo ratings yet
- ERQ Study Manuscript ACCEPTEDDocument30 pagesERQ Study Manuscript ACCEPTEDmarcelocarvalhoteacher2373No ratings yet
- Internet Supported Cognitive Behavior Therapy To Help Students With Shy-Socially Isolated ProblemsDocument10 pagesInternet Supported Cognitive Behavior Therapy To Help Students With Shy-Socially Isolated ProblemsTorro AllegroNo ratings yet
- Defusion Vs Cog restructuring-DEacon-2011Document16 pagesDefusion Vs Cog restructuring-DEacon-2011psicgabrielpinedaNo ratings yet
- Chao 2014Document24 pagesChao 2014Adrian BotelloNo ratings yet
- Keeping The Goal in Sight: Testing The Influence of Narrowed Visual Attention On Physical ActivityDocument12 pagesKeeping The Goal in Sight: Testing The Influence of Narrowed Visual Attention On Physical ActivityEddy VedderNo ratings yet
- Kirschner 2019Document21 pagesKirschner 2019Arzaci ArzaciNo ratings yet
- Ehrlich 2015Document13 pagesEhrlich 2015Muhammad HijrilNo ratings yet
- Resonance Performance ModelDocument20 pagesResonance Performance ModelsarahbeeNo ratings yet
- Self-Reflection and Insight Scale (Grant Et Al., 2002)Document17 pagesSelf-Reflection and Insight Scale (Grant Et Al., 2002)Viktorija PetunovaNo ratings yet
- Anti Stigma TaiwanDocument8 pagesAnti Stigma TaiwanLeticia Raquel Pe�a Pe�aNo ratings yet
- Ijirt150094 PaperDocument10 pagesIjirt150094 PaperSruthi GunasekaranNo ratings yet
- Compassion Focused Therapy After Traumatic Brain Injury: Theoretical Foundations and A Case IllustrationDocument13 pagesCompassion Focused Therapy After Traumatic Brain Injury: Theoretical Foundations and A Case IllustrationMiguelySusy Ramos-RojasNo ratings yet
- Psycho-Physiological State Inventory PaperDocument8 pagesPsycho-Physiological State Inventory PaperAmrit Kr MahatoNo ratings yet
- ArticleDocument14 pagesArticleShaa ShaamalaahNo ratings yet
- Research Article The Relationship Between Symptoms and Social Functioning Over The Course of Cognitive Behavioral Therapy For Social Anxiety DisorderDocument7 pagesResearch Article The Relationship Between Symptoms and Social Functioning Over The Course of Cognitive Behavioral Therapy For Social Anxiety DisorderJefry TameNo ratings yet
- Bakker RIckard 2017 Engagementinmobilephoneapp Mood PrismresultsDocument12 pagesBakker RIckard 2017 Engagementinmobilephoneapp Mood PrismresultsHomebbeautyNo ratings yet
- Yusufov 2018 Meta Analytic Evaluation of Stress Reduction Interventions For Undergraduate and Graduate StudentsDocument20 pagesYusufov 2018 Meta Analytic Evaluation of Stress Reduction Interventions For Undergraduate and Graduate Studentsjou jimNo ratings yet
- The Physical Sacrifice of Thinking Investigating The Relationship Between Thinking and Physical Activity in Everyday LifeDocument9 pagesThe Physical Sacrifice of Thinking Investigating The Relationship Between Thinking and Physical Activity in Everyday LifeAndres Mera VergaraNo ratings yet
- Doebel Et Al 2019 Good Things Come To Those Who Wait Delaying Gratification Likely Does Matter For Later Achievement (ADocument3 pagesDoebel Et Al 2019 Good Things Come To Those Who Wait Delaying Gratification Likely Does Matter For Later Achievement (AconstantinabollartiNo ratings yet
- Becker2017 PDFDocument34 pagesBecker2017 PDFMaddY M.No ratings yet
- The Effect of Reappraising Social Exclusion On Emotional DistressDocument12 pagesThe Effect of Reappraising Social Exclusion On Emotional DistressMariel NavarroNo ratings yet
- Vocational Rehabilitation Improves Insight and Social Functioning of People With SchizophreniaDocument1 pageVocational Rehabilitation Improves Insight and Social Functioning of People With SchizophreniaNursulfia MaharaniNo ratings yet
- The Effectiveness of Group Psychotherapy in ReduciDocument13 pagesThe Effectiveness of Group Psychotherapy in ReduciAgnes MontalboNo ratings yet
- Woods Et Al 2018 What Is in A Name A Historical Review of Intelligence Test Score LabelsDocument14 pagesWoods Et Al 2018 What Is in A Name A Historical Review of Intelligence Test Score LabelsQuỳnh Anh LêNo ratings yet
- Psychol Psychother - 2023 - Mackali - The Mediating Role of Self Compassion in The Relationship Between Internalized StigmaDocument15 pagesPsychol Psychother - 2023 - Mackali - The Mediating Role of Self Compassion in The Relationship Between Internalized Stigmajagannatha.ganyaNo ratings yet
- The Process of Empowerment A Model For Use in Research and PracticeDocument15 pagesThe Process of Empowerment A Model For Use in Research and PracticeAnnNo ratings yet
- Jurnal International Wartegg 2Document8 pagesJurnal International Wartegg 2Ilham FauzanNo ratings yet
- Flake Fried 2020 Measurement Schmeasurement Questionable Measurement Practices and How To Avoid ThemDocument10 pagesFlake Fried 2020 Measurement Schmeasurement Questionable Measurement Practices and How To Avoid Themtaolingyi2001No ratings yet
- Brook Comptom Frame Sizes PDFDocument12 pagesBrook Comptom Frame Sizes PDFVictorNo ratings yet
- Catalog HarfitDocument80 pagesCatalog Harfitfajarsanjaya1992No ratings yet
- Publix Coral Springs Inspection ReportDocument5 pagesPublix Coral Springs Inspection ReportAmanda RojasNo ratings yet
- Fire Alarm Systems: Intelligent Detection. Superior ProtectionDocument17 pagesFire Alarm Systems: Intelligent Detection. Superior ProtectionLuiyi Lazcano MontalvoNo ratings yet
- Soal Uas Ganjil SMK XiDocument2 pagesSoal Uas Ganjil SMK Xibondan iskandarNo ratings yet
- Testngo Covid-19 Rapid Antigen Saliva TestDocument18 pagesTestngo Covid-19 Rapid Antigen Saliva Testrachel lowNo ratings yet
- Installation and Use Instructions: PatentedDocument32 pagesInstallation and Use Instructions: PatentedvizanteaNo ratings yet
- Financial Forecasting For Strategic GrowthDocument3 pagesFinancial Forecasting For Strategic GrowthVergel MartinezNo ratings yet
- Personality Disorder Pre-Assessment QuestionnaireDocument16 pagesPersonality Disorder Pre-Assessment QuestionnaireTasos AlbaNo ratings yet
- Trading in Financial MarketsDocument33 pagesTrading in Financial MarketsjlosamNo ratings yet
- Sudarshan Samhita Book inDocument9 pagesSudarshan Samhita Book inAnonymous CJ89xIx70% (3)
- Perlindungan Hukum Bagi Profesi Perawat Terhadap Pelaksanaan Praktik KeperawatanDocument5 pagesPerlindungan Hukum Bagi Profesi Perawat Terhadap Pelaksanaan Praktik KeperawatanALWIN WinNo ratings yet
- A-Dec 300, 400, and 500 Product Families Installation ChecklistDocument2 pagesA-Dec 300, 400, and 500 Product Families Installation ChecklistIliasNo ratings yet
- Mynn 11-2020Document23 pagesMynn 11-2020Tweed3ANo ratings yet
- Bosch Washing Machine BrochureDocument6 pagesBosch Washing Machine BrochurePrasad DNo ratings yet
- DPPM UNIT2 Disaster and Vulnerability ProfileDocument57 pagesDPPM UNIT2 Disaster and Vulnerability ProfileVamshi TangelapallyNo ratings yet
- CMC8458 Cablecraft Products Catalog Final No Crop MarksDocument84 pagesCMC8458 Cablecraft Products Catalog Final No Crop MarksvikeshmNo ratings yet
- Spherical TankDocument30 pagesSpherical TankNuzuliana EnuzNo ratings yet
- Incidence & Types of Mos in Food: Chapter ThreeDocument21 pagesIncidence & Types of Mos in Food: Chapter ThreeReta megersaNo ratings yet
- Batteries PresentationDocument24 pagesBatteries PresentationGajendraPatelNo ratings yet
- Steam TableDocument3 pagesSteam TableMUHAMAD SAUKINo ratings yet
- Pickerlaza: A Website On Iot Based Garbage Collection SystemDocument20 pagesPickerlaza: A Website On Iot Based Garbage Collection SystemBeckyNo ratings yet
- Language Development ActivitiesDocument25 pagesLanguage Development ActivitiesMarc WilfordNo ratings yet
- Lesson Redoxreactiontitration Student LabDocument5 pagesLesson Redoxreactiontitration Student LabThành Huỳnh QuanNo ratings yet
- 3 IdiotsDocument1 page3 IdiotsVic SherNo ratings yet
- A Guide To Biological Buffer Preparation: For Weighing, PH Measurement and PipettingDocument20 pagesA Guide To Biological Buffer Preparation: For Weighing, PH Measurement and PipettingWagner ProchnowNo ratings yet
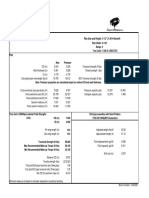
- 5.5 In. 21.90# IEU S-135 R2 XT55 (7.0 X 4.0) - 10P.15BDocument3 pages5.5 In. 21.90# IEU S-135 R2 XT55 (7.0 X 4.0) - 10P.15BJohnNo ratings yet
- West Coast Cannabis Magazine-January-10Document49 pagesWest Coast Cannabis Magazine-January-10murciano207No ratings yet
- Philips Wireless Phone Jack Model PH0900 (PX211 D Rev 2.2)Document29 pagesPhilips Wireless Phone Jack Model PH0900 (PX211 D Rev 2.2)chapicab6211No ratings yet