Download as pdf or txt
You might also like
- Re Admission FormDocument2 pagesRe Admission FormMissy SamanthaNo ratings yet
- Application Form Evaluation and Other Forms PDFDocument6 pagesApplication Form Evaluation and Other Forms PDFMaria Olivia AquinoNo ratings yet
- Application For Transfer: The University of The West Indies St. AugustineDocument3 pagesApplication For Transfer: The University of The West Indies St. AugustineRashaad TurksonNo ratings yet
- Fm-Uro-007-Application For Graduation 01.17.2022Document3 pagesFm-Uro-007-Application For Graduation 01.17.2022lee tohNo ratings yet
- Application For Leave of Absence (Loa) : Program Adviser Department Chair Director of UG/G ProgramDocument2 pagesApplication For Leave of Absence (Loa) : Program Adviser Department Chair Director of UG/G ProgramdyrandzNo ratings yet
- Teaching Staff Application FormatDocument2 pagesTeaching Staff Application FormatbadrinathNo ratings yet
- Slu GradDocument3 pagesSlu GradCabbage BunsNo ratings yet
- Petition Form PDFDocument1 pagePetition Form PDFAdnan KamalNo ratings yet
- Mentor-Mentee FormatDocument3 pagesMentor-Mentee FormatZafarNo ratings yet
- Bio Data Form Intership Traineeship PDFDocument1 pageBio Data Form Intership Traineeship PDFSabiha RajpootNo ratings yet
- Xavier University Application FormDocument2 pagesXavier University Application FormAlton Melvar M DapanasNo ratings yet
- Application For Leave of Absence (Loa)Document1 pageApplication For Leave of Absence (Loa)John CenaNo ratings yet
- XS BOT Nomination - Form.2011Document1 pageXS BOT Nomination - Form.2011daro3071No ratings yet
- Application For Graduate ScholarshipDocument3 pagesApplication For Graduate ScholarshipGavin BovellNo ratings yet
- Application For Leave of Absence: Ateneo de Manila UniversityDocument4 pagesApplication For Leave of Absence: Ateneo de Manila UniversityKent Emmanuel C. SoriaNo ratings yet
- Honors College Undergraduate Petition: I RequestDocument2 pagesHonors College Undergraduate Petition: I RequestEric MoralesNo ratings yet
- Syracuse University - School of Education Formal Doctoral ProgramDocument4 pagesSyracuse University - School of Education Formal Doctoral ProgramLaura Knieser ReederNo ratings yet
- Application To Study Updated - Template DepEdDocument3 pagesApplication To Study Updated - Template DepEdfrenalyne.tabernillaNo ratings yet
- Swof ClaimDocument1 pageSwof ClaimAbdul basitNo ratings yet
- RIT Internship Form 240603 145818Document2 pagesRIT Internship Form 240603 145818madhavan cNo ratings yet
- Application Form For Orientation CourseDocument3 pagesApplication Form For Orientation CourseAmit Kurmar SharmaNo ratings yet
- Graduate Studies Admission Department Recommendation Form (Derf)Document1 pageGraduate Studies Admission Department Recommendation Form (Derf)Archangel GabNo ratings yet
- Phi Iri Entry Form Corrected Copy1Document2 pagesPhi Iri Entry Form Corrected Copy1Jan Michael FloreceNo ratings yet
- University of The East: UE Form S-No. (DRRM-Revised March 2009)Document1 pageUniversity of The East: UE Form S-No. (DRRM-Revised March 2009)Ryan PadiernosNo ratings yet
- Admission SlipDocument7 pagesAdmission SlipRachelle Melegrito BernabeNo ratings yet
- Nomination FormDocument6 pagesNomination Formdeosa villamonteNo ratings yet
- Form 9Document1 pageForm 9Nino James PorfecioNo ratings yet
- Application For Cross Enrolment FormDocument1 pageApplication For Cross Enrolment FormArlene Magalang NatividadNo ratings yet
- Transcript Application FormDocument3 pagesTranscript Application FormPrabhansh VarshneyNo ratings yet
- Student Medical CertificateDocument1 pageStudent Medical CertificateZhichao WangNo ratings yet
- AFG EnggArkiDocument2 pagesAFG EnggArkiGerald Vincent BorjaNo ratings yet
- Enrollment Adjusment Form: Please Check The Appropriate Box and Write Clearly The Information NeededDocument1 pageEnrollment Adjusment Form: Please Check The Appropriate Box and Write Clearly The Information NeededRena Rose MalunesNo ratings yet
- Shifting Form: CC: Guidance Office, Registrar, New DeanDocument2 pagesShifting Form: CC: Guidance Office, Registrar, New DeanMai PalerNo ratings yet
- Antrag Auf Nachteilsausgleich 190807 EngDocument3 pagesAntrag Auf Nachteilsausgleich 190807 EngJL CNo ratings yet
- WAGNER COLLEGE Non Degree AppicationDocument2 pagesWAGNER COLLEGE Non Degree Appicationjoedy_27joedy_27No ratings yet
- Pet ExceptDocument1 pagePet ExceptnathanmockNo ratings yet
- KwaZulu Natal Department of Transport Bursary Application FormDocument8 pagesKwaZulu Natal Department of Transport Bursary Application FormMandisa ZibulaNo ratings yet
- Undergraduate Application Form-23022022Document2 pagesUndergraduate Application Form-23022022bongisebodgeNo ratings yet
- Admission Form 2024 25Document3 pagesAdmission Form 2024 25ayushkolhe90No ratings yet
- Universityofmauritius: Application FormDocument2 pagesUniversityofmauritius: Application FormDivwinDier100% (1)
- Cap College Foundation, Inc. Request For School Credentials: Check The Credentials Being RequestedDocument1 pageCap College Foundation, Inc. Request For School Credentials: Check The Credentials Being RequestedChristian HizolaNo ratings yet
- Directed Studies Course request-CIVL592Document2 pagesDirected Studies Course request-CIVL592havarticanNo ratings yet
- Application Format For LibrarianDocument2 pagesApplication Format For Librariansuryadavas3221No ratings yet
- Adding Changing Dropping FormDocument2 pagesAdding Changing Dropping Formrunish venganzaNo ratings yet
- School: Annual Confidential ReportDocument13 pagesSchool: Annual Confidential ReportFarina Martins100% (1)
- Upform3 1Document5 pagesUpform3 1ntyt4qzdpxNo ratings yet
- Application For Graduation-SignedDocument3 pagesApplication For Graduation-SignedJoseph ApostolNo ratings yet
- Extencircumpet (1) Carteret CommDocument2 pagesExtencircumpet (1) Carteret Commcrclccanointed1No ratings yet
- University of Mauritius Vacancies Job Vacancy Application FormDocument2 pagesUniversity of Mauritius Vacancies Job Vacancy Application FormtodadaNo ratings yet
- Eligibility: - Photo Field of StudyDocument6 pagesEligibility: - Photo Field of StudyNeyo MaharodNo ratings yet
- Forms ResearchDocument4 pagesForms ResearchAnalou LopezNo ratings yet
- Undertaking ODL22Document1 pageUndertaking ODL22GurpreetNo ratings yet
- UREG QF 14 Application For Graduation Revision 1Document1 pageUREG QF 14 Application For Graduation Revision 1MaryJoyAnne DavocolNo ratings yet
- University of The Philippines DilimanDocument4 pagesUniversity of The Philippines DilimanPoison IvyNo ratings yet
- Intercampus Migration FormDocument2 pagesIntercampus Migration FormxaneNo ratings yet
- Pcatp FormDocument6 pagesPcatp FormOmer YousufNo ratings yet
- Fee ReceiptDocument1 pageFee ReceiptRachit SharmaNo ratings yet
- Beginners Sight and Read: Parent Pack For Strong Foundational Level Series 1From EverandBeginners Sight and Read: Parent Pack For Strong Foundational Level Series 1No ratings yet
- The Stress-Free Guide to Parenting a Child With ADHD: Effective and Proven Strategies for Alleviating Anxiety and Forming Strong Bonds Without the HassleFrom EverandThe Stress-Free Guide to Parenting a Child With ADHD: Effective and Proven Strategies for Alleviating Anxiety and Forming Strong Bonds Without the HassleNo ratings yet
- GEND3032 Outline24Document13 pagesGEND3032 Outline24Kamera RightNo ratings yet
- SEWING INSTRUCTIONS - Hela Cloth Menstrual Pads - Hela Cloth Pantyliners - Kulmine - ENDocument8 pagesSEWING INSTRUCTIONS - Hela Cloth Menstrual Pads - Hela Cloth Pantyliners - Kulmine - ENKamera RightNo ratings yet
- 4 GROUP 3 Reality of Trade - The WTO and DevelopingDocument11 pages4 GROUP 3 Reality of Trade - The WTO and DevelopingKamera RightNo ratings yet
- 2023-2024 MoC Course OutlineDocument10 pages2023-2024 MoC Course OutlineKamera RightNo ratings yet
- Kuratko 9 e CH 04Document33 pagesKuratko 9 e CH 04lobna_qassem7176No ratings yet
- Coard - Unit 2 Workbook Becoming BilingualDocument22 pagesCoard - Unit 2 Workbook Becoming BilingualKamera RightNo ratings yet
- Govt2049 Tutorial Worksheet 2023 2024 FinDocument4 pagesGovt2049 Tutorial Worksheet 2023 2024 FinKamera RightNo ratings yet
- Kuratko 9 e CH 06Document23 pagesKuratko 9 e CH 06Kamera RightNo ratings yet
- Direct and Indirect Object PronounsDocument2 pagesDirect and Indirect Object PronounsKamera RightNo ratings yet
- Business Model Development WorksheetDocument16 pagesBusiness Model Development WorksheetKamera RightNo ratings yet
- Breakeven - Analysis ExampleDocument1 pageBreakeven - Analysis ExampleKamera RightNo ratings yet
- Govt 2048 Tutorial Sheet 2022Document8 pagesGovt 2048 Tutorial Sheet 2022Kamera RightNo ratings yet
- 12 Month P L ExampleDocument1 page12 Month P L ExampleKamera RightNo ratings yet
- Racial Profiling and The War On Terror - Changing Trends and PerspDocument25 pagesRacial Profiling and The War On Terror - Changing Trends and PerspKamera RightNo ratings yet
- Protectionism and Trade A Country's Glory or Doom OriginalDocument10 pagesProtectionism and Trade A Country's Glory or Doom OriginalKamera RightNo ratings yet
- 2022 PHC Additional Information Form: Interview TranscriptDocument5 pages2022 PHC Additional Information Form: Interview TranscriptKamera RightNo ratings yet
- 7 Jurisdictional Immunities - 2020-2021Document32 pages7 Jurisdictional Immunities - 2020-2021Kamera RightNo ratings yet
- BSC International Relations Major Checklist 2021-2022 0Document1 pageBSC International Relations Major Checklist 2021-2022 0Kamera RightNo ratings yet
- Business ProposalDocument25 pagesBusiness ProposalKamera RightNo ratings yet
- Comparative AnalysisDocument9 pagesComparative AnalysisKamera RightNo ratings yet
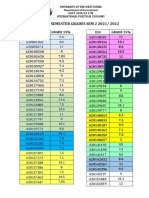
- Govt 2049 Mid Semester Grades 2022Document1 pageGovt 2049 Mid Semester Grades 2022Kamera RightNo ratings yet
- Islam Is The New Black - Muslim Perceptions of Law EnforcementDocument11 pagesIslam Is The New Black - Muslim Perceptions of Law EnforcementKamera RightNo ratings yet
- 12 Professional House Cleaning Checklists JobberDocument5 pages12 Professional House Cleaning Checklists JobberKamera Right100% (2)
- ABJam17-v18 0 3 2-Eng-170213 - WDocument41 pagesABJam17-v18 0 3 2-Eng-170213 - WKamera RightNo ratings yet
- Madarsa Scheme SPQEMDocument6 pagesMadarsa Scheme SPQEMmanam101No ratings yet
- MBBS & BDS Session (2018-19) Schedule: Attention Candidates ForDocument3 pagesMBBS & BDS Session (2018-19) Schedule: Attention Candidates ForAndersen HarrisNo ratings yet
- 0625 w19 Ms 11 PDFDocument3 pages0625 w19 Ms 11 PDFsuperpooh-1No ratings yet
- Philippine Educational Practices in The Philippines and Their Legal BasesDocument27 pagesPhilippine Educational Practices in The Philippines and Their Legal BasesChristine Joy Torralba-MarianoNo ratings yet
- Fiziks: Banaras Hindu University (B.H.U) Entrance Test For The M.Sc. Physics ProgrammeDocument1 pageFiziks: Banaras Hindu University (B.H.U) Entrance Test For The M.Sc. Physics ProgrammeHritikNo ratings yet
- GST 301 Question 18-19 UpdatedDocument5 pagesGST 301 Question 18-19 Updatedusmankirya4610No ratings yet
- DownloaddocDocument16 pagesDownloaddocShubham WaghmareNo ratings yet
- Miles CPA Roadmap1Document42 pagesMiles CPA Roadmap1GNR ASSOCIATESNo ratings yet
- 10th MarksheetDocument1 page10th Marksheetsr6714336No ratings yet
- Working Paper 04 - EMIS Case Study GhanaDocument24 pagesWorking Paper 04 - EMIS Case Study GhanasceneoritaNo ratings yet
- JKUAT Bachelors Degree Placement ListDocument179 pagesJKUAT Bachelors Degree Placement ListDiana WangamatiNo ratings yet
- Sample Offer Letter 71 NewDocument2 pagesSample Offer Letter 71 Newlaxmib25No ratings yet
- 3rd Update-Cancelled ExamDocument3 pages3rd Update-Cancelled ExamHiba HassanNo ratings yet
- Graduate Diploma in LawDocument7 pagesGraduate Diploma in LawMaruthi MaddipatlaNo ratings yet
- Sbipo1819 WRTN Result PDFDocument11 pagesSbipo1819 WRTN Result PDFPhani Sekhar SarmaNo ratings yet
- KVS Recruitment 2016 PGT TGT PRT PDFDocument19 pagesKVS Recruitment 2016 PGT TGT PRT PDFATI039 POOVAIMANAGAR GHSSNo ratings yet
- Kalinga UniversityDocument6 pagesKalinga UniversitySarthak SidhantNo ratings yet
- IgcseDocument5 pagesIgcseWing Zoom4No ratings yet
- Assessment FrameworkDocument50 pagesAssessment FrameworkCharles OndiekiNo ratings yet
- Universitas Padjadjaran: LL L L L LL L L L LL LLL L LL LL L LLL 11Document1 pageUniversitas Padjadjaran: LL L L L LL L L L LL LLL L LL LL L LLL 11Raden FashaNo ratings yet
- Madurai Seniority ListDocument292 pagesMadurai Seniority Listnowshatkhan50% (2)
- PHD RulesDocument29 pagesPHD RulesSriVenkateswaranKothandapanyNo ratings yet
- Annexure-I (M) Pharmacy Council of India: (SIF-E)Document14 pagesAnnexure-I (M) Pharmacy Council of India: (SIF-E)ManKapNo ratings yet
- 0580 Mathematics: MARK SCHEME For The May/June 2013 SeriesDocument4 pages0580 Mathematics: MARK SCHEME For The May/June 2013 SeriesAhmed SherifNo ratings yet
- Kilifi CountyDocument17 pagesKilifi CountyJohn Munene KarokiNo ratings yet
- Factsheet New Skills Agenda For EU - 09Document2 pagesFactsheet New Skills Agenda For EU - 09Murali RamanathNo ratings yet
- New M.S. Students: Me 8Xx Me 9XxDocument4 pagesNew M.S. Students: Me 8Xx Me 9XxFatima GORINENo ratings yet
- 0520 s14 Ms 12 PDFDocument12 pages0520 s14 Ms 12 PDFlauranistNo ratings yet
- Health Sciences 2021 FinalDocument418 pagesHealth Sciences 2021 FinalMandlakhe HadebeNo ratings yet