Download as pdf or txt
You might also like
- 2023 Par-Q+Document2 pages2023 Par-Q+Lyca Cortes II100% (1)
- GHS Health Declaration Form PDFDocument2 pagesGHS Health Declaration Form PDFFattah AfawNo ratings yet
- Health Statement (G-42) Form (Dependent) - SONDocument1 pageHealth Statement (G-42) Form (Dependent) - SONMd. Shihab HossainNo ratings yet
- Health Statement (G-42) Form (Standard Employee)Document1 pageHealth Statement (G-42) Form (Standard Employee)Rahman AnisurNo ratings yet
- Health Insurance StatementDocument8 pagesHealth Insurance StatementHaronymous Aaron BreaultNo ratings yet
- Declaration of Good Heath: Ddmmy YYYDocument2 pagesDeclaration of Good Heath: Ddmmy YYYindu chauhanNo ratings yet
- Declaration Good Health Form PDFDocument2 pagesDeclaration Good Health Form PDFMurali SiddarthNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsMaria JessaNo ratings yet
- Survey Questionnaire 5-30-2013 FORM (Final) - DistributedDocument6 pagesSurvey Questionnaire 5-30-2013 FORM (Final) - Distributedom parkashNo ratings yet
- COVID19 Vaccine Administration Form Rev 9222Document2 pagesCOVID19 Vaccine Administration Form Rev 9222Amín CarrilloNo ratings yet
- Declaration of Good Health Form PDFDocument3 pagesDeclaration of Good Health Form PDFvemula shekar100% (1)
- Proposal Form Individual Medical InsuranceDocument3 pagesProposal Form Individual Medical InsurancekrishnaNo ratings yet
- Ged00015 Rasheedreuel Nolasco ParqDocument2 pagesGed00015 Rasheedreuel Nolasco ParqRasheed NolascoNo ratings yet
- ReligareDocument2 pagesReligaresanjay thapliyalNo ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- Identifying Information and Healthcare Provider (For Child Patient)Document9 pagesIdentifying Information and Healthcare Provider (For Child Patient)Prabha GuptaNo ratings yet
- Certificate of InsurabilityDocument3 pagesCertificate of InsurabilityDharmendra PalNo ratings yet
- Individual Health Application FormDocument2 pagesIndividual Health Application FormRalph Wamae0% (1)
- DGH Form 1 Fillable v7Document4 pagesDGH Form 1 Fillable v7SovNo ratings yet
- Aviva 4Document4 pagesAviva 4Rahul KumarNo ratings yet
- Vaccine Administration Record (VAR) - Informed Consent For VaccinationDocument2 pagesVaccine Administration Record (VAR) - Informed Consent For VaccinationHilda LunaNo ratings yet
- WWW - Csc.gov - PH: Additional RequirementsDocument4 pagesWWW - Csc.gov - PH: Additional RequirementsJaj EscNo ratings yet
- OnlineRevivalDGH 180124Document7 pagesOnlineRevivalDGH 180124AJAYNo ratings yet
- Medical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)Document3 pagesMedical Application Form: Name Relation (E/S/C) D. O. B SEX (M/F) Marital Status Height (CM) Weight (KG) Emirates (VISA)cmthebossNo ratings yet
- Envelope - Medical Application Form - New - V3 - Mednet - 1Document3 pagesEnvelope - Medical Application Form - New - V3 - Mednet - 1muhdm7771No ratings yet
- Eapps Health StartDocument6 pagesEapps Health StartRegine CaspilloNo ratings yet
- FLast - 6 MedStaff Applicant Declaration (6009) SignedDocument2 pagesFLast - 6 MedStaff Applicant Declaration (6009) SignedCold NoduleNo ratings yet
- FLast - 6 MedStaff Applicant Declaration (6009) SignedDocument2 pagesFLast - 6 MedStaff Applicant Declaration (6009) SignedCold NoduleNo ratings yet
- Patient'S ProfileDocument17 pagesPatient'S ProfileLucas JelmarNo ratings yet
- Given Name Field - Surname Field - 1234566 - DB Comments-V1Document5 pagesGiven Name Field - Surname Field - 1234566 - DB Comments-V1sunny tiwariNo ratings yet
- Medical Declaration Form: Family History of The ApplicantDocument3 pagesMedical Declaration Form: Family History of The ApplicantJae WaiNo ratings yet
- Global Health Employee Application Form (Underwritten)Document4 pagesGlobal Health Employee Application Form (Underwritten)rudolfh1309No ratings yet
- Parqplus 2020Document6 pagesParqplus 2020klinikcitrautamapalembangNo ratings yet
- Health Questionnaire: MohamadDocument2 pagesHealth Questionnaire: MohamadMoh AmmNo ratings yet
- Medical Application FormDocument3 pagesMedical Application FormBogdan Brdar100% (1)
- Par Q FormDocument2 pagesPar Q FormLejinNo ratings yet
- General Health Questions: The Physical Activity Readiness Questionnaire For StudentsDocument2 pagesGeneral Health Questions: The Physical Activity Readiness Questionnaire For Students202310350No ratings yet
- DoGH FormDocument2 pagesDoGH FormcoolgrassNo ratings yet
- New Patient Registration FormDocument4 pagesNew Patient Registration Formapi-358908929No ratings yet
- DSMES Assessment Template (Chart 7)Document5 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Health Questionnaire Form EnglishDocument1 pageHealth Questionnaire Form EnglishAhsan ShafiqueNo ratings yet
- Prulife Uk Form PiDocument3 pagesPrulife Uk Form PiPaulie TitoNo ratings yet
- Employee Health Evaluation & Enrollment Form: Corporate Solutions IncorporatedDocument2 pagesEmployee Health Evaluation & Enrollment Form: Corporate Solutions IncorporatedMitchell BigleyNo ratings yet
- Uw Autism Center Intake Packet: What Are Your Primary Patient Concerns? Please Be SpecificDocument10 pagesUw Autism Center Intake Packet: What Are Your Primary Patient Concerns? Please Be SpecificPrabha GuptaNo ratings yet
- Par QDocument2 pagesPar Qaicel sagaNo ratings yet
- Declaration of Good Health Form - With Covid QDocument2 pagesDeclaration of Good Health Form - With Covid QRajnish YadavNo ratings yet
- Physical Exam Form IHSAADocument2 pagesPhysical Exam Form IHSAASattagrace HarrisNo ratings yet
- Medical FormDocument1 pageMedical FormCarlos SegoviaNo ratings yet
- Medical Application Form (New) - V3-2021!10!12 - RAKDocument3 pagesMedical Application Form (New) - V3-2021!10!12 - RAKAnkita NiravNo ratings yet
- Application For Reinstatement of Plan Agreement (Revised As of July 21, 2021)Document3 pagesApplication For Reinstatement of Plan Agreement (Revised As of July 21, 2021)Cathylyn LacadinNo ratings yet
- Client Screening Website FormDocument2 pagesClient Screening Website FormBrett Whipp100% (2)
- Declaration of Good Health Form NewDocument3 pagesDeclaration of Good Health Form NewBalu PollachiNo ratings yet
- Name (In Full) Date of Birth Gender Male / Female Blood Group Physical Disability, If Any Kindly Answer All The Following QuestionsDocument2 pagesName (In Full) Date of Birth Gender Male / Female Blood Group Physical Disability, If Any Kindly Answer All The Following QuestionsVikranth VeeraNo ratings yet
- NUTP Health Declaration FormDocument2 pagesNUTP Health Declaration FormCik GeeNo ratings yet
- DiabetesDocument2 pagesDiabetessudhanshugst123No ratings yet
- Sukoon New MAFDocument5 pagesSukoon New MAFJdNo ratings yet
- Chaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportDocument2 pagesChaitanya Godavari Grameena Bank:: Head Office:: Guntur Medical Examination ReportbajibabuNo ratings yet
- Physical Activity Readiness Questionnaire (PAR Q) : When Using This Form, You Need To StateDocument3 pagesPhysical Activity Readiness Questionnaire (PAR Q) : When Using This Form, You Need To StateF-dawgNo ratings yet
- Reon Energy Solution Health Status Questionnare (HSQ)Document2 pagesReon Energy Solution Health Status Questionnare (HSQ)arbab201No ratings yet
- Detecting & Living with Breast Cancer For DummiesFrom EverandDetecting & Living with Breast Cancer For DummiesRating: 1 out of 5 stars1/5 (1)
- Narrative Perspective AFDocument1 pageNarrative Perspective AFAngel AndersonNo ratings yet
- 16marks HTM PDFDocument5 pages16marks HTM PDFJ.R.Vinod KumaarNo ratings yet
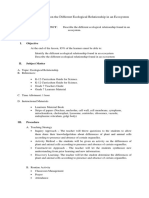
- Detailed Lesson Plan On FungiDocument3 pagesDetailed Lesson Plan On FungiMae Amor EnorioNo ratings yet
- HRM Practices at Indian Oil CorporationDocument16 pagesHRM Practices at Indian Oil CorporationAditi BhadouriaNo ratings yet
- 2023 SMO Results DetailsDocument4 pages2023 SMO Results Details9hfm97v5j5No ratings yet
- Y Varies Directly As X and Inversely As Z". Varies Directly As X and Inversely As Z"Document4 pagesY Varies Directly As X and Inversely As Z". Varies Directly As X and Inversely As Z"Rey Angelica Garcia TampusNo ratings yet
- Aloof Personality TraitsDocument4 pagesAloof Personality TraitsManasi DasNo ratings yet
- Unjust Enrichment McInnesDocument78 pagesUnjust Enrichment McInnesYang WangNo ratings yet
- Excuses PDFDocument5 pagesExcuses PDFUlisses PiassaNo ratings yet
- Datuin and Zarco Ecoframe Landslides Sept2019Document49 pagesDatuin and Zarco Ecoframe Landslides Sept2019Isaiah Emmanuel SuguitanNo ratings yet
- LDC - 2017 Cutoff and Advice DetailsDocument1 pageLDC - 2017 Cutoff and Advice DetailsAghor GamingNo ratings yet
- Celiac Disease Diagnostic Testing AlgorithmDocument1 pageCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakNo ratings yet
- Case Concerning Electronica SiculaDocument9 pagesCase Concerning Electronica SiculaasepkusnaliNo ratings yet
- Anti-Sexual Harrassment ActDocument30 pagesAnti-Sexual Harrassment ActJ Velasco PeraltaNo ratings yet
- Configuracion de BMR Boot Server RHEL 56Document482 pagesConfiguracion de BMR Boot Server RHEL 56Adalberto Blanco MejiaNo ratings yet
- Graha YuddhaDocument10 pagesGraha YuddhaHeather WilliamsNo ratings yet
- Bee Agskills - NSW DPIDocument10 pagesBee Agskills - NSW DPIRick3862No ratings yet
- Pidilite Internship Report - SalesDocument28 pagesPidilite Internship Report - SalesAnuragNo ratings yet
- Urea Cycle DisordersDocument23 pagesUrea Cycle DisordersIsabela BurculetNo ratings yet
- MCS052Document8 pagesMCS052AasNo ratings yet
- Normal Carbohydrate Balance and Maintenance of Blood Glucose LevelsDocument2 pagesNormal Carbohydrate Balance and Maintenance of Blood Glucose LevelsSig G. MiNo ratings yet
- Landi Kotal To Wagah Reading SampleDocument28 pagesLandi Kotal To Wagah Reading SampleAafi SyedNo ratings yet
- Lord's SupperDocument1 pageLord's SupperJesus LivesNo ratings yet
- A Guide To Confidentiality in Health and Social CareDocument6 pagesA Guide To Confidentiality in Health and Social CareSergio Antonio Morales SarmientoNo ratings yet
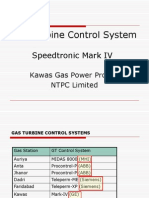
- Gas Turbine Control System1 - NemaDocument50 pagesGas Turbine Control System1 - Nemaveerclaire100% (1)
- 19BCS4030 Final ReportDocument107 pages19BCS4030 Final ReportShivang ChandaNo ratings yet
- A Comprehensive Literature Review On Construction Project Risk Analysis PDFDocument16 pagesA Comprehensive Literature Review On Construction Project Risk Analysis PDFAsif HameedNo ratings yet
- Cop Practical Book 6Document75 pagesCop Practical Book 6DanielleMuntyanNo ratings yet
- Plantillas Odoo Leah Beauty & Boutique (Productos y Usuarios)Document85 pagesPlantillas Odoo Leah Beauty & Boutique (Productos y Usuarios)Policarpio LazalaNo ratings yet
- DG Reporting VFDocument2 pagesDG Reporting VFRamani DantuluriNo ratings yet