
Fluids and Electrolytes
Fluids and Electrolytes
You might also like
- Preclinical Physiology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Physiology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Rating: 1 out of 5 stars1/5 (1)
- Nursing Fluids and ElectrolytesDocument14 pagesNursing Fluids and Electrolytesaga1028100% (18)
- Case Scenario For Community Health NursingDocument5 pagesCase Scenario For Community Health Nursinghemihema100% (1)
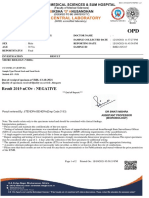
- Patient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusDocument2 pagesPatient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusThushar P kumarNo ratings yet
- 3.14 Chapter 3 Water and Electrolytes Balance and ImblanceDocument140 pages3.14 Chapter 3 Water and Electrolytes Balance and ImblanceShourav SarkarNo ratings yet
- The Water Prescription: For Health, Vitality, and RejuvenationFrom EverandThe Water Prescription: For Health, Vitality, and RejuvenationRating: 5 out of 5 stars5/5 (2)
- Tramadol Vancomycin Drug StudyDocument6 pagesTramadol Vancomycin Drug StudyAllene PaderangaNo ratings yet
- Occupational Health in Aviation PDFDocument235 pagesOccupational Health in Aviation PDFabhayNo ratings yet
- Blood InvestigationDocument70 pagesBlood InvestigationRohit RaiNo ratings yet
- Colour My WordsDocument194 pagesColour My WordsEleanor MaclureNo ratings yet
- Fluid Volume BalanceDocument73 pagesFluid Volume BalanceSalman HabeebNo ratings yet
- Basic of Fluid Therapy ImaDocument69 pagesBasic of Fluid Therapy Imal Made ArtawanNo ratings yet
- Fluid and Electrolyte Management of The Surgical PatientDocument28 pagesFluid and Electrolyte Management of The Surgical PatientAndri Feisal NasutionNo ratings yet
- Fluids and Electrolytes-2Document82 pagesFluids and Electrolytes-2Jem Loterte100% (1)
- HEALTH SCI 12 - ANAPHY - Chapter - 27Document11 pagesHEALTH SCI 12 - ANAPHY - Chapter - 27Kyla Marie BadanaNo ratings yet
- Physiology, Body Fluids - StatPearls - NCBI BookshelfDocument5 pagesPhysiology, Body Fluids - StatPearls - NCBI Bookshelfpilar gabriela hernandez fernandezNo ratings yet
- Chapter 17 Fluid Electrolytes and Acid-BDocument23 pagesChapter 17 Fluid Electrolytes and Acid-BKayan L.No ratings yet
- Fluid, Electrolyte, and Acid-Base BalanceDocument41 pagesFluid, Electrolyte, and Acid-Base BalanceRn nadeenNo ratings yet
- 11 - Fluid and ElectrolitesDocument46 pages11 - Fluid and ElectrolitesSelin SakarNo ratings yet
- Fluids and Electrolytes: Epidemiology/PathophysiologyDocument27 pagesFluids and Electrolytes: Epidemiology/PathophysiologyManna YankiNo ratings yet
- DwsDocument27 pagesDwsKunni MardhiyahNo ratings yet
- Metabolisme AirDocument15 pagesMetabolisme AirKlara SintaNo ratings yet
- Fluid and Electrolytes Lecture NotesDocument85 pagesFluid and Electrolytes Lecture NotesVince Peliño De MesaNo ratings yet
- Fluid and Electrolyte Imbalance PDFDocument21 pagesFluid and Electrolyte Imbalance PDFShafaq AlamNo ratings yet
- Fluids and Electrolytes NCM 101Document142 pagesFluids and Electrolytes NCM 101France John Evangelista Torres100% (2)
- Metabolisme AirDocument15 pagesMetabolisme AirAyu FadhilahNo ratings yet
- Fluid Electrolyte BalanceDocument19 pagesFluid Electrolyte BalanceRatna VimalNo ratings yet
- Medical Surgical Nursing: Fluids and ElectrolytesDocument28 pagesMedical Surgical Nursing: Fluids and ElectrolytesDhen MarcNo ratings yet
- Emergency Fluid TherapyDocument7 pagesEmergency Fluid TherapyAnaNo ratings yet
- Fluids and ElectrolytesDocument8 pagesFluids and ElectrolytesDEWINo ratings yet
- Water MetabolismDocument3 pagesWater MetabolismJuber mansuriNo ratings yet
- Lect 02Document5 pagesLect 02Iptysam Al-AlawiNo ratings yet
- Fluids and ElectrolytesDocument71 pagesFluids and ElectrolytesHarold Castillo OrigenesNo ratings yet
- Fluids and ElectrolytesDocument9 pagesFluids and ElectrolytesaclumutNo ratings yet
- The Body Fluid CompartmentsDocument6 pagesThe Body Fluid CompartmentsAlya Putri KhairaniNo ratings yet
- Part 1 - Fluid and Electrolyte Balance, Nursing Process, Fluid ImbalancesDocument23 pagesPart 1 - Fluid and Electrolyte Balance, Nursing Process, Fluid Imbalancesfebie pacheco100% (1)
- Fluid Electrolyte and AcidBase BalanceDocument33 pagesFluid Electrolyte and AcidBase Balancemoncalshareen3No ratings yet
- NUR108 2014 Student (1) .PPTX 1Document129 pagesNUR108 2014 Student (1) .PPTX 1LLLJJJ100% (1)
- Fluids and ElectrolytesDocument79 pagesFluids and ElectrolytesReignallienn Inocencio MartinNo ratings yet
- F & E Study Guide - SY 2022-2023Document16 pagesF & E Study Guide - SY 2022-20232A - Nicole Marrie HonradoNo ratings yet
- CH 25 of GuytonDocument7 pagesCH 25 of GuytonBea Samonte100% (2)
- Fluid and Electrolyte BalanceDocument295 pagesFluid and Electrolyte BalanceAnuchithra RadhakrishnanNo ratings yet
- ACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idDocument14 pagesACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idCenitserNo ratings yet
- Fluid and ElectrolytesDocument137 pagesFluid and ElectrolytesNano Baddour100% (1)
- 19 Fluid and Electrolyte Imbalance and Nutritional ProblemDocument40 pages19 Fluid and Electrolyte Imbalance and Nutritional ProblemPaul EbenezerNo ratings yet
- 3 Fluid and ElectrolyteDocument7 pages3 Fluid and ElectrolyteStephen HDNo ratings yet
- Fluid and Electrolyte BalanceDocument87 pagesFluid and Electrolyte Balancerajashree kokatanurNo ratings yet
- Fluids and ElectrolytesDocument9 pagesFluids and ElectrolytesCoy EnNo ratings yet
- Cairan Dan ElektrolitDocument11 pagesCairan Dan ElektrolitYuanitaipNo ratings yet
- Hyponatremia Dan HypernatremiaDocument25 pagesHyponatremia Dan HypernatremiaramithadNo ratings yet
- Australian Naturopathic Network: Departments Medical Sciences A&P FluidDocument4 pagesAustralian Naturopathic Network: Departments Medical Sciences A&P FluidFathur Rahman Mutiara HikmahNo ratings yet
- Electrolytes: Regulation of Body Fluid CompartmentsDocument6 pagesElectrolytes: Regulation of Body Fluid Compartmentsbuhari rabiuNo ratings yet
- Pathophysiology Module 4Document26 pagesPathophysiology Module 4johnbryanmalonesNo ratings yet
- Fluids Electrolytes NotesDocument23 pagesFluids Electrolytes NotesHamza AdriNo ratings yet
- Fluid & Electrolyte Balance: Part 4: Regulation & MaintenanceDocument40 pagesFluid & Electrolyte Balance: Part 4: Regulation & MaintenanceMy MusicNo ratings yet
- NCM 112 Fluids & Electrolytes Quiz AssignmentDocument4 pagesNCM 112 Fluids & Electrolytes Quiz AssignmentJoyce Kathreen Ebio LopezNo ratings yet
- Fluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceFrom EverandFluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceRating: 5 out of 5 stars5/5 (2)
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledFrom EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo ratings yet
- Lymph Health: The Key to a Strong Immune SystemFrom EverandLymph Health: The Key to a Strong Immune SystemRating: 5 out of 5 stars5/5 (1)
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentFrom EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiNo ratings yet
- The Ripple Effect Unraveling The Psychology of Social ResponsibilityFrom EverandThe Ripple Effect Unraveling The Psychology of Social ResponsibilityNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- AGD PPT HermantoDocument33 pagesAGD PPT HermantoWahyu Permata LisaNo ratings yet
- Cerebral Palsy: An Overview: The Centers For Disease ControlDocument8 pagesCerebral Palsy: An Overview: The Centers For Disease ControlAlma PradiftaNo ratings yet
- Benign Gynecologic LesionsDocument103 pagesBenign Gynecologic Lesions201286% (7)
- Hing Asafoetida Medicinal UsesDocument5 pagesHing Asafoetida Medicinal UseshemanthbolemNo ratings yet
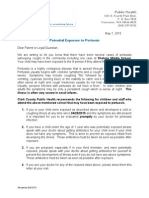
- Whooping Cough Letter Shahala Middle SchoolDocument2 pagesWhooping Cough Letter Shahala Middle SchoolKGW NewsNo ratings yet
- Telomeres and AgingDocument3 pagesTelomeres and AgingApple Jack100% (1)
- Complications of 3rd Molar SurgeryDocument12 pagesComplications of 3rd Molar Surgeryhamad_kayani_774954No ratings yet
- Anatomy MCQ SBA eMRCSDocument121 pagesAnatomy MCQ SBA eMRCSTowhid HasanNo ratings yet
- Colds: What Is A Cold?Document2 pagesColds: What Is A Cold?Mocha BorgsNo ratings yet
- SEMINAR - 7 (Pharmacoepidemilogy)Document69 pagesSEMINAR - 7 (Pharmacoepidemilogy)LathaVijendraNo ratings yet
- Management of Neoplastic Pericardial EffusionsDocument4 pagesManagement of Neoplastic Pericardial EffusionsMamamia DonchanNo ratings yet
- 125409orig1s113 PDFDocument268 pages125409orig1s113 PDFKarl SaganNo ratings yet
- Syok Kardiogenik E.C. Sindrom Koroner Akut: Dr. Sarah QonitahDocument43 pagesSyok Kardiogenik E.C. Sindrom Koroner Akut: Dr. Sarah QonitahAnti TjahyaNo ratings yet
- OilsDocument67 pagesOilsNatural2NaturalNo ratings yet
- Bronchial Asthma QuestionsDocument44 pagesBronchial Asthma QuestionsguevarrajanelleruthNo ratings yet
- Mycobacterium SpeciesDocument13 pagesMycobacterium SpeciesSakshi SangleNo ratings yet
- Vein of Galen MalformationDocument69 pagesVein of Galen MalformationBhupendra GuptaNo ratings yet
- The Students' ProblemDocument21 pagesThe Students' ProblemAmairaNo ratings yet
- Medipoint Hospital, AundhDocument26 pagesMedipoint Hospital, AundhVivek SinghNo ratings yet
- An Introduction To Cognitive Psychology Processes and Disorders 3Rd Edition Full ChapterDocument41 pagesAn Introduction To Cognitive Psychology Processes and Disorders 3Rd Edition Full Chapterjohn.hill578100% (21)
- Perlis CRF Renal ReplacementDocument65 pagesPerlis CRF Renal ReplacementFikri SeptianNo ratings yet
- GRADE HandbookDocument75 pagesGRADE HandbookEzequiel ZacañinoNo ratings yet
- 2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishDocument169 pages2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishMuhammad UmairNo ratings yet
- 5096 s07 Ms 2Document7 pages5096 s07 Ms 2mstudy1234560% (1)
























































































Download as pdf or txt
You might also like
- Preclinical Physiology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Physiology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Rating: 1 out of 5 stars1/5 (1)
- Nursing Fluids and ElectrolytesDocument14 pagesNursing Fluids and Electrolytesaga1028100% (18)
- Case Scenario For Community Health NursingDocument5 pagesCase Scenario For Community Health Nursinghemihema100% (1)
- Patient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusDocument2 pagesPatient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusThushar P kumarNo ratings yet
- 3.14 Chapter 3 Water and Electrolytes Balance and ImblanceDocument140 pages3.14 Chapter 3 Water and Electrolytes Balance and ImblanceShourav SarkarNo ratings yet
- The Water Prescription: For Health, Vitality, and RejuvenationFrom EverandThe Water Prescription: For Health, Vitality, and RejuvenationRating: 5 out of 5 stars5/5 (2)
- Tramadol Vancomycin Drug StudyDocument6 pagesTramadol Vancomycin Drug StudyAllene PaderangaNo ratings yet
- Occupational Health in Aviation PDFDocument235 pagesOccupational Health in Aviation PDFabhayNo ratings yet
- Blood InvestigationDocument70 pagesBlood InvestigationRohit RaiNo ratings yet
- Colour My WordsDocument194 pagesColour My WordsEleanor MaclureNo ratings yet
- Fluid Volume BalanceDocument73 pagesFluid Volume BalanceSalman HabeebNo ratings yet
- Basic of Fluid Therapy ImaDocument69 pagesBasic of Fluid Therapy Imal Made ArtawanNo ratings yet
- Fluid and Electrolyte Management of The Surgical PatientDocument28 pagesFluid and Electrolyte Management of The Surgical PatientAndri Feisal NasutionNo ratings yet
- Fluids and Electrolytes-2Document82 pagesFluids and Electrolytes-2Jem Loterte100% (1)
- HEALTH SCI 12 - ANAPHY - Chapter - 27Document11 pagesHEALTH SCI 12 - ANAPHY - Chapter - 27Kyla Marie BadanaNo ratings yet
- Physiology, Body Fluids - StatPearls - NCBI BookshelfDocument5 pagesPhysiology, Body Fluids - StatPearls - NCBI Bookshelfpilar gabriela hernandez fernandezNo ratings yet
- Chapter 17 Fluid Electrolytes and Acid-BDocument23 pagesChapter 17 Fluid Electrolytes and Acid-BKayan L.No ratings yet
- Fluid, Electrolyte, and Acid-Base BalanceDocument41 pagesFluid, Electrolyte, and Acid-Base BalanceRn nadeenNo ratings yet
- 11 - Fluid and ElectrolitesDocument46 pages11 - Fluid and ElectrolitesSelin SakarNo ratings yet
- Fluids and Electrolytes: Epidemiology/PathophysiologyDocument27 pagesFluids and Electrolytes: Epidemiology/PathophysiologyManna YankiNo ratings yet
- DwsDocument27 pagesDwsKunni MardhiyahNo ratings yet
- Metabolisme AirDocument15 pagesMetabolisme AirKlara SintaNo ratings yet
- Fluid and Electrolytes Lecture NotesDocument85 pagesFluid and Electrolytes Lecture NotesVince Peliño De MesaNo ratings yet
- Fluid and Electrolyte Imbalance PDFDocument21 pagesFluid and Electrolyte Imbalance PDFShafaq AlamNo ratings yet
- Fluids and Electrolytes NCM 101Document142 pagesFluids and Electrolytes NCM 101France John Evangelista Torres100% (2)
- Metabolisme AirDocument15 pagesMetabolisme AirAyu FadhilahNo ratings yet
- Fluid Electrolyte BalanceDocument19 pagesFluid Electrolyte BalanceRatna VimalNo ratings yet
- Medical Surgical Nursing: Fluids and ElectrolytesDocument28 pagesMedical Surgical Nursing: Fluids and ElectrolytesDhen MarcNo ratings yet
- Emergency Fluid TherapyDocument7 pagesEmergency Fluid TherapyAnaNo ratings yet
- Fluids and ElectrolytesDocument8 pagesFluids and ElectrolytesDEWINo ratings yet
- Water MetabolismDocument3 pagesWater MetabolismJuber mansuriNo ratings yet
- Lect 02Document5 pagesLect 02Iptysam Al-AlawiNo ratings yet
- Fluids and ElectrolytesDocument71 pagesFluids and ElectrolytesHarold Castillo OrigenesNo ratings yet
- Fluids and ElectrolytesDocument9 pagesFluids and ElectrolytesaclumutNo ratings yet
- The Body Fluid CompartmentsDocument6 pagesThe Body Fluid CompartmentsAlya Putri KhairaniNo ratings yet
- Part 1 - Fluid and Electrolyte Balance, Nursing Process, Fluid ImbalancesDocument23 pagesPart 1 - Fluid and Electrolyte Balance, Nursing Process, Fluid Imbalancesfebie pacheco100% (1)
- Fluid Electrolyte and AcidBase BalanceDocument33 pagesFluid Electrolyte and AcidBase Balancemoncalshareen3No ratings yet
- NUR108 2014 Student (1) .PPTX 1Document129 pagesNUR108 2014 Student (1) .PPTX 1LLLJJJ100% (1)
- Fluids and ElectrolytesDocument79 pagesFluids and ElectrolytesReignallienn Inocencio MartinNo ratings yet
- F & E Study Guide - SY 2022-2023Document16 pagesF & E Study Guide - SY 2022-20232A - Nicole Marrie HonradoNo ratings yet
- CH 25 of GuytonDocument7 pagesCH 25 of GuytonBea Samonte100% (2)
- Fluid and Electrolyte BalanceDocument295 pagesFluid and Electrolyte BalanceAnuchithra RadhakrishnanNo ratings yet
- ACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idDocument14 pagesACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idCenitserNo ratings yet
- Fluid and ElectrolytesDocument137 pagesFluid and ElectrolytesNano Baddour100% (1)
- 19 Fluid and Electrolyte Imbalance and Nutritional ProblemDocument40 pages19 Fluid and Electrolyte Imbalance and Nutritional ProblemPaul EbenezerNo ratings yet
- 3 Fluid and ElectrolyteDocument7 pages3 Fluid and ElectrolyteStephen HDNo ratings yet
- Fluid and Electrolyte BalanceDocument87 pagesFluid and Electrolyte Balancerajashree kokatanurNo ratings yet
- Fluids and ElectrolytesDocument9 pagesFluids and ElectrolytesCoy EnNo ratings yet
- Cairan Dan ElektrolitDocument11 pagesCairan Dan ElektrolitYuanitaipNo ratings yet
- Hyponatremia Dan HypernatremiaDocument25 pagesHyponatremia Dan HypernatremiaramithadNo ratings yet
- Australian Naturopathic Network: Departments Medical Sciences A&P FluidDocument4 pagesAustralian Naturopathic Network: Departments Medical Sciences A&P FluidFathur Rahman Mutiara HikmahNo ratings yet
- Electrolytes: Regulation of Body Fluid CompartmentsDocument6 pagesElectrolytes: Regulation of Body Fluid Compartmentsbuhari rabiuNo ratings yet
- Pathophysiology Module 4Document26 pagesPathophysiology Module 4johnbryanmalonesNo ratings yet
- Fluids Electrolytes NotesDocument23 pagesFluids Electrolytes NotesHamza AdriNo ratings yet
- Fluid & Electrolyte Balance: Part 4: Regulation & MaintenanceDocument40 pagesFluid & Electrolyte Balance: Part 4: Regulation & MaintenanceMy MusicNo ratings yet
- NCM 112 Fluids & Electrolytes Quiz AssignmentDocument4 pagesNCM 112 Fluids & Electrolytes Quiz AssignmentJoyce Kathreen Ebio LopezNo ratings yet
- Fluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceFrom EverandFluids and Electrolytes: An Easy and Intuitive Way to Understand and Memorize Fluids, Electrolytes, and Acidic-Base BalanceRating: 5 out of 5 stars5/5 (2)
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledFrom EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo ratings yet
- Lymph Health: The Key to a Strong Immune SystemFrom EverandLymph Health: The Key to a Strong Immune SystemRating: 5 out of 5 stars5/5 (1)
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentFrom EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiNo ratings yet
- The Ripple Effect Unraveling The Psychology of Social ResponsibilityFrom EverandThe Ripple Effect Unraveling The Psychology of Social ResponsibilityNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- AGD PPT HermantoDocument33 pagesAGD PPT HermantoWahyu Permata LisaNo ratings yet
- Cerebral Palsy: An Overview: The Centers For Disease ControlDocument8 pagesCerebral Palsy: An Overview: The Centers For Disease ControlAlma PradiftaNo ratings yet
- Benign Gynecologic LesionsDocument103 pagesBenign Gynecologic Lesions201286% (7)
- Hing Asafoetida Medicinal UsesDocument5 pagesHing Asafoetida Medicinal UseshemanthbolemNo ratings yet
- Whooping Cough Letter Shahala Middle SchoolDocument2 pagesWhooping Cough Letter Shahala Middle SchoolKGW NewsNo ratings yet
- Telomeres and AgingDocument3 pagesTelomeres and AgingApple Jack100% (1)
- Complications of 3rd Molar SurgeryDocument12 pagesComplications of 3rd Molar Surgeryhamad_kayani_774954No ratings yet
- Anatomy MCQ SBA eMRCSDocument121 pagesAnatomy MCQ SBA eMRCSTowhid HasanNo ratings yet
- Colds: What Is A Cold?Document2 pagesColds: What Is A Cold?Mocha BorgsNo ratings yet
- SEMINAR - 7 (Pharmacoepidemilogy)Document69 pagesSEMINAR - 7 (Pharmacoepidemilogy)LathaVijendraNo ratings yet
- Management of Neoplastic Pericardial EffusionsDocument4 pagesManagement of Neoplastic Pericardial EffusionsMamamia DonchanNo ratings yet
- 125409orig1s113 PDFDocument268 pages125409orig1s113 PDFKarl SaganNo ratings yet
- Syok Kardiogenik E.C. Sindrom Koroner Akut: Dr. Sarah QonitahDocument43 pagesSyok Kardiogenik E.C. Sindrom Koroner Akut: Dr. Sarah QonitahAnti TjahyaNo ratings yet
- OilsDocument67 pagesOilsNatural2NaturalNo ratings yet
- Bronchial Asthma QuestionsDocument44 pagesBronchial Asthma QuestionsguevarrajanelleruthNo ratings yet
- Mycobacterium SpeciesDocument13 pagesMycobacterium SpeciesSakshi SangleNo ratings yet
- Vein of Galen MalformationDocument69 pagesVein of Galen MalformationBhupendra GuptaNo ratings yet
- The Students' ProblemDocument21 pagesThe Students' ProblemAmairaNo ratings yet
- Medipoint Hospital, AundhDocument26 pagesMedipoint Hospital, AundhVivek SinghNo ratings yet
- An Introduction To Cognitive Psychology Processes and Disorders 3Rd Edition Full ChapterDocument41 pagesAn Introduction To Cognitive Psychology Processes and Disorders 3Rd Edition Full Chapterjohn.hill578100% (21)
- Perlis CRF Renal ReplacementDocument65 pagesPerlis CRF Renal ReplacementFikri SeptianNo ratings yet
- GRADE HandbookDocument75 pagesGRADE HandbookEzequiel ZacañinoNo ratings yet
- 2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishDocument169 pages2000+ MCQS With Solution: of Physics, Chemistry, Biology, Maths & EnglishMuhammad UmairNo ratings yet
- 5096 s07 Ms 2Document7 pages5096 s07 Ms 2mstudy1234560% (1)