Download as doc, pdf, or txt
You might also like
- Drug Study Heparin and FenylDocument4 pagesDrug Study Heparin and FenylAnisa Jamito75% (4)
- Common Cases in Vascular SurgeryDocument72 pagesCommon Cases in Vascular Surgerynohazz100% (2)
- Dr. Kiki - Pengantar Trauma UpdateDocument20 pagesDr. Kiki - Pengantar Trauma UpdateRsud Malinau Ppk Blud100% (1)
- Rauma Epar: Soetamto Wibowo Bagian Bedah FK UNAIR / RSUD DR Soetomo SurabayaDocument37 pagesRauma Epar: Soetamto Wibowo Bagian Bedah FK UNAIR / RSUD DR Soetomo SurabayaMuhammad FirdausNo ratings yet
- Byecsu SurgDocument22 pagesByecsu SurgBea Y. Bas-ongNo ratings yet
- Limb Ischemia VascularDocument6 pagesLimb Ischemia Vascularalbadrimohammed1997No ratings yet
- Arteriovenous Malformation 1001Document19 pagesArteriovenous Malformation 1001housic1No ratings yet
- Abdominal Trauma Algorithm - FHADocument53 pagesAbdominal Trauma Algorithm - FHAKevin AdrianNo ratings yet
- Materi - Acute Limb IschemiaDocument29 pagesMateri - Acute Limb IschemiaPutra AchmadNo ratings yet
- L 4 The Positive Remodeling Effect of Paclitaxel DCB - DR - NgoMinhHungDocument43 pagesL 4 The Positive Remodeling Effect of Paclitaxel DCB - DR - NgoMinhHungNguyễn Bạch Vân ThủyNo ratings yet
- Akut Limb IskemikDocument31 pagesAkut Limb IskemikLaluMuhammadSabarSetiawanNo ratings yet
- EAU Pocket On Urological Trauma 2022Document18 pagesEAU Pocket On Urological Trauma 2022Fco. Javier Hernández CalderónNo ratings yet
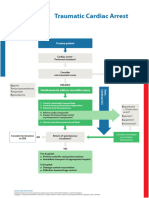
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteDocument1 pagePoster SpecCircs Traumatic Cardiac Arrest Algorithm ENG V20151005 HRES SiteangelologrilloNo ratings yet
- Care of The Post PICA (Stent)Document75 pagesCare of The Post PICA (Stent)benypermadiNo ratings yet
- Eau Guidelines On Urological Trauma: (Limited Text Update March 2017)Document18 pagesEau Guidelines On Urological Trauma: (Limited Text Update March 2017)Peri HidayatNo ratings yet
- Angiography (Cardiac Catherization) : Patient Teaching/preparationDocument2 pagesAngiography (Cardiac Catherization) : Patient Teaching/preparationpsyNo ratings yet
- Vicpostoporderform WebDocument2 pagesVicpostoporderform WebJunaid ShahNo ratings yet
- Algorithm of Resuscitation CareDocument1 pageAlgorithm of Resuscitation CarejyothiNo ratings yet
- CIT1Document25 pagesCIT1chris wangNo ratings yet
- SIMPO 1.2 DR WIZA - The Practicality of Enoxaparin Across ACS Spectrum - 2022Document23 pagesSIMPO 1.2 DR WIZA - The Practicality of Enoxaparin Across ACS Spectrum - 2022yan salviantoNo ratings yet
- Anticoagulation in Percutaneous Coronary Intervention: ReviewDocument19 pagesAnticoagulation in Percutaneous Coronary Intervention: ReviewMahmud Rahman AljuklanNo ratings yet
- Damage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and CorpsmenDocument1 pageDamage - Control - Resus - Quick - Reference - Guide - Medics - Corpsmen - 2023-Quick Reference Guide For Combat Medics and Corpsmenchou youNo ratings yet
- EAU Pocket Guidelines Urological Trauma 2019Document18 pagesEAU Pocket Guidelines Urological Trauma 2019felixNo ratings yet
- Resuscitation in Retroperitoneal HaemorrhageDocument39 pagesResuscitation in Retroperitoneal Haemorrhagemark chrisatyaNo ratings yet
- Syncope Dr. Adrian RIzal PKB 2019Document39 pagesSyncope Dr. Adrian RIzal PKB 2019Fandy Hazzy AlfataNo ratings yet
- Diagnosis and Treatment of Radiation ProctitisDocument2 pagesDiagnosis and Treatment of Radiation ProctitispatNo ratings yet
- Kim Johnson Kardex To Discharge PlanDocument13 pagesKim Johnson Kardex To Discharge PlanFranz Patrick Legria, CPAC - SNNo ratings yet
- Acute Medicine: Shock: Inadequate Tissue and Organ PerfusionDocument3 pagesAcute Medicine: Shock: Inadequate Tissue and Organ Perfusionmyat252No ratings yet
- Poster SpecCircs Traumatic Cardiac Arrest Algorithm SERB V20160714 HRESDocument1 pagePoster SpecCircs Traumatic Cardiac Arrest Algorithm SERB V20160714 HRESJelena TadićNo ratings yet
- Venous Intervention - GSV Ablation FINALDocument43 pagesVenous Intervention - GSV Ablation FINALaaaaaaNo ratings yet
- The Use of Methylene Blue in The Abdominal Aortic Surgery: A Case ReportDocument4 pagesThe Use of Methylene Blue in The Abdominal Aortic Surgery: A Case Reportserena7205No ratings yet
- Platelet Transfusion Guidelines NewDocument5 pagesPlatelet Transfusion Guidelines Newgautam harshNo ratings yet
- Pulmonary EmbolismDocument61 pagesPulmonary Embolismjhk0428No ratings yet
- Vascular AnesthesiaDocument6 pagesVascular AnesthesiaVignesh VenkatesanNo ratings yet
- Post Operative ComplicationsDocument11 pagesPost Operative ComplicationsIlyas HarunNo ratings yet
- POST OP BrunnerDocument7 pagesPOST OP Brunnerjamie carpioNo ratings yet
- Abdominal PDFDocument1 pageAbdominal PDFChakra BaktiNo ratings yet
- Acute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticeDocument54 pagesAcute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticeKiara GovenderNo ratings yet
- EAU Guidelines On Sexual and Reproductive Health 2022 - 2022 03 29 084141 - Megw (110 111)Document2 pagesEAU Guidelines On Sexual and Reproductive Health 2022 - 2022 03 29 084141 - Megw (110 111)CRISTH KIMBERLY ENEQUE DE LA CRUZNo ratings yet
- Pak Jaenal - Askep Acs - Scu - PPTDocument37 pagesPak Jaenal - Askep Acs - Scu - PPTDilaNo ratings yet
- Artigo - Valve Heart Surgery in BrazilDocument12 pagesArtigo - Valve Heart Surgery in BrazilRBonrukNo ratings yet
- Obscure Gastrointestinal Bleeding: Chylous AscitesDocument2 pagesObscure Gastrointestinal Bleeding: Chylous AscitesMintdonNo ratings yet
- Vascular Interventional RadiologyDocument1 pageVascular Interventional RadiologywhitecoatNo ratings yet
- Peripheral Vascular Disease and Amputations: Moderator: MR MZ ShaikDocument9 pagesPeripheral Vascular Disease and Amputations: Moderator: MR MZ ShaikhshshzjxjNo ratings yet
- Pharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)Document44 pagesPharmacological Management of Acute Coronary Syndromes (ACS) and Acute Limb Ischemia (ALI)hendratj90No ratings yet
- Aboyans v. Esc Congress 2018 Est Carotidea Severa AsintDocument32 pagesAboyans v. Esc Congress 2018 Est Carotidea Severa Asintkelicita kitNo ratings yet
- Slide WS 2 Dr. Junior, SP - JP (K)Document18 pagesSlide WS 2 Dr. Junior, SP - JP (K)Luh Leni AriniNo ratings yet
- Stroke Physician: Discharge ChecklistDocument4 pagesStroke Physician: Discharge ChecklistEllaNo ratings yet
- The Radiology Assistant - CT in TraumaDocument18 pagesThe Radiology Assistant - CT in Traumaابو عبد الرحمنNo ratings yet
- Laporan Kematian DigestDocument5 pagesLaporan Kematian DigestJusticia AndhikaNo ratings yet
- Philippe Setup Ra Unit (Khoá gây tê vùng dưới hướng dẫn siêu âm ĐHYHN)Document36 pagesPhilippe Setup Ra Unit (Khoá gây tê vùng dưới hướng dẫn siêu âm ĐHYHN)Rùa’s Anesthesia HanoiNo ratings yet
- Acute FiaDocument2 pagesAcute FiaAndrei MurariuNo ratings yet
- VTE Prophylaxis GuidelinesDocument1 pageVTE Prophylaxis GuidelinesSylvia Ruth Alisa Nababan100% (1)
- Surgery Cases: CASE 1: Blunt Abdominal TraumaDocument3 pagesSurgery Cases: CASE 1: Blunt Abdominal TraumaGio Tamaño BalisiNo ratings yet
- Guidelines For The Management of Intracerebral HaemorrhageDocument18 pagesGuidelines For The Management of Intracerebral Haemorrhagerebeca marityNo ratings yet
- Acute Coronary Syndrome: History and Clinical Assessment Suggest ACSDocument12 pagesAcute Coronary Syndrome: History and Clinical Assessment Suggest ACSginongNo ratings yet
- Lesson 5Document3 pagesLesson 5NER CARLO SANTOSNo ratings yet
- Hemophilia MX SOPDocument1 pageHemophilia MX SOPdhvanishah0313No ratings yet
- Atlas of Coronary Intravascular Optical Coherence TomographyFrom EverandAtlas of Coronary Intravascular Optical Coherence TomographyNo ratings yet
- Pathophysiology of Lun in SepsisDocument2 pagesPathophysiology of Lun in Sepsisvidro alifNo ratings yet
- Stent EsophagusDocument24 pagesStent Esophagusvidro alifNo ratings yet
- Digestive 01Document12 pagesDigestive 01vidro alifNo ratings yet
- AbstrakDocument2 pagesAbstrakvidro alifNo ratings yet
- Abstrak Giant GallstonesDocument1 pageAbstrak Giant Gallstonesvidro alifNo ratings yet
- Bladder Cancer: DR Vidro Alif Gunawan Departemen Bedah Universitas Sriwijaya PalembangDocument24 pagesBladder Cancer: DR Vidro Alif Gunawan Departemen Bedah Universitas Sriwijaya Palembangvidro alifNo ratings yet
- Ward Report 21-2-19Document13 pagesWard Report 21-2-19vidro alifNo ratings yet
- Final NeuronotesDocument16 pagesFinal Neuronotesapi-479939114No ratings yet
- Mitochondria and ChloroplastsDocument19 pagesMitochondria and ChloroplastsNadane Aldover100% (1)
- CardiacassessmentDocument40 pagesCardiacassessmentsasNo ratings yet
- Patient PositioningDocument76 pagesPatient PositioningLaxman KannaNo ratings yet
- Autonomic Nervous SystemDocument28 pagesAutonomic Nervous Systemglad mohesh100% (1)
- Maximal Pre-Excitation Based Algorithm For Localization of Manifest Accessory Pathways in AdultsDocument10 pagesMaximal Pre-Excitation Based Algorithm For Localization of Manifest Accessory Pathways in AdultsFredy TandriNo ratings yet
- Askep Abuse Child Kasus 2Document7 pagesAskep Abuse Child Kasus 2Salsabila izzatunnisaaNo ratings yet
- Erc - 2005Document58 pagesErc - 2005zulfantri1983No ratings yet
- Pleullar EffusionDocument20 pagesPleullar EffusionGopi GNo ratings yet
- Inflammation and Types of Inflammation-1Document9 pagesInflammation and Types of Inflammation-1Shalabh JoharyNo ratings yet
- Physiological Mechanisms of PainDocument7 pagesPhysiological Mechanisms of PainZAFFAR QURESHINo ratings yet
- Muscle MetabolismDocument63 pagesMuscle MetabolismAmanuel MaruNo ratings yet
- CHAPTER 2 - Textbook ExerciseDocument8 pagesCHAPTER 2 - Textbook ExerciseLeena HingNo ratings yet
- General Biology 2-201-270Document70 pagesGeneral Biology 2-201-270Sab IbarretaNo ratings yet
- Checklist & Algoritma ACLSDocument16 pagesChecklist & Algoritma ACLSNadhif JovaldyNo ratings yet
- Responsi Stemi Dr. Tuko SP - JP FixDocument56 pagesResponsi Stemi Dr. Tuko SP - JP FixcintaNo ratings yet
- Fiziologie Valori Normale PDFDocument1 pageFiziologie Valori Normale PDFStaicu GabrielNo ratings yet
- Airway and VentilatoryDocument22 pagesAirway and VentilatoryAbdullah MatarNo ratings yet
- Medical Surgical Nursing Bullets (Nle & Nclex)Document105 pagesMedical Surgical Nursing Bullets (Nle & Nclex)Cuzii marieeNo ratings yet
- Acid Base BalanceDocument13 pagesAcid Base BalanceRashed ShatnawiNo ratings yet
- Personal Hormonal Profiling Refresh #4 - Personal Trainer OpleidingDocument13 pagesPersonal Hormonal Profiling Refresh #4 - Personal Trainer OpleidingOverload WorldwideNo ratings yet
- Physiology Lab 2 FinalDocument3 pagesPhysiology Lab 2 Finalaileen agustin100% (6)
- Chemical Coordination and Integration: SolutionsDocument10 pagesChemical Coordination and Integration: SolutionsIhtisham Ul HaqNo ratings yet
- Heat-Stress PptshowDocument22 pagesHeat-Stress Pptshowusman rasheedNo ratings yet
- BFP QuestionnaireDocument19 pagesBFP QuestionnaireSathish SaciNo ratings yet
- Integrated Test For The Fisrt 4 Modules (A)Document39 pagesIntegrated Test For The Fisrt 4 Modules (A)Danielle RibeiroNo ratings yet
- 28 Years Male With Quadriparesis FinalDocument52 pages28 Years Male With Quadriparesis Finalsaleh ahmedNo ratings yet
- Pengkajian Luka DasarDocument56 pagesPengkajian Luka DasarFitri aniNo ratings yet
- 4HB1 01 Rms 20200305Document13 pages4HB1 01 Rms 20200305Engy Hisham MarwanNo ratings yet
- Animal Skeletons A Worksheet by Vijay Kumar HeerDocument3 pagesAnimal Skeletons A Worksheet by Vijay Kumar HeerVIJAY KUMAR HEERNo ratings yet