Download as pdf or txt
You might also like
- Design and Application of The Worm GearDocument259 pagesDesign and Application of The Worm GearVero Felo100% (2)
- HR Manager RACI MAtrixDocument2 pagesHR Manager RACI MAtrixDigendra Rathore50% (2)
- Leyland HA6ETI Service ManualDocument72 pagesLeyland HA6ETI Service ManualPolavarapu Sreedhar100% (4)
- A Systematic Review of The Outcomes of Posterolateral Corner Knee Injuries Part 2Document9 pagesA Systematic Review of The Outcomes of Posterolateral Corner Knee Injuries Part 2cesarmgaytanmedinaNo ratings yet
- Getgood2016 231016 153128Document11 pagesGetgood2016 231016 153128Cristian SanchezNo ratings yet
- Am J Sports Med 2014 Albrecht 59 69Document12 pagesAm J Sports Med 2014 Albrecht 59 69liminNo ratings yet
- (2016) Running and Knee Osteoarthritis - A Systematic Review and Meta-AnalysisDocument12 pages(2016) Running and Knee Osteoarthritis - A Systematic Review and Meta-Analysiscalixto1995No ratings yet
- Ekhtiari 2017Document9 pagesEkhtiari 2017QuiroprácticaParaTodosNo ratings yet
- Medicine The American Journal of SportsDocument6 pagesMedicine The American Journal of Sportslite.trawler-0xNo ratings yet
- Vergelijking Versneld Vs NT Versneld Revalidatie Na ACLDocument14 pagesVergelijking Versneld Vs NT Versneld Revalidatie Na ACLEllen&Koen WalravensNo ratings yet
- BMAC, MSC For Knee OsteoarthritisDocument11 pagesBMAC, MSC For Knee OsteoarthritisMrinalini SinghNo ratings yet
- Medicine The American Journal of Sports: Diagnosis of Acute Groin Injuries: A Prospective Study of 110 AthletesDocument9 pagesMedicine The American Journal of Sports: Diagnosis of Acute Groin Injuries: A Prospective Study of 110 AthletesomingNo ratings yet
- Adipose Derived Stromal Cell (ADSC) Injections For Pain Management of Osteoarthritis in The Human Knee JointDocument8 pagesAdipose Derived Stromal Cell (ADSC) Injections For Pain Management of Osteoarthritis in The Human Knee JointBrandaNo ratings yet
- Adnan's SynopsisDocument15 pagesAdnan's Synopsisadnanmahboob83No ratings yet
- Clinically Significant Outcomes After Meniscectomy 2019Document12 pagesClinically Significant Outcomes After Meniscectomy 2019asmaNo ratings yet
- Systematic ReviewDocument7 pagesSystematic ReviewErwin WibowoNo ratings yet
- Clinical Outcomes After Anterior Cruciate Ligament Injury - PantheDocument21 pagesClinical Outcomes After Anterior Cruciate Ligament Injury - PantheOlga SeregNo ratings yet
- Thesis On Bone CancerDocument5 pagesThesis On Bone Cancerkvpyqegld100% (2)
- Medicine The American Journal of SportsDocument7 pagesMedicine The American Journal of SportsJohann Sebastian CruzNo ratings yet
- Rotator Cuff Degeneration Etiology and PathogenesisDocument9 pagesRotator Cuff Degeneration Etiology and PathogenesisNur Hasri IndahsariNo ratings yet
- Adnan's SynopsisDocument16 pagesAdnan's Synopsisadnanmahboob83No ratings yet
- Pedley Et Al. 2020 - Revisão Sistemática - Saltos - Cinética e CinemáticaDocument18 pagesPedley Et Al. 2020 - Revisão Sistemática - Saltos - Cinética e CinemáticaFábio LanferdiniNo ratings yet
- Timing of Rehabilitation On Length of Stay and Cost in Patients With Hip or Knee Joint Arthroplasty: A Systematic Review With Meta-AnalysisDocument22 pagesTiming of Rehabilitation On Length of Stay and Cost in Patients With Hip or Knee Joint Arthroplasty: A Systematic Review With Meta-AnalysisskNo ratings yet
- 2010 Mars Group Descriptive Epidemiology of The Multicenter ACL Revision Study (MARS) CohortDocument8 pages2010 Mars Group Descriptive Epidemiology of The Multicenter ACL Revision Study (MARS) CohortArmin ParavlićNo ratings yet
- Arthroscopic Meniscus Allograft Transplantation in Male Professional Soccer Players. 2013.Document8 pagesArthroscopic Meniscus Allograft Transplantation in Male Professional Soccer Players. 2013.GuilhermeAndradeNo ratings yet
- Lim 2017Document10 pagesLim 2017Juliana Gomes BarretoNo ratings yet
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDocument21 pagesThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-Analysisilham Maulana ArifNo ratings yet
- Kamei 2013Document11 pagesKamei 2013ferd dinanNo ratings yet
- AmJSportsMed 2015 Khayambashi 0363546515616237Document9 pagesAmJSportsMed 2015 Khayambashi 0363546515616237Aurimas MintaučkisNo ratings yet
- Prospect of Stem Cells Conditioned Medium (Secretome) in Ligament and Tendon Healing: A Systematic ReviewDocument8 pagesProspect of Stem Cells Conditioned Medium (Secretome) in Ligament and Tendon Healing: A Systematic ReviewMuhammad RifqoNo ratings yet
- ACL Injuries in The Female Athlete: Causes, Impacts, and Conditioning Programs Frank R. Noyes Sue Barber-WestinDocument658 pagesACL Injuries in The Female Athlete: Causes, Impacts, and Conditioning Programs Frank R. Noyes Sue Barber-WestinluizamgoNo ratings yet
- Clinics in Sports MedicineDocument202 pagesClinics in Sports MedicineAndres Sanchez EscobedoNo ratings yet
- Choi 2021Document12 pagesChoi 2021paul_androideNo ratings yet
- 30 Mekanisme WastingDocument61 pages30 Mekanisme WastingArmi ZakaNo ratings yet
- Research Paper OsteoarthritisDocument8 pagesResearch Paper Osteoarthritisc9snjtdx100% (1)
- Treatment of Osteoarthritis of The Knee With Bracing: A Scoping ReviewDocument7 pagesTreatment of Osteoarthritis of The Knee With Bracing: A Scoping Reviewger80No ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- The Effects of Preoperative Embolization On Carotid Body Paraganglioma Surgery: A Systematic Review and Meta-AnalysisDocument8 pagesThe Effects of Preoperative Embolization On Carotid Body Paraganglioma Surgery: A Systematic Review and Meta-AnalysisNicolás HenaoNo ratings yet
- JTD 2018 ORCWI 14 FinalDocument13 pagesJTD 2018 ORCWI 14 FinalLinh DoanNo ratings yet
- Evidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewDocument9 pagesEvidence-Based Treatment Choices For Acute Lateral Ankle Sprain: A Comprehensive Systematic ReviewMilton RezzaNo ratings yet
- Biologic Agents To Optimize Outcomes Following ACL Repair and Reconstruction A Systematic Review of Clinical EvidenceDocument38 pagesBiologic Agents To Optimize Outcomes Following ACL Repair and Reconstruction A Systematic Review of Clinical EvidenceyasimNo ratings yet
- Selection Criteria For Patients With Chronic AnkleDocument7 pagesSelection Criteria For Patients With Chronic AnkleChristina SuppiahNo ratings yet
- Research Lit ReviewDocument18 pagesResearch Lit Reviewapi-383151067No ratings yet
- Aatika 8Document7 pagesAatika 8Abhishek GuptaNo ratings yet
- 2-29 - Sport - 2009, Vol.28, Issue 2, AllograftsDocument157 pages2-29 - Sport - 2009, Vol.28, Issue 2, AllograftsLucian AlexandruNo ratings yet
- Ankle Distraction Arthroplasty A Survivorship RevDocument9 pagesAnkle Distraction Arthroplasty A Survivorship RevmirandaroydsNo ratings yet
- Lberaçao Capsular Posteror CrurgcaDocument7 pagesLberaçao Capsular Posteror CrurgcaEduardo FilhoNo ratings yet
- Sport Injuries Sustained by Athletes With Disability - A Systematic ReviewDocument13 pagesSport Injuries Sustained by Athletes With Disability - A Systematic Review2psdbwq4zbNo ratings yet
- AAOS Recon 2013Document96 pagesAAOS Recon 2013cooperorthopaedicsNo ratings yet
- Research Proposal FinalDocument12 pagesResearch Proposal Finalapi-662511892No ratings yet
- Classifications in Brief Goutallier ClassificationDocument6 pagesClassifications in Brief Goutallier ClassificationHugo BorboaNo ratings yet
- Assessment of Quadriceps Muscle Thickness Using BedsideDocument9 pagesAssessment of Quadriceps Muscle Thickness Using BedsideJoaquin LopezNo ratings yet
- Singh Et Al (2012)Document7 pagesSingh Et Al (2012)Puri RaharjaNo ratings yet
- A Scoping Review of The Proximal Humerus Fracture LiteratureDocument10 pagesA Scoping Review of The Proximal Humerus Fracture LiteratureIin Novita SariNo ratings yet
- Anterior Cruciate Ligament Reconstruction With HamDocument7 pagesAnterior Cruciate Ligament Reconstruction With Hamich khuyNo ratings yet
- Canadian Academy of Sport and Exercise Medicine.11Document5 pagesCanadian Academy of Sport and Exercise Medicine.11Diego PonceNo ratings yet
- Factors Associated With A Delay in Achieving Full Knee Extension Before Anterior Cruciate Ligament ReconstructionDocument5 pagesFactors Associated With A Delay in Achieving Full Knee Extension Before Anterior Cruciate Ligament ReconstructioniwanNo ratings yet
- Clinical Behavior of Short Dental Implants - Systematic Review and Meta-Analysis. J Clin Med, 2020Document16 pagesClinical Behavior of Short Dental Implants - Systematic Review and Meta-Analysis. J Clin Med, 2020Marlene Kasumi Gantier TakanoNo ratings yet
- Ischemic Therapy in Musculoskeletal Medicine (4939)Document9 pagesIschemic Therapy in Musculoskeletal Medicine (4939)RexDavidGidoNo ratings yet
- Acl Injury Research PaperDocument6 pagesAcl Injury Research Paperrvpchmrhf100% (1)
- Orthodontic Mechanotherapies and Their in Uence On External Root Resorption: A Systematic ReviewDocument17 pagesOrthodontic Mechanotherapies and Their in Uence On External Root Resorption: A Systematic ReviewMarlon Cespedes AlccaNo ratings yet
- Article 4Document10 pagesArticle 4umair muqriNo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- Moen2014 231018 211347Document10 pagesMoen2014 231018 211347Cristian SanchezNo ratings yet
- Abjs-4-204 231018 174928Document9 pagesAbjs-4-204 231018 174928Cristian SanchezNo ratings yet
- Clark2017 231018 152310Document7 pagesClark2017 231018 152310Cristian SanchezNo ratings yet
- 167 2010 Article 1100 231128 225046Document13 pages167 2010 Article 1100 231128 225046Cristian SanchezNo ratings yet
- 0301 620X99B2BJJ 2016 0256R1 - 231018 - 151141Document12 pages0301 620X99B2BJJ 2016 0256R1 - 231018 - 151141Cristian SanchezNo ratings yet
- Ado PVC sunum-ENDocument19 pagesAdo PVC sunum-ENMete RuscukluNo ratings yet
- Disel Tank Stand Frame REPORTDocument15 pagesDisel Tank Stand Frame REPORTSIful Islam ShawonNo ratings yet
- Reeling Self: Subjectivity in FilmsDocument40 pagesReeling Self: Subjectivity in FilmsMęawy MįlkshãkeNo ratings yet
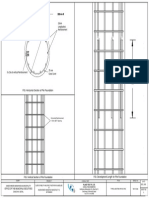
- RCC Pile 500mm-FINAL PRINTDocument1 pageRCC Pile 500mm-FINAL PRINTSushant GiriNo ratings yet
- Financial Planning Using ExcelDocument217 pagesFinancial Planning Using ExcelThomas100% (1)
- The Wonderful World of Chrome Extensions Volume 27Document14 pagesThe Wonderful World of Chrome Extensions Volume 27rajat mehrotraNo ratings yet
- ASTM Cross Reference Chart: Carbon SteelDocument1 pageASTM Cross Reference Chart: Carbon SteelMurat UzunNo ratings yet
- Muhammad Tofiq CV PDFDocument3 pagesMuhammad Tofiq CV PDFJOB 2015No ratings yet
- Section1 For cs50Document90 pagesSection1 For cs50wwwron456No ratings yet
- A Top-Down Approach To Achieving Performance Predictability in Database SystemsDocument47 pagesA Top-Down Approach To Achieving Performance Predictability in Database SystemsvisaobuonNo ratings yet
- Models 3885, 3886, 3887: Installation, Operation and Maintenance InstructionsDocument36 pagesModels 3885, 3886, 3887: Installation, Operation and Maintenance Instructionsjordanron88No ratings yet
- UntitledDocument3 pagesUntitledArchana shuklaNo ratings yet
- Audacity Exercises For Chapter 3Document22 pagesAudacity Exercises For Chapter 3Heather WhiteheadNo ratings yet
- IN1831 001 021422 CheckweigherIPacDocument20 pagesIN1831 001 021422 CheckweigherIPacprakashNo ratings yet
- Service Manual: 20010915-18000 Hamamatsu, JapanDocument19 pagesService Manual: 20010915-18000 Hamamatsu, JapanTvbox 15No ratings yet
- Agricultural Water Management: PrefaceDocument3 pagesAgricultural Water Management: PrefacelinoNo ratings yet
- Class Xii Cs - 10 Sample PapersDocument43 pagesClass Xii Cs - 10 Sample PapersHalfborn GundersonNo ratings yet
- Metashape Pro 1 8 en 14 23Document10 pagesMetashape Pro 1 8 en 14 23ركن علي خالد بواقنه ركن علي خالد بواقنهNo ratings yet
- Cyber Handbook Enterprise Latest Pages DeletedDocument37 pagesCyber Handbook Enterprise Latest Pages DeletedRaghuram CoorgNo ratings yet
- Business Intelligence Assignment 3Document11 pagesBusiness Intelligence Assignment 3Ahmed Chaudhary100% (1)
- Chapter 6 Wireless SecurityDocument8 pagesChapter 6 Wireless SecurityShashant SakhareNo ratings yet
- KB5015684: Featured Update To Windows 10, Version 22H2 by Using An Enablement Package - Microsoft SuDocument1 pageKB5015684: Featured Update To Windows 10, Version 22H2 by Using An Enablement Package - Microsoft SuAllamNo ratings yet
- Assignment 3 Burhanuddin Sikandar Roll No:-1511Document7 pagesAssignment 3 Burhanuddin Sikandar Roll No:-1511Barry AllenNo ratings yet
- Excalibur 7018 MR: Conformances Key FeaturesDocument2 pagesExcalibur 7018 MR: Conformances Key FeaturesAsongwe HansNo ratings yet
- Raspberry Pi 3x3x3 LED Cube Workshop Demo: March 20, 2015Document26 pagesRaspberry Pi 3x3x3 LED Cube Workshop Demo: March 20, 2015Dave TowerNo ratings yet
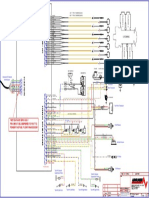
- R3 SV EMS Wiring DiagramDocument1 pageR3 SV EMS Wiring DiagramGreg VosperNo ratings yet
- Ismail O. Ogunlana: Personal DataDocument2 pagesIsmail O. Ogunlana: Personal DataFawazNo ratings yet