Download as pdf or txt
You might also like
- Development of The Nervous System 3rd Edition Sanes Test BankDocument35 pagesDevelopment of The Nervous System 3rd Edition Sanes Test Bankbateddivisor51zwed100% (27)
- Biology Investigatory ProjectDocument14 pagesBiology Investigatory Projectatharva surwase100% (2)
- INFERTILITY Obg SeminarDocument19 pagesINFERTILITY Obg SeminarDelphy VargheseNo ratings yet
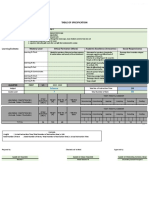
- TOS-Technical DrawingDocument8 pagesTOS-Technical DrawingMarc Angelo L. SebastianNo ratings yet
- Answer Key Intraboard ADocument18 pagesAnswer Key Intraboard AJonas Marvin Anaque100% (4)
- Female Infertility: DR Jaqueline Sudiman, PHDDocument21 pagesFemale Infertility: DR Jaqueline Sudiman, PHDGlorio Absalom PuaNo ratings yet
- Evaluation of Infertile CoupleDocument70 pagesEvaluation of Infertile CoupleNdenwaneku OkuwaNo ratings yet
- 24 InfertilityDocument17 pages24 InfertilityDawit g/kidanNo ratings yet
- Infertility Report...Document9 pagesInfertility Report...sufian JaganyNo ratings yet
- Azdihar Lec 9 InfertilityDocument37 pagesAzdihar Lec 9 Infertilityalmastar officeNo ratings yet
- Female Infertility: DR Jaqueline Sudiman, PHDDocument21 pagesFemale Infertility: DR Jaqueline Sudiman, PHDJuli FionaNo ratings yet
- Gine 2p - MergedDocument30 pagesGine 2p - MergedHeidy MagañaNo ratings yet
- Obg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementDocument81 pagesObg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementElakkiyaanu64 Elakkiyaanu64No ratings yet
- INFERTILITYDocument48 pagesINFERTILITYAyisha EdwinNo ratings yet
- InfertilityDocument41 pagesInfertilityKiran RoyNo ratings yet
- Care of Clients With Reproductive Issues: Analiza M Gonzales Man, Maed LecturerDocument67 pagesCare of Clients With Reproductive Issues: Analiza M Gonzales Man, Maed LecturerJazther CapiliNo ratings yet
- Care of Male and Female Clients With General and Specific Problem in Reproduction and SexualityDocument7 pagesCare of Male and Female Clients With General and Specific Problem in Reproduction and SexualityAllaine Royce LibrandoNo ratings yet
- Infertility: Chegolihina L.VDocument29 pagesInfertility: Chegolihina L.VAmrutesh KhodkeNo ratings yet
- InfertilityDocument23 pagesInfertilityanduamlakmolalgn332No ratings yet
- Reproductive Issues 1Document61 pagesReproductive Issues 1Marl Dindreb JaoNo ratings yet
- Basic Infertility EvaluationDocument13 pagesBasic Infertility EvaluationRosu GeorgeNo ratings yet
- методы обследованияDocument49 pagesметоды обследованияNaincy SharmaNo ratings yet
- Early Bleeding in PregnancyDocument64 pagesEarly Bleeding in Pregnancymoreen kipkemoiNo ratings yet
- Lecture 19infertilityDocument34 pagesLecture 19infertilitySulaiman SanusiNo ratings yet
- 13 InfertilityDocument34 pages13 InfertilityWaad AlNo ratings yet
- Recent Advancement in Infertility ManagementDocument18 pagesRecent Advancement in Infertility ManagementFarheen khan100% (3)
- Week 1 - Women Health DisordersDocument41 pagesWeek 1 - Women Health Disordersmemoona kaleemNo ratings yet
- Infertility - Practice Essentials, Overview, Etiology of InfertilityDocument84 pagesInfertility - Practice Essentials, Overview, Etiology of Infertilityfeby megaNo ratings yet
- AmenorrheaDocument40 pagesAmenorrheaMeraol HusseinNo ratings yet
- Chapter 51: Nursing Assessment: Reproductive System: Structures and FunctionsDocument6 pagesChapter 51: Nursing Assessment: Reproductive System: Structures and FunctionsjefrocNo ratings yet
- Infertility: by Kenbon SDocument58 pagesInfertility: by Kenbon SgimNo ratings yet
- 1 Infertility EvaluationDocument9 pages1 Infertility Evaluationeldarhobe91No ratings yet
- InfertilityDocument23 pagesInfertilityoforiamponsahdaniel970No ratings yet
- Infertility: DR Madhusudhan C Associate Professor Department of Gen - MedicineDocument20 pagesInfertility: DR Madhusudhan C Associate Professor Department of Gen - MedicineTeena ChandranNo ratings yet
- Faq 147Document3 pagesFaq 147Gaylene Munsayac AldaveNo ratings yet
- Infertility, Investigation and Management: Dr. Raedah Al-FadhliDocument64 pagesInfertility, Investigation and Management: Dr. Raedah Al-Fadhliapi-3703352No ratings yet
- Bio IP Cla12 SsDocument8 pagesBio IP Cla12 SsTamilselvy AnsariNo ratings yet
- Session 8 Delayed Puberty&DevelopmentDocument20 pagesSession 8 Delayed Puberty&DevelopmentTimothy JaestylishNo ratings yet
- INFERTILITYDocument18 pagesINFERTILITYAmirNo ratings yet
- Reproduction, Technology, and The SocietyDocument38 pagesReproduction, Technology, and The SocietyJep LorenzoNo ratings yet
- Endometritis: R.N. Zainab Neamat JumaahDocument19 pagesEndometritis: R.N. Zainab Neamat JumaahKevin Adrian WijayaNo ratings yet
- 12 Female InfertilityDocument31 pages12 Female InfertilityawalsherNo ratings yet
- Infertility SlidesDocument49 pagesInfertility SlidesRwapembe StephenNo ratings yet
- Male Infertility, Diagnosis and Recent ManagementDocument77 pagesMale Infertility, Diagnosis and Recent ManagementDR SHASHWAT JANINo ratings yet
- Female InfertilityDocument4 pagesFemale InfertilitySonalika PatelNo ratings yet
- A Clinical Guide To Delayed PubertyDocument4 pagesA Clinical Guide To Delayed PubertyOleinic VeraNo ratings yet
- Gynecology Case Discussion History & Clinical Examination: DR - Ketaki Junnare DR - Shweta DR - Priyadarshini Dr. NamrataDocument36 pagesGynecology Case Discussion History & Clinical Examination: DR - Ketaki Junnare DR - Shweta DR - Priyadarshini Dr. Namratapriyadarshini adsulNo ratings yet
- Menstrual DisordersDocument77 pagesMenstrual Disorders2012100% (3)
- What Is InfertilityDocument10 pagesWhat Is InfertilityTemitopeNo ratings yet
- Introduction to Infertility (1)Document10 pagesIntroduction to Infertility (1)simrankumaria0No ratings yet
- Infertility: They Can't Have Bab IesDocument10 pagesInfertility: They Can't Have Bab Iesnyzgirl17No ratings yet
- Bio IpDocument10 pagesBio IpNamrata SaxenaNo ratings yet
- EndometriosisDocument9 pagesEndometriosiskotamalathi63No ratings yet
- Female InfertilityDocument33 pagesFemale InfertilityKiprotich Titus NgetichNo ratings yet
- InfertilityDocument8 pagesInfertilityrivannyNo ratings yet
- Bio IP Cla12 SsDocument8 pagesBio IP Cla12 SsTamilselvy AnsariNo ratings yet
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDocument36 pagesMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosoreNo ratings yet
- History Taking and Physical Examination in GynaecologyDocument41 pagesHistory Taking and Physical Examination in GynaecologygimNo ratings yet
- Ectopic Pregancy: Chena B. CurigDocument35 pagesEctopic Pregancy: Chena B. CurigJaicca Faith Tandih AllasNo ratings yet
- Reproductive Disorders in Females St.Document55 pagesReproductive Disorders in Females St.EstherThompsonNo ratings yet
- Infertility: SymptomsDocument9 pagesInfertility: SymptomsVyshak KrishnanNo ratings yet
- Alumna: Código:: - Guivin Pereyra SharonDocument42 pagesAlumna: Código:: - Guivin Pereyra SharonSharon Guivin PereyraNo ratings yet
- Mariott I 2012Document20 pagesMariott I 2012PrasadNo ratings yet
- 2021口试真题汇总 071104Document11 pages2021口试真题汇总 071104PrasadNo ratings yet
- ManupatiGangadhar NotesDocument10 pagesManupatiGangadhar NotesPrasadNo ratings yet
- W1717010003.internal MedicineDocument7 pagesW1717010003.internal MedicinePrasadNo ratings yet
- Ped NotesDocument59 pagesPed NotesPrasadNo ratings yet
- LUMBAR DISC NotesDocument7 pagesLUMBAR DISC NotesPrasadNo ratings yet
- Stomatology Class NotesDocument6 pagesStomatology Class NotesPrasadNo ratings yet
- Medicine Class NotesDocument15 pagesMedicine Class NotesPrasadNo ratings yet
- XX063Document3 pagesXX063BittuNo ratings yet
- UTS Physical Sexual Self ActivityDocument3 pagesUTS Physical Sexual Self ActivityHanna CasasNo ratings yet
- Biology ProjectDocument9 pagesBiology ProjectNitesh JaiswalNo ratings yet
- Form 4 Science Chapter 3 NotesDocument12 pagesForm 4 Science Chapter 3 NotesAnonymous klhru5ENo ratings yet
- Developmental Psychology Childhood Adolescence 9th Edition Shaffer Test BankDocument25 pagesDevelopmental Psychology Childhood Adolescence 9th Edition Shaffer Test BankPatriciaGrantetab100% (65)
- Biological ClassificationDocument30 pagesBiological ClassificationUttam SinghNo ratings yet
- Bio 9 EssayDocument2 pagesBio 9 EssayBryan LeNo ratings yet
- Best Dr. Chia Yin NinDocument8 pagesBest Dr. Chia Yin Ninhar shishNo ratings yet
- Biology Investigatory ProjectDocument26 pagesBiology Investigatory ProjectChinmay ChoudharyNo ratings yet
- Science 10Document51 pagesScience 10Michelle LapuzNo ratings yet
- Seed GerminationDocument12 pagesSeed Germinationhrishikesh08No ratings yet
- Emesculation & Pollinatin TechniquesDocument8 pagesEmesculation & Pollinatin TechniquesShivangi NegiNo ratings yet
- Science 5 Modes of Reproduction in Animals Quarter 2 Week 3: What Is ItDocument4 pagesScience 5 Modes of Reproduction in Animals Quarter 2 Week 3: What Is ItGOODWIN GALVANNo ratings yet
- LAB Mendelian TraitsDocument4 pagesLAB Mendelian TraitsJoshua RomeaNo ratings yet
- Podocarpus: Coniferopsida: Fouzia Youseph M.SC Botany (Sem2)Document9 pagesPodocarpus: Coniferopsida: Fouzia Youseph M.SC Botany (Sem2)Fouzia Youseph100% (1)
- AQA Entry Level Certificate Scheme of WorkDocument3 pagesAQA Entry Level Certificate Scheme of WorkChris HarrisNo ratings yet
- "Mediscan: Ob - First Trimester Scan ReportDocument3 pages"Mediscan: Ob - First Trimester Scan Reportshanmugasundaram32No ratings yet
- Perpetuation of Life Animal ReproductionDocument23 pagesPerpetuation of Life Animal ReproductionKyla Heart ZaragozaNo ratings yet
- PSN Endometriosis Nov 15 SD Feb 19Document56 pagesPSN Endometriosis Nov 15 SD Feb 19lili mursidaNo ratings yet
- (Updated) SECOND QUARTER EXAM in Earth and Life ScienceDocument8 pages(Updated) SECOND QUARTER EXAM in Earth and Life ScienceMELECIA, Dhenielle Mae T.100% (1)
- Family PlanningDocument34 pagesFamily PlanningArenz Rubi Tolentino IglesiasNo ratings yet
- Female Reproductive Physiology and Endocrinology of CattleDocument25 pagesFemale Reproductive Physiology and Endocrinology of CattleMarco MPNo ratings yet
- Grade 10 Biology Pollination ClassworkDocument2 pagesGrade 10 Biology Pollination Classworkbts trashNo ratings yet
- EnterMedSchool Biology Book-30Document628 pagesEnterMedSchool Biology Book-30SleoNo ratings yet
- Embryology ObgDocument36 pagesEmbryology ObgsamrusangaliNo ratings yet
- Fetal Membranes and PlacentaDocument48 pagesFetal Membranes and Placentaveegeer100% (4)