Download as pdf or txt
You might also like
- Analyzing The PV92 Locus On Chromosome 16 For The Alu Insertion Through The Polymerase Chain Reaction and Agarose Gel ElectrophoresisDocument10 pagesAnalyzing The PV92 Locus On Chromosome 16 For The Alu Insertion Through The Polymerase Chain Reaction and Agarose Gel ElectrophoresisJohansen C. Pico100% (1)
- Molecular Pathology of Hematolymphoid Diseases - C. Dunphy (Springer, 2010) WW PDFDocument613 pagesMolecular Pathology of Hematolymphoid Diseases - C. Dunphy (Springer, 2010) WW PDFMoldovan Tiberiu100% (2)
- Millipore UF Catalog PDFDocument100 pagesMillipore UF Catalog PDFShawkatNo ratings yet
- P.03 Cell Adaptation Cell Injury and Cell Death Part 2 08 09 2017Document4 pagesP.03 Cell Adaptation Cell Injury and Cell Death Part 2 08 09 2017PAUL ALINGKAYONNo ratings yet
- DR Divesh Mishra's Pathology NotesDocument12 pagesDR Divesh Mishra's Pathology NotesSanchit PathakNo ratings yet
- Pathology FDocument42 pagesPathology FAryan SahNo ratings yet
- I. Cellular Adaptations:: Cellular Injury, Cell Adaptation & Cell Death 1. Hyperplasia 3. AtrophyDocument4 pagesI. Cellular Adaptations:: Cellular Injury, Cell Adaptation & Cell Death 1. Hyperplasia 3. AtrophyShuaib SiddiquiNo ratings yet
- Histopathology - Lec Prelim 1Document43 pagesHistopathology - Lec Prelim 1Jean Calubag CatalanNo ratings yet
- Anatomy and PhysiologyDocument7 pagesAnatomy and PhysiologyWeng WengNo ratings yet
- Histopathology NotesDocument12 pagesHistopathology NotesLeandro Miguel TongolNo ratings yet
- Cell Adaptation & Response To Injury by NikitaDocument3 pagesCell Adaptation & Response To Injury by NikitaMedical Student NotesNo ratings yet
- Bentuk-Bentuk Adaptasi Terhadap Stress Lingkungan 2014 - HIPOFUNGSIDocument32 pagesBentuk-Bentuk Adaptasi Terhadap Stress Lingkungan 2014 - HIPOFUNGSImisswilnaanggunNo ratings yet
- General Pathology Supertrans Block 1Document10 pagesGeneral Pathology Supertrans Block 1Mavic VillanuevaNo ratings yet
- CellularAdaptation Injury and Death - General OverviewDocument13 pagesCellularAdaptation Injury and Death - General OverviewlydNo ratings yet
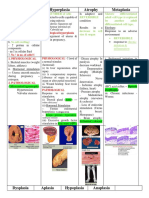
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument20 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Physiology of The BloodDocument16 pagesPhysiology of The BlooddiytNo ratings yet
- Dist of Growth 1 2023 LectureDocument60 pagesDist of Growth 1 2023 LecturejaidenrmNo ratings yet
- NRS Review Notes - CancerDocument20 pagesNRS Review Notes - CancerMariecar GarazaNo ratings yet
- Difference BLN Hypertropy &atropyDocument2 pagesDifference BLN Hypertropy &atropyFu'e AbdumalikNo ratings yet
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocument24 pagesHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanNo ratings yet
- Male ReproductionDocument3 pagesMale Reproductionmelly nazwa juwitaNo ratings yet
- Placenta Previa Case StudyDocument7 pagesPlacenta Previa Case StudyKing NavsunNo ratings yet
- BiochemistryDocument65 pagesBiochemistryjosue gomezNo ratings yet
- BiochemistryDocument81 pagesBiochemistryGlorivy E. Mora GonzalezNo ratings yet
- Cellular Adaptation - 2022Document49 pagesCellular Adaptation - 2022Leo Lucifer 104No ratings yet
- Hematology ReviewerDocument4 pagesHematology ReviewerAbigail Puno100% (1)
- 02 Gestational Trophoblastic DiseaseDocument8 pages02 Gestational Trophoblastic Diseasemisakichan FrandoNo ratings yet
- BLOOD TransesDocument7 pagesBLOOD TransesBianca Paulyn CastilloNo ratings yet
- First Aid 2015 Pages AddedDocument11 pagesFirst Aid 2015 Pages AddedNicole WilliamNo ratings yet
- Anemia - SFFTDocument5 pagesAnemia - SFFTShikha UpadhyayNo ratings yet
- Chapter 1 Cell InjuryDocument21 pagesChapter 1 Cell Injuryhenna patelNo ratings yet
- Cell Injury - Part 1Document58 pagesCell Injury - Part 1Mirleyka GonzálezNo ratings yet
- 1 Cellular Response To Injury 1Document33 pages1 Cellular Response To Injury 1Alex XanderNo ratings yet
- FM1 Pathology - FULLDocument85 pagesFM1 Pathology - FULLMFC 2019No ratings yet
- FM1 Pathology - FULLDocument85 pagesFM1 Pathology - FULLMFC 2019No ratings yet
- BIOLOGY Answer Key English Medium SSLC March 2019 by A+ EducareDocument5 pagesBIOLOGY Answer Key English Medium SSLC March 2019 by A+ EducarehadiyxxNo ratings yet
- Introduction & VomitingDocument47 pagesIntroduction & VomitingSyarifah FauziahNo ratings yet
- AfsfasDocument5 pagesAfsfasPaul Stephen SorianoNo ratings yet
- ZON HematopoyesisDocument16 pagesZON HematopoyesisMariana CabagnaNo ratings yet
- The Metabolic and Endocrine Systems NotesDocument9 pagesThe Metabolic and Endocrine Systems NotesCarl Elexer Cuyugan Ano100% (2)
- Weakness (Approach To Diagnosis) - Dr. TulmoDocument2 pagesWeakness (Approach To Diagnosis) - Dr. TulmoMonique BorresNo ratings yet
- Prelim Anaphy 1Document4 pagesPrelim Anaphy 1Sav OliNo ratings yet
- Patho Supplement Handout For Sept 2018 UPDATED May 2018 PDFDocument25 pagesPatho Supplement Handout For Sept 2018 UPDATED May 2018 PDFemely p. tango100% (1)
- TOPNOTCH Patho Supplement Handout For Sept 2018 UPDATED May 2018Document25 pagesTOPNOTCH Patho Supplement Handout For Sept 2018 UPDATED May 2018Waiwit KritayakiranaNo ratings yet
- The Metabolic and Endocrine Systems NotesDocument15 pagesThe Metabolic and Endocrine Systems Notesrozelle28No ratings yet
- Krok 1 Physiology 19Document1 pageKrok 1 Physiology 19Sandeep KumarNo ratings yet
- Cell Injury & AdaptationDocument22 pagesCell Injury & AdaptationUmam LoyalNo ratings yet
- Endo ReviewerDocument5 pagesEndo ReviewerZIAN LABADIANo ratings yet
- 5.1 PPT ANEMIADocument29 pages5.1 PPT ANEMIAResta SeptiaNo ratings yet
- Cellular Pathology: Normal CellsDocument22 pagesCellular Pathology: Normal CellsPrakash PanthiNo ratings yet
- Cellular Pathology: Normal CellsDocument20 pagesCellular Pathology: Normal CellsRHONENo ratings yet
- Newborn ScreeningDocument6 pagesNewborn ScreeningFatimah Maimana SolaimanNo ratings yet
- Approach To A Floppy ChildDocument3 pagesApproach To A Floppy ChildTaimur KhalilNo ratings yet
- PATH 1 ALL Lectures Final1Document2,054 pagesPATH 1 ALL Lectures Final1Andleeb Imran100% (1)
- Wilm's Tumor EtcDocument5 pagesWilm's Tumor EtcDanica BonNo ratings yet
- Emergencies in Pediatric Surgery: DR Irene Lokananta SpbaDocument16 pagesEmergencies in Pediatric Surgery: DR Irene Lokananta SpbaGoldwin AdithyaNo ratings yet
- Intro Patho (Dr. Apao)Document82 pagesIntro Patho (Dr. Apao)Kristine Josephine D. BusaNo ratings yet
- 1 HematopoiesisDocument8 pages1 HematopoiesisAndra BauerNo ratings yet
- Hematological Disorders ErythropoiesisDocument4 pagesHematological Disorders Erythropoiesis3S - JOCSON, DENESE NICOLE LEE M.No ratings yet
- Pathology Notes 2009Document137 pagesPathology Notes 2009KelvinTMaikanaNo ratings yet
- Cedera Sel Dan Adaptasi (Residen)Document77 pagesCedera Sel Dan Adaptasi (Residen)jujuNo ratings yet
- Human Brain Evolution: The Influence of Freshwater and Marine Food ResourcesFrom EverandHuman Brain Evolution: The Influence of Freshwater and Marine Food ResourcesStephen CunnaneRating: 4 out of 5 stars4/5 (1)
- Organisation of Eukaryotic ChromosomesDocument48 pagesOrganisation of Eukaryotic Chromosomesstevensb05591% (23)
- Post It Note Science DNA Replication, Transcription and Translation Mini.1.Kreitzer-houslerDocument4 pagesPost It Note Science DNA Replication, Transcription and Translation Mini.1.Kreitzer-houslerCHRISTEROP0% (1)
- MitochondriaDocument32 pagesMitochondriaDayana Prasanth100% (1)
- UNIT I Gen Bio ReviewerDocument4 pagesUNIT I Gen Bio ReviewerKym DacudaoNo ratings yet
- Application of Electrophoresis Techniques in Forensic ScienceDocument2 pagesApplication of Electrophoresis Techniques in Forensic ScienceNaeem MalikNo ratings yet
- Diet Mediterania Kontrol Kadar Glukosa Darah Pada Diabetes Melitus Tipe 2Document6 pagesDiet Mediterania Kontrol Kadar Glukosa Darah Pada Diabetes Melitus Tipe 2krisnaNo ratings yet
- 12 2 PWPT PDFDocument24 pages12 2 PWPT PDFapi-262378640No ratings yet
- Bioprocessbrochure PDFDocument16 pagesBioprocessbrochure PDFViesta SampeNo ratings yet
- DNA StructureDocument38 pagesDNA Structuremuhdmoosa100% (3)
- ExamDocument27 pagesExamKashish HoraNo ratings yet
- Recombinant DNA MCQDocument6 pagesRecombinant DNA MCQChaze WaldenNo ratings yet
- BR574 0915 xMAP Cookbook 3rdedition WR PDFDocument148 pagesBR574 0915 xMAP Cookbook 3rdedition WR PDFNiranjan BhuvanaratnamNo ratings yet
- Chapter 2 Form 5 ScienceDocument4 pagesChapter 2 Form 5 ScienceZainurain Zainal AbidinNo ratings yet
- Practical 33 PDFDocument4 pagesPractical 33 PDFPriyanka RamNo ratings yet
- 499-Article Text-706-1-10-20220526-MutoniDocument8 pages499-Article Text-706-1-10-20220526-MutoniChristine MutoniNo ratings yet
- Cot CurveDocument16 pagesCot CurveVidyasagar Deshpande100% (1)
- Chapter 6 FuelingDocument5 pagesChapter 6 FuelingRossi100% (1)
- TimelineDocument2 pagesTimelineapi-282582740No ratings yet
- Processing of Vitamin b12Document16 pagesProcessing of Vitamin b12TANSIEWYENNo ratings yet
- CellsDocument19 pagesCellsAulia Safri NahriyahNo ratings yet
- Second Quarter Exam in General Biology IDocument5 pagesSecond Quarter Exam in General Biology IAubrey SalidoNo ratings yet
- sc1c02627 Si 001Document16 pagessc1c02627 Si 001Maii MohammedNo ratings yet
- Plant Metabolomics Standards MS DataDocument56 pagesPlant Metabolomics Standards MS DataansoletNo ratings yet
- Lse 05Document26 pagesLse 05Anjali MunjalNo ratings yet
- Week 2 Study GuideDocument7 pagesWeek 2 Study GuideSAVORY SITHNo ratings yet
- Ex - No. Genomic DNA Isolation From Fish Fins Using Phenol-Chloroform MethodDocument2 pagesEx - No. Genomic DNA Isolation From Fish Fins Using Phenol-Chloroform MethodmercyaugustinNo ratings yet
- CBSE Class 12 Biology Question Paper Solution 2010 Set 1Document8 pagesCBSE Class 12 Biology Question Paper Solution 2010 Set 1Bhavya PatelNo ratings yet