
Immunization History Form
Immunization History Form
You might also like
- Secdocument - 38download Advanced Practice Palliative Nursing 2Nd Edition Constance Dahlin Full ChapterDocument67 pagesSecdocument - 38download Advanced Practice Palliative Nursing 2Nd Edition Constance Dahlin Full Chapternaomi.parker972100% (9)
- Are Clear Aligners Better Than The Conventional Orthodontic FixedDocument9 pagesAre Clear Aligners Better Than The Conventional Orthodontic Fixed黎燦燦No ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of Immunizationashish guptaNo ratings yet
- John Jay Immunization FormDocument3 pagesJohn Jay Immunization FormIsam BoukattayaNo ratings yet
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- Immunization Record: Form Is Due at OrientationDocument3 pagesImmunization Record: Form Is Due at OrientationCasey JonesNo ratings yet
- Cuny Immunization Record FormDocument2 pagesCuny Immunization Record Formmichael JacksonNo ratings yet
- FIU Immunization Documentation FormDocument2 pagesFIU Immunization Documentation FormMO MONo ratings yet
- Rhodes Immunization RecordDocument5 pagesRhodes Immunization RecordDr.P.S.N RajuNo ratings yet
- Fall 2024 Proof of MMR and Meningitis Vaccine Form - FillableDocument1 pageFall 2024 Proof of MMR and Meningitis Vaccine Form - FillableMicman12No ratings yet
- Univ of Florida ImmunisationDocument2 pagesUniv of Florida ImmunisationPavan Kumar MangipudiNo ratings yet
- Immunization Requirement Form - UpdateDocument2 pagesImmunization Requirement Form - UpdateManojkumar ANo ratings yet
- An Important FormDocument3 pagesAn Important FormRachel ColeNo ratings yet
- CUB - Immunisation FormDocument2 pagesCUB - Immunisation FormArcane BeingNo ratings yet
- Instructions For Completion of UA Immunization FormDocument4 pagesInstructions For Completion of UA Immunization FormJ StockmanNo ratings yet
- Immunization FormsDocument6 pagesImmunization FormsNadya IrsalinaNo ratings yet
- Immun RecordDocument2 pagesImmun RecordNonofYaNo ratings yet
- C4 PIC Imm Packet 4.2024Document4 pagesC4 PIC Imm Packet 4.2024c2184841No ratings yet
- James Madison University Immunization FormDocument1 pageJames Madison University Immunization FormMiguel EspirituNo ratings yet
- Immunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationDocument7 pagesImmunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationShubham TrivediNo ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of ImmunizationАида АрзуманянNo ratings yet
- Mandatory Immunization FormDocument5 pagesMandatory Immunization FormlxndrcrowleyNo ratings yet
- Health Immunization MMR FormDocument2 pagesHealth Immunization MMR FormHenrique Delfino Almeida AlvesNo ratings yet
- ImmunizationCertificate PDFDocument2 pagesImmunizationCertificate PDFAnonymous kq5iEDxxhrNo ratings yet
- Varicella Immunization CertDocument2 pagesVaricella Immunization CertShaikahamedNo ratings yet
- (No Cash - Check or Money Order Only) : SECTION 2. To Be Completed by The Appropriate Official at The Medical SchoolDocument6 pages(No Cash - Check or Money Order Only) : SECTION 2. To Be Completed by The Appropriate Official at The Medical SchoolParthNo ratings yet
- Medical Record FormDocument4 pagesMedical Record FormДария КоваленкоNo ratings yet
- Patient Portal: OR Positive Titer Date: - / - / - If Twinrix Check HereDocument1 pagePatient Portal: OR Positive Titer Date: - / - / - If Twinrix Check HereNitai GAURANGANo ratings yet
- Immunization Form International Visiting StudentsDocument2 pagesImmunization Form International Visiting Studentsmellb99No ratings yet
- 2024 VPD FormFINAL 16012024Document5 pages2024 VPD FormFINAL 16012024dkid9876No ratings yet
- HMS Exchange Clerk Program Checklist: International Students Only: English InterviewDocument5 pagesHMS Exchange Clerk Program Checklist: International Students Only: English InterviewChristopher WuNo ratings yet
- Cuestionario de SaludDocument1 pageCuestionario de SaludLuis Sosa GodoyNo ratings yet
- Confidential Student Health Form.1.8.18Document4 pagesConfidential Student Health Form.1.8.18Kevin GreavesNo ratings yet
- Health History and Immunization Form: University of Valley Forge - Health CenterDocument4 pagesHealth History and Immunization Form: University of Valley Forge - Health CenterBernard AmetepeNo ratings yet
- Health Background Form 1Document4 pagesHealth Background Form 1Riya SuramNo ratings yet
- Immunization Record PART I: To Be Completed by The Student. Please Print or TypeDocument3 pagesImmunization Record PART I: To Be Completed by The Student. Please Print or Typeruhayl khanNo ratings yet
- Immreq15 16Document2 pagesImmreq15 16api-234991765No ratings yet
- COVID Vaccination Packet SFODocument16 pagesCOVID Vaccination Packet SFOferNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Immuz FormDocument2 pagesImmuz Formapi-250919827No ratings yet
- Rory Elliott 12 17 1997: Measles Vaccine Requirement Form (MMR)Document2 pagesRory Elliott 12 17 1997: Measles Vaccine Requirement Form (MMR)roryNo ratings yet
- USC Immunization Checklist FormDocument2 pagesUSC Immunization Checklist FormbuiiiilderNo ratings yet
- Student Immunization Form 2017-2018Document2 pagesStudent Immunization Form 2017-2018Yashu SharmaNo ratings yet
- Immunization RecordDocument1 pageImmunization RecordJane PhamNo ratings yet
- #F2F Student FormsDocument15 pages#F2F Student FormsMarlyn Dimatatac PanopioNo ratings yet
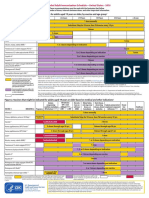
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Immunization Letter NB FORM RevisedDocument6 pagesImmunization Letter NB FORM RevisedUddhavendra Pal SinghNo ratings yet
- HE Form - 2011Document2 pagesHE Form - 2011peter1234uNo ratings yet
- Certificate of Immunization FormDocument1 pageCertificate of Immunization FormShaikahamedNo ratings yet
- Vaccination Requirements of IFMSA Exchange Progam in Israel-9.15Document2 pagesVaccination Requirements of IFMSA Exchange Progam in Israel-9.15Niko DobrilovicNo ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- Points To Remember in Cold Chain ManagementDocument6 pagesPoints To Remember in Cold Chain Managementpaul arvie violetaNo ratings yet
- 2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12Document4 pages2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12James AllenNo ratings yet
- Sequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDocument2 pagesSequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDonnaNo ratings yet
- MeningococcalDocument2 pagesMeningococcalLuai Sammy Abu-RayyanNo ratings yet
- Different COVID-19 VaccinesDocument3 pagesDifferent COVID-19 Vaccinesfsese05722No ratings yet
- Immunization Requirement - Student Health Center - The University of UtahDocument2 pagesImmunization Requirement - Student Health Center - The University of Utahmithun916No ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalNo ratings yet
- East Tennessee State Univer Meningococcal Meningitis and Hepatitis B Vaccine WaiverDocument1 pageEast Tennessee State Univer Meningococcal Meningitis and Hepatitis B Vaccine WaiverDonnaNo ratings yet
- Factsheet priorCOVID19infection ENGDocument5 pagesFactsheet priorCOVID19infection ENGVasilije MunjasNo ratings yet
- SOP For Retest of Raw MaterialsDocument3 pagesSOP For Retest of Raw MaterialsRainMan75100% (1)
- A Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)Document14 pagesA Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)asma khanNo ratings yet
- Navpers 18068F U.S. Navy Enlisted Classification Manual April 2012Document1,612 pagesNavpers 18068F U.S. Navy Enlisted Classification Manual April 2012VietVetSteve100% (1)
- Health and Safety FCX-HS34Document3 pagesHealth and Safety FCX-HS34berry trisnamuktiNo ratings yet
- Worksheet No.3: Grade 10Document5 pagesWorksheet No.3: Grade 10melvin ynionNo ratings yet
- Reading Comprehension Class 12 CbseDocument4 pagesReading Comprehension Class 12 CbseCbse AccountNo ratings yet
- AV eIFU 10223671 Mg-En V03Document68 pagesAV eIFU 10223671 Mg-En V03Goutham RevuruNo ratings yet
- Final Research Paper 2Document9 pagesFinal Research Paper 2api-510720092No ratings yet
- Committee 2020, Reporter, May Edition 2020, April 24, 2020Document32 pagesCommittee 2020, Reporter, May Edition 2020, April 24, 2020ucopresident_2130533No ratings yet
- Smallholder Vegetable Packhouses: Establishing and ManagingDocument50 pagesSmallholder Vegetable Packhouses: Establishing and ManagingMeet ShahNo ratings yet
- I. Sparq Manufacturing Management Department: Itec854 Danial Bavi / Id: 45485348Document6 pagesI. Sparq Manufacturing Management Department: Itec854 Danial Bavi / Id: 45485348fawas hamdiNo ratings yet
- Drug StudyDocument7 pagesDrug StudyKynaWeeNo ratings yet
- New Graduate RN Cover Letter SamplesDocument7 pagesNew Graduate RN Cover Letter Samplesf60pk9dc100% (3)
- 3 - Safety Plan (KH&B Co.,Ltd.)Document30 pages3 - Safety Plan (KH&B Co.,Ltd.)Wint PaingNo ratings yet
- Assignment in Advance ReadingDocument3 pagesAssignment in Advance ReadingJessa CaberteNo ratings yet
- Hy-Line Silver Brown Commercial Performance Standards ManualDocument16 pagesHy-Line Silver Brown Commercial Performance Standards Manualthanh ba matNo ratings yet
- Efect and Longevity of Botulinum Toxin in The Treatment of Gummy Smile - A Meta Analysis and Meta Regression - Zengiski, 2021Document9 pagesEfect and Longevity of Botulinum Toxin in The Treatment of Gummy Smile - A Meta Analysis and Meta Regression - Zengiski, 2021Rafael Autran Cavalcante AraújoNo ratings yet
- Solid Waste Management: M. Sc. Environmental Science Central University of RajasthanDocument21 pagesSolid Waste Management: M. Sc. Environmental Science Central University of RajasthanAvrenim Magaro DecanoNo ratings yet
- SLS Ginopol L24 151-21-3-MSDS US-GHSDocument8 pagesSLS Ginopol L24 151-21-3-MSDS US-GHSRG TNo ratings yet
- CPR WebDocument222 pagesCPR WebANo ratings yet
- Poison StandardDocument661 pagesPoison StandardmhutchzNo ratings yet
- 20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnDocument161 pages20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnNgọc HuyềnNo ratings yet
- Review On Inflammatory DisesesDocument21 pagesReview On Inflammatory Disesesdigitalmazdoor5201No ratings yet
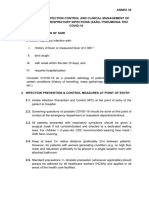
- Annex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Document4 pagesAnnex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Yeoh Zi-NingNo ratings yet
- Nurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationDocument4 pagesNurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationEmma WatsonNo ratings yet
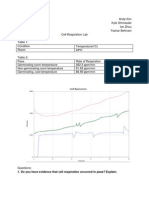
- Cellular Respiration LabDocument6 pagesCellular Respiration Labianzhou1No ratings yet
- Social Work Processes and MethodsDocument32 pagesSocial Work Processes and MethodsAaron Jay ZuluetaNo ratings yet
- 1842 13404 1 SMDocument7 pages1842 13404 1 SMnanda wildaNo ratings yet























































































Download as pdf or txt
You might also like
- Secdocument - 38download Advanced Practice Palliative Nursing 2Nd Edition Constance Dahlin Full ChapterDocument67 pagesSecdocument - 38download Advanced Practice Palliative Nursing 2Nd Edition Constance Dahlin Full Chapternaomi.parker972100% (9)
- Are Clear Aligners Better Than The Conventional Orthodontic FixedDocument9 pagesAre Clear Aligners Better Than The Conventional Orthodontic Fixed黎燦燦No ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of Immunizationashish guptaNo ratings yet
- John Jay Immunization FormDocument3 pagesJohn Jay Immunization FormIsam BoukattayaNo ratings yet
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- Immunization Record: Form Is Due at OrientationDocument3 pagesImmunization Record: Form Is Due at OrientationCasey JonesNo ratings yet
- Cuny Immunization Record FormDocument2 pagesCuny Immunization Record Formmichael JacksonNo ratings yet
- FIU Immunization Documentation FormDocument2 pagesFIU Immunization Documentation FormMO MONo ratings yet
- Rhodes Immunization RecordDocument5 pagesRhodes Immunization RecordDr.P.S.N RajuNo ratings yet
- Fall 2024 Proof of MMR and Meningitis Vaccine Form - FillableDocument1 pageFall 2024 Proof of MMR and Meningitis Vaccine Form - FillableMicman12No ratings yet
- Univ of Florida ImmunisationDocument2 pagesUniv of Florida ImmunisationPavan Kumar MangipudiNo ratings yet
- Immunization Requirement Form - UpdateDocument2 pagesImmunization Requirement Form - UpdateManojkumar ANo ratings yet
- An Important FormDocument3 pagesAn Important FormRachel ColeNo ratings yet
- CUB - Immunisation FormDocument2 pagesCUB - Immunisation FormArcane BeingNo ratings yet
- Instructions For Completion of UA Immunization FormDocument4 pagesInstructions For Completion of UA Immunization FormJ StockmanNo ratings yet
- Immunization FormsDocument6 pagesImmunization FormsNadya IrsalinaNo ratings yet
- Immun RecordDocument2 pagesImmun RecordNonofYaNo ratings yet
- C4 PIC Imm Packet 4.2024Document4 pagesC4 PIC Imm Packet 4.2024c2184841No ratings yet
- James Madison University Immunization FormDocument1 pageJames Madison University Immunization FormMiguel EspirituNo ratings yet
- Immunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationDocument7 pagesImmunizations Page Effective Spring 2010 Guidelines For Completing Immunization InformationShubham TrivediNo ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of ImmunizationАида АрзуманянNo ratings yet
- Mandatory Immunization FormDocument5 pagesMandatory Immunization FormlxndrcrowleyNo ratings yet
- Health Immunization MMR FormDocument2 pagesHealth Immunization MMR FormHenrique Delfino Almeida AlvesNo ratings yet
- ImmunizationCertificate PDFDocument2 pagesImmunizationCertificate PDFAnonymous kq5iEDxxhrNo ratings yet
- Varicella Immunization CertDocument2 pagesVaricella Immunization CertShaikahamedNo ratings yet
- (No Cash - Check or Money Order Only) : SECTION 2. To Be Completed by The Appropriate Official at The Medical SchoolDocument6 pages(No Cash - Check or Money Order Only) : SECTION 2. To Be Completed by The Appropriate Official at The Medical SchoolParthNo ratings yet
- Medical Record FormDocument4 pagesMedical Record FormДария КоваленкоNo ratings yet
- Patient Portal: OR Positive Titer Date: - / - / - If Twinrix Check HereDocument1 pagePatient Portal: OR Positive Titer Date: - / - / - If Twinrix Check HereNitai GAURANGANo ratings yet
- Immunization Form International Visiting StudentsDocument2 pagesImmunization Form International Visiting Studentsmellb99No ratings yet
- 2024 VPD FormFINAL 16012024Document5 pages2024 VPD FormFINAL 16012024dkid9876No ratings yet
- HMS Exchange Clerk Program Checklist: International Students Only: English InterviewDocument5 pagesHMS Exchange Clerk Program Checklist: International Students Only: English InterviewChristopher WuNo ratings yet
- Cuestionario de SaludDocument1 pageCuestionario de SaludLuis Sosa GodoyNo ratings yet
- Confidential Student Health Form.1.8.18Document4 pagesConfidential Student Health Form.1.8.18Kevin GreavesNo ratings yet
- Health History and Immunization Form: University of Valley Forge - Health CenterDocument4 pagesHealth History and Immunization Form: University of Valley Forge - Health CenterBernard AmetepeNo ratings yet
- Health Background Form 1Document4 pagesHealth Background Form 1Riya SuramNo ratings yet
- Immunization Record PART I: To Be Completed by The Student. Please Print or TypeDocument3 pagesImmunization Record PART I: To Be Completed by The Student. Please Print or Typeruhayl khanNo ratings yet
- Immreq15 16Document2 pagesImmreq15 16api-234991765No ratings yet
- COVID Vaccination Packet SFODocument16 pagesCOVID Vaccination Packet SFOferNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Immuz FormDocument2 pagesImmuz Formapi-250919827No ratings yet
- Rory Elliott 12 17 1997: Measles Vaccine Requirement Form (MMR)Document2 pagesRory Elliott 12 17 1997: Measles Vaccine Requirement Form (MMR)roryNo ratings yet
- USC Immunization Checklist FormDocument2 pagesUSC Immunization Checklist FormbuiiiilderNo ratings yet
- Student Immunization Form 2017-2018Document2 pagesStudent Immunization Form 2017-2018Yashu SharmaNo ratings yet
- Immunization RecordDocument1 pageImmunization RecordJane PhamNo ratings yet
- #F2F Student FormsDocument15 pages#F2F Student FormsMarlyn Dimatatac PanopioNo ratings yet
- Figure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupDocument2 pagesFigure 1. Recommended Immunization Schedule For Adults Aged 19 Years or Older, by Vaccine and Age GroupmsarasNo ratings yet
- Immunization Letter NB FORM RevisedDocument6 pagesImmunization Letter NB FORM RevisedUddhavendra Pal SinghNo ratings yet
- HE Form - 2011Document2 pagesHE Form - 2011peter1234uNo ratings yet
- Certificate of Immunization FormDocument1 pageCertificate of Immunization FormShaikahamedNo ratings yet
- Vaccination Requirements of IFMSA Exchange Progam in Israel-9.15Document2 pagesVaccination Requirements of IFMSA Exchange Progam in Israel-9.15Niko DobrilovicNo ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- Points To Remember in Cold Chain ManagementDocument6 pagesPoints To Remember in Cold Chain Managementpaul arvie violetaNo ratings yet
- 2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12Document4 pages2014-2015 Texas Minimum State Vaccine Requirements For Students Grades K-12James AllenNo ratings yet
- Sequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDocument2 pagesSequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDonnaNo ratings yet
- MeningococcalDocument2 pagesMeningococcalLuai Sammy Abu-RayyanNo ratings yet
- Different COVID-19 VaccinesDocument3 pagesDifferent COVID-19 Vaccinesfsese05722No ratings yet
- Immunization Requirement - Student Health Center - The University of UtahDocument2 pagesImmunization Requirement - Student Health Center - The University of Utahmithun916No ratings yet
- Adult ScheduleDocument3 pagesAdult ScheduledrmanojvimalNo ratings yet
- East Tennessee State Univer Meningococcal Meningitis and Hepatitis B Vaccine WaiverDocument1 pageEast Tennessee State Univer Meningococcal Meningitis and Hepatitis B Vaccine WaiverDonnaNo ratings yet
- Factsheet priorCOVID19infection ENGDocument5 pagesFactsheet priorCOVID19infection ENGVasilije MunjasNo ratings yet
- SOP For Retest of Raw MaterialsDocument3 pagesSOP For Retest of Raw MaterialsRainMan75100% (1)
- A Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)Document14 pagesA Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)asma khanNo ratings yet
- Navpers 18068F U.S. Navy Enlisted Classification Manual April 2012Document1,612 pagesNavpers 18068F U.S. Navy Enlisted Classification Manual April 2012VietVetSteve100% (1)
- Health and Safety FCX-HS34Document3 pagesHealth and Safety FCX-HS34berry trisnamuktiNo ratings yet
- Worksheet No.3: Grade 10Document5 pagesWorksheet No.3: Grade 10melvin ynionNo ratings yet
- Reading Comprehension Class 12 CbseDocument4 pagesReading Comprehension Class 12 CbseCbse AccountNo ratings yet
- AV eIFU 10223671 Mg-En V03Document68 pagesAV eIFU 10223671 Mg-En V03Goutham RevuruNo ratings yet
- Final Research Paper 2Document9 pagesFinal Research Paper 2api-510720092No ratings yet
- Committee 2020, Reporter, May Edition 2020, April 24, 2020Document32 pagesCommittee 2020, Reporter, May Edition 2020, April 24, 2020ucopresident_2130533No ratings yet
- Smallholder Vegetable Packhouses: Establishing and ManagingDocument50 pagesSmallholder Vegetable Packhouses: Establishing and ManagingMeet ShahNo ratings yet
- I. Sparq Manufacturing Management Department: Itec854 Danial Bavi / Id: 45485348Document6 pagesI. Sparq Manufacturing Management Department: Itec854 Danial Bavi / Id: 45485348fawas hamdiNo ratings yet
- Drug StudyDocument7 pagesDrug StudyKynaWeeNo ratings yet
- New Graduate RN Cover Letter SamplesDocument7 pagesNew Graduate RN Cover Letter Samplesf60pk9dc100% (3)
- 3 - Safety Plan (KH&B Co.,Ltd.)Document30 pages3 - Safety Plan (KH&B Co.,Ltd.)Wint PaingNo ratings yet
- Assignment in Advance ReadingDocument3 pagesAssignment in Advance ReadingJessa CaberteNo ratings yet
- Hy-Line Silver Brown Commercial Performance Standards ManualDocument16 pagesHy-Line Silver Brown Commercial Performance Standards Manualthanh ba matNo ratings yet
- Efect and Longevity of Botulinum Toxin in The Treatment of Gummy Smile - A Meta Analysis and Meta Regression - Zengiski, 2021Document9 pagesEfect and Longevity of Botulinum Toxin in The Treatment of Gummy Smile - A Meta Analysis and Meta Regression - Zengiski, 2021Rafael Autran Cavalcante AraújoNo ratings yet
- Solid Waste Management: M. Sc. Environmental Science Central University of RajasthanDocument21 pagesSolid Waste Management: M. Sc. Environmental Science Central University of RajasthanAvrenim Magaro DecanoNo ratings yet
- SLS Ginopol L24 151-21-3-MSDS US-GHSDocument8 pagesSLS Ginopol L24 151-21-3-MSDS US-GHSRG TNo ratings yet
- CPR WebDocument222 pagesCPR WebANo ratings yet
- Poison StandardDocument661 pagesPoison StandardmhutchzNo ratings yet
- 20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnDocument161 pages20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnNgọc HuyềnNo ratings yet
- Review On Inflammatory DisesesDocument21 pagesReview On Inflammatory Disesesdigitalmazdoor5201No ratings yet
- Annex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Document4 pagesAnnex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Yeoh Zi-NingNo ratings yet
- Nurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationDocument4 pagesNurs FPX 4050 Assessment 2 Ethical and Policy Factors in Care CoordinationEmma WatsonNo ratings yet
- Cellular Respiration LabDocument6 pagesCellular Respiration Labianzhou1No ratings yet
- Social Work Processes and MethodsDocument32 pagesSocial Work Processes and MethodsAaron Jay ZuluetaNo ratings yet
- 1842 13404 1 SMDocument7 pages1842 13404 1 SMnanda wildaNo ratings yet