Download as pdf or txt
You might also like
- Drug StudyDocument8 pagesDrug StudyJoshua VillarbaNo ratings yet
- Clinical Case Report Powerpoint PresentationDocument24 pagesClinical Case Report Powerpoint Presentationapi-354139540100% (1)
- Toovey 2007Document22 pagesToovey 2007fissionmailedNo ratings yet
- RabiesDocument25 pagesRabiesAdindapauliaNo ratings yet
- 1 Immunization جمعت كل مهم هناDocument13 pages1 Immunization جمعت كل مهم هناReem 10No ratings yet
- Public Health RabbiesDocument3 pagesPublic Health Rabbiesrobertkani2004No ratings yet
- Medical Virology Dr. Saif AL-Mayah: Rabies Virus Disease:This Virus Causes Rabies. Important PropertiesDocument9 pagesMedical Virology Dr. Saif AL-Mayah: Rabies Virus Disease:This Virus Causes Rabies. Important PropertiesAtheer AlabdyNo ratings yet
- 3 Vaccines 2022 EnglishDocument28 pages3 Vaccines 2022 EnglishVlad SmithNo ratings yet
- Rhabdoviridae: Rabies VirusDocument13 pagesRhabdoviridae: Rabies Virusميمونه عبد الرحيم مصطفىNo ratings yet
- Rabies 151018135758 Lva1 App6892 PDFDocument44 pagesRabies 151018135758 Lva1 App6892 PDFAna SismanNo ratings yet
- Reviewer 2.3c - VaccinesDocument3 pagesReviewer 2.3c - VaccinesCyrene ManansalaNo ratings yet
- Is Hospital Mortality Higher at Weekends? If So, Why?: CommentDocument4 pagesIs Hospital Mortality Higher at Weekends? If So, Why?: CommentRatna KusumasariNo ratings yet
- 1 s2.0 S0264410X13004003 MainDocument4 pages1 s2.0 S0264410X13004003 MainDiego TulcanNo ratings yet
- Alpha-C-galactosylceramide As An Adjuvant For A Live Attenuated in Uenza Virus VaccineDocument9 pagesAlpha-C-galactosylceramide As An Adjuvant For A Live Attenuated in Uenza Virus VaccineLeandro CarreñoNo ratings yet
- Rabies and Intradermal Rabies Vaccination: Alan C. Jackson, MDDocument32 pagesRabies and Intradermal Rabies Vaccination: Alan C. Jackson, MDLemuel GuevarraNo ratings yet
- Recent Trends in Viral VaccinesDocument64 pagesRecent Trends in Viral VaccinesAkula Sai PrasannaNo ratings yet
- Feline Rhinotracheitis-Calici-Panleukopenia Vaccine: Modified Live VirusDocument1 pageFeline Rhinotracheitis-Calici-Panleukopenia Vaccine: Modified Live VirusFeni AprianiNo ratings yet
- WHO Rabies PDFDocument5 pagesWHO Rabies PDFJulian HuningkorNo ratings yet
- DouglasDocument3 pagesDouglasLINGGA DEWINo ratings yet
- Rabies: Lyssa Virus. Genus Name of RhabdoviridaeDocument3 pagesRabies: Lyssa Virus. Genus Name of RhabdoviridaeFhaye LitucoNo ratings yet
- ImmunisationDocument42 pagesImmunisationDr. Ajeta GuptaNo ratings yet
- RabiesDocument48 pagesRabiesSarah AliNo ratings yet
- Prof. Mochammad Hatta. MD, PHD, SPMK (K) Molecular Biology and Immunology Laboratory, Hasanuddin University, IndonesiaDocument11 pagesProf. Mochammad Hatta. MD, PHD, SPMK (K) Molecular Biology and Immunology Laboratory, Hasanuddin University, IndonesiaRahmawati HamudiNo ratings yet
- Anti-Viral ChemotherapyDocument39 pagesAnti-Viral Chemotherapyjolan.freedomNo ratings yet
- 3.03.12 IbdDocument23 pages3.03.12 Ibdmeghayadav.businessNo ratings yet
- WHO - RabiesDocument5 pagesWHO - RabiesSatish Kumar DashNo ratings yet
- Disease PreventionDocument15 pagesDisease PreventionFashion CollectionNo ratings yet
- Review Article A Detail Comprehensive Review On VaccinesDocument9 pagesReview Article A Detail Comprehensive Review On VaccinesKarthika KrishnanNo ratings yet
- 8 A Potent Neutralizing Antibody With Therapeutic PotentialDocument10 pages8 A Potent Neutralizing Antibody With Therapeutic Potentialrommelbasket08No ratings yet
- RabiesDocument28 pagesRabiesrouhanbinrashidNo ratings yet
- L) Resolved by Hospital Day 6. No Other: From The Centers For Disease Control and PreventionDocument3 pagesL) Resolved by Hospital Day 6. No Other: From The Centers For Disease Control and Preventionatika sgrtNo ratings yet
- Ebola, Rubella AndRabiesDocument37 pagesEbola, Rubella AndRabiesmulatumeleseNo ratings yet
- Rabies GuidelinesDocument21 pagesRabies Guidelineslotski100% (2)
- 0506hoENTEROVIRAL INFECTIONSDocument57 pages0506hoENTEROVIRAL INFECTIONSAmandeep SinghNo ratings yet
- Induces Long Lasting Intracellular Replication-Deficient: Leishmania DonovaniDocument9 pagesInduces Long Lasting Intracellular Replication-Deficient: Leishmania DonovanimclimacoNo ratings yet
- Inverse Vaccination, The Opposite of Jenner's Concept, For Therapy of AutoimmunityDocument11 pagesInverse Vaccination, The Opposite of Jenner's Concept, For Therapy of AutoimmunityAna Paula MartinsNo ratings yet
- VITALSIGNSIMMUNIZATIONDocument6 pagesVITALSIGNSIMMUNIZATIONGlaiza Mae TuralbaNo ratings yet
- PIIS0085253821003483Document3 pagesPIIS0085253821003483Bala MuraliNo ratings yet
- Distemper en PerrosDocument6 pagesDistemper en PerrosAlexandra GuerreroNo ratings yet
- Immunization - Dr. SarahDocument14 pagesImmunization - Dr. Sarahf6bk6xnppyNo ratings yet
- Rabies Menurut Inet MscapehDocument8 pagesRabies Menurut Inet MscapehenvadNo ratings yet
- Communicable Disease (Introduction Part 2) : Period of DeclineDocument6 pagesCommunicable Disease (Introduction Part 2) : Period of Declinefiel borataNo ratings yet
- Pichichero2009 - AntibodyDocument11 pagesPichichero2009 - AntibodyPatrícia KellenNo ratings yet
- 5 - Group 1 - Infectious DiseaseDocument58 pages5 - Group 1 - Infectious DiseaseEarle NiervoNo ratings yet
- Newcastle Disease: C H A P T E R 2 - 3 - 1 4Document14 pagesNewcastle Disease: C H A P T E R 2 - 3 - 1 4Roby R. AryoputrantoNo ratings yet
- Animal BitesDocument10 pagesAnimal BitesWilly WizeNo ratings yet
- Rabies VaccineDocument12 pagesRabies VaccineRONAK LASHKARINo ratings yet
- 2.03.14 Newcastle DisDocument14 pages2.03.14 Newcastle DisdiparayogagalihNo ratings yet
- Neonatal Varicella: PediatricsDocument5 pagesNeonatal Varicella: Pediatricsnoval rafsanjaniNo ratings yet
- Sheen Ann John 1st Year PG Dept of PedodonticsDocument68 pagesSheen Ann John 1st Year PG Dept of PedodonticsSri MareesNo ratings yet
- Post-Exposure Prophylaxis (PEP) : Rabies Exposure May Be Classified As Per WHO Into Three CategoriesDocument7 pagesPost-Exposure Prophylaxis (PEP) : Rabies Exposure May Be Classified As Per WHO Into Three CategoriesPramod KumarNo ratings yet
- Rabies: NAME: Duaa Amer Abed U.O.A C.O.PharmacyDocument8 pagesRabies: NAME: Duaa Amer Abed U.O.A C.O.PharmacyTee bagNo ratings yet
- Prelims - GMJ Lecture - Module 2 III DisorderDocument3 pagesPrelims - GMJ Lecture - Module 2 III DisorderjuiceNo ratings yet
- Rabies: Prophylaxis If The Animal Can BeDocument1 pageRabies: Prophylaxis If The Animal Can BeAlna Shelah IbañezNo ratings yet
- Covid JournalDocument8 pagesCovid JournalwilverNo ratings yet
- MMR ImmunizationDocument43 pagesMMR ImmunizationkukuruziNo ratings yet
- ZoonosisDocument27 pagesZoonosisSingh BhujangiNo ratings yet
- 1 s2.0 S0213005X19302101Document3 pages1 s2.0 S0213005X19302101A MFNo ratings yet
- Imunisasi: Bambang MulyawanDocument60 pagesImunisasi: Bambang Mulyawanmentarimen19No ratings yet
- Principles of ImmunizationDocument4 pagesPrinciples of ImmunizationDoc Prince CaballeroNo ratings yet
- Wikipedia - Epididymitis (CHECKED)Document6 pagesWikipedia - Epididymitis (CHECKED)pixoguiasNo ratings yet
- Considerations On The Use of Neonatal and Pediatric ResuscitationDocument15 pagesConsiderations On The Use of Neonatal and Pediatric ResuscitationrsmitrahuadaNo ratings yet
- Breast CancerDocument68 pagesBreast Cancerapi-3748365100% (4)
- Ankur Jindal Curriculum VitaeDocument15 pagesAnkur Jindal Curriculum VitaeManoj KumarNo ratings yet
- Canavalia Gladiata On Peptic UlcerDocument3 pagesCanavalia Gladiata On Peptic UlcerspandanaNo ratings yet
- Care of The Unconscious, Multi-Trauma PatientDocument37 pagesCare of The Unconscious, Multi-Trauma PatientRomaine BarrettNo ratings yet
- Comprehensive Report On Rapid Plasma Reagin Test (RPR)Document3 pagesComprehensive Report On Rapid Plasma Reagin Test (RPR)Kim RuizNo ratings yet
- Hartalega Extreme Gloves - Sell Sheet - Colloidal Oatmeal Coated Nitrile Powder Free 2.5 MilDocument1 pageHartalega Extreme Gloves - Sell Sheet - Colloidal Oatmeal Coated Nitrile Powder Free 2.5 Milmfidae_210808925No ratings yet
- Your Arthroscopic Shoulder Surgery,: A Helpful GuideDocument12 pagesYour Arthroscopic Shoulder Surgery,: A Helpful GuideAle XyyNo ratings yet
- Non Malignant DiseasesDocument36 pagesNon Malignant DiseasesshokoNo ratings yet
- OliclinomelDocument11 pagesOliclinomelDevarajan Melpanaiyur SowmyanarayananNo ratings yet
- Blood Vessel and Lymphatic Lab OutputDocument12 pagesBlood Vessel and Lymphatic Lab OutputDayledaniel SorvetoNo ratings yet
- PPH PosterDocument1 pagePPH PosterKhaled Gaber SabaaNo ratings yet
- Op GhaiDocument9 pagesOp GhaiParth MittalNo ratings yet
- Nursing Care Plan: RationaleDocument3 pagesNursing Care Plan: Rationaleimnas100% (1)
- Nursing BulletsDocument73 pagesNursing BulletsJanine Anjenette Sibayan100% (7)
- Rajkumari Amrit Kaur College of Nursing: Lesson Plan On Infection Prevention and Control MeasuresDocument18 pagesRajkumari Amrit Kaur College of Nursing: Lesson Plan On Infection Prevention and Control MeasuresIshwar Das100% (2)
- 10 Common Elderly Health IssuesDocument12 pages10 Common Elderly Health Issuessweetsai05No ratings yet
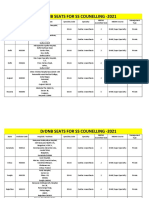
- Final DRDNB Seats For SS Counselling 2021Document152 pagesFinal DRDNB Seats For SS Counselling 2021Pavan KumarNo ratings yet
- DOH Administrative Order No 2024 0043Document44 pagesDOH Administrative Order No 2024 0043Jasper John HerreraNo ratings yet
- AssignmentDocument7 pagesAssignmentAkilesh MNo ratings yet
- TD Vaccine Operational GuidelinesDocument2 pagesTD Vaccine Operational GuidelinesSiddhartha NandiNo ratings yet
- Imaging The MediastinumDocument55 pagesImaging The Mediastinumcheeze_8No ratings yet
- PR076 RIQAS Monthly Calendar NOV1Document28 pagesPR076 RIQAS Monthly Calendar NOV1PannaMkNo ratings yet
- Circulating Case Slip: Name of Student Student NumberDocument12 pagesCirculating Case Slip: Name of Student Student NumberEugenio Roque Casaclang De Leon IiiNo ratings yet
- Complications in Children With Percutaneous Endoscopic Gastrostomy (PEG) PlacementDocument5 pagesComplications in Children With Percutaneous Endoscopic Gastrostomy (PEG) PlacementHenry BarberenaNo ratings yet
- AJGP 05 2021 Clinical Sweetman Step by Step Model Brief WEB 2Document7 pagesAJGP 05 2021 Clinical Sweetman Step by Step Model Brief WEB 2alex.ttkNo ratings yet
- Obstetric Hemorrhage: by CC Nadine D. BacalangcoDocument87 pagesObstetric Hemorrhage: by CC Nadine D. BacalangcoNadine BacalangcoNo ratings yet
- Tuoren Price List (2022 Dec)Document5 pagesTuoren Price List (2022 Dec)satan ghostNo ratings yet