Download as pdf or txt
You might also like
- Secrets or Not Secrets - Confidentiality in Couple Therapy - 2009Document5 pagesSecrets or Not Secrets - Confidentiality in Couple Therapy - 2009NIYIDED DANIELA MARTÍNEZ MUÑOZNo ratings yet
- Harris - Harris - The Radiology of Emergency Medicine, 5th EditionDocument1,050 pagesHarris - Harris - The Radiology of Emergency Medicine, 5th EditionMadalina Talpau100% (1)
- Biostatistics Step 3 NotesDocument17 pagesBiostatistics Step 3 Notesrsimranjit100% (1)
- Guias 2012Document20 pagesGuias 2012Curro MirallesNo ratings yet
- Guidelines DVT PrimaryDocument2 pagesGuidelines DVT PrimaryRAMARNo ratings yet
- ADR Form AkhDocument2 pagesADR Form Akhsofiasofi191980No ratings yet
- UH Treatment Protocol Edit 6 March 24 2020Document9 pagesUH Treatment Protocol Edit 6 March 24 2020zeeNo ratings yet
- HeparinDocument4 pagesHeparinTri Purma SariNo ratings yet
- Anticoagulation EndosDocument16 pagesAnticoagulation EndosDr AhmedNo ratings yet
- L3 - Reducing Adverse Drug Reactions - 2022Document15 pagesL3 - Reducing Adverse Drug Reactions - 2022Kayleigh NorrisNo ratings yet
- Clinical Pathway Peds Appendicitis 2012Document3 pagesClinical Pathway Peds Appendicitis 2012DivaraNo ratings yet
- Thrombosis Risk Factor Assessment FormDocument3 pagesThrombosis Risk Factor Assessment Formpanel.anuphospitalNo ratings yet
- New May2020 PDFDocument7 pagesNew May2020 PDFDoctorMoodyNo ratings yet
- Covid Outpatient Management 2021 12 30Document2 pagesCovid Outpatient Management 2021 12 30Kj_bdNo ratings yet
- Primary Survey: Emergency/Disaster By: MR:GEBRIELLE HIPOLITO RN, USRN, MAN Emergency Nursing ProtocolsDocument7 pagesPrimary Survey: Emergency/Disaster By: MR:GEBRIELLE HIPOLITO RN, USRN, MAN Emergency Nursing ProtocolsJasmine JarapNo ratings yet
- How To Use The FYI FlagsDocument5 pagesHow To Use The FYI FlagsFuji guruNo ratings yet
- Kastay Insect BaitDocument6 pagesKastay Insect BaitCalvin PrasetioNo ratings yet
- PharmacovigilanceDocument33 pagesPharmacovigilanceAna Sarah KurniaNo ratings yet
- ADR ScalesDocument4 pagesADR ScalesAnonymous l39lxfzJNo ratings yet
- COVID-19 InterimGuidelines Treatment ENGDocument25 pagesCOVID-19 InterimGuidelines Treatment ENGMartin PaturlanneNo ratings yet
- ADR Form-MCp-PharmD VI Year InternshipDocument1 pageADR Form-MCp-PharmD VI Year InternshipMarifuddin HussainiNo ratings yet
- Covid Basics Poster v2 20211230Document2 pagesCovid Basics Poster v2 20211230Swagat MohantyNo ratings yet
- Update On Clinical Management - PrivateDocument57 pagesUpdate On Clinical Management - PrivateJashveerBediNo ratings yet
- Sarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalDocument2 pagesSarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalTan Chin AunNo ratings yet
- SanfordDocument8 pagesSanfordAndreea StancuNo ratings yet
- DaunorubicininjDocument16 pagesDaunorubicininjNaldo NathanNo ratings yet
- Acep Evidencecare Covid19severitytoolDocument3 pagesAcep Evidencecare Covid19severitytoolShariq IqbalNo ratings yet
- Suspected COVID-19 Cases Management in Triage HospitalsDocument6 pagesSuspected COVID-19 Cases Management in Triage HospitalsMuhamed RamadanNo ratings yet
- Sample Case Studies of COVID-19 in PregnancyDocument29 pagesSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNo ratings yet
- Low Molecular Weight Heparins Summary Prescribing Guide Version 1.3Document14 pagesLow Molecular Weight Heparins Summary Prescribing Guide Version 1.3sharief145No ratings yet
- Materi EPODocument24 pagesMateri EPONova M S PutriNo ratings yet
- Early Treatment Information For Doctors Updated 11042022Document4 pagesEarly Treatment Information For Doctors Updated 11042022han tianNo ratings yet
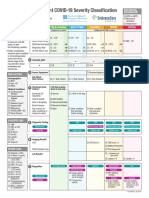
- Emergency Department COVID-19 Severity ClassificationDocument3 pagesEmergency Department COVID-19 Severity ClassificationAsti YumnaNo ratings yet
- Low Molecular Weigh Heparins Summary Prescribing Guide Version 14Document15 pagesLow Molecular Weigh Heparins Summary Prescribing Guide Version 14alexandr zinchenkoNo ratings yet
- Join Our High-Yield Medical Learning Community At: GNU 1.2: James Heilman, MD. ModifiedDocument18 pagesJoin Our High-Yield Medical Learning Community At: GNU 1.2: James Heilman, MD. ModifiedJoshua-Majid ShahbaziNo ratings yet
- Cossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberDocument2 pagesCossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberRocky BisNo ratings yet
- 21 Acute Liver Failure Guidelines 2017Document57 pages21 Acute Liver Failure Guidelines 2017Yoyo RashadNo ratings yet
- COVID-19 InterimGuidelines Treatment ENGDocument24 pagesCOVID-19 InterimGuidelines Treatment ENGHouda LaatabiNo ratings yet
- Fall_Risk_Assessment_FormDocument2 pagesFall_Risk_Assessment_FormQuality AssuranceNo ratings yet
- COVID-19 Antiviral TX Guidance 4-22-2020Document23 pagesCOVID-19 Antiviral TX Guidance 4-22-2020Lydia IsaacNo ratings yet
- 3A CTC 16 HypertensionDocument72 pages3A CTC 16 HypertensionHarissa Katrina De LaraNo ratings yet
- Screenshot 2020-03-20 at 08.25.44 PDFDocument10 pagesScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresNo ratings yet
- MGH mass-general-COVID-19-treatment-guidanceDocument21 pagesMGH mass-general-COVID-19-treatment-guidanceAli KhanzadaNo ratings yet
- Junio Covid-19 - Sanford GuideDocument8 pagesJunio Covid-19 - Sanford GuideEfraín Castilla MinayaNo ratings yet
- Barnet Primary Care Pathway During Covid19 v1 PDFDocument1 pageBarnet Primary Care Pathway During Covid19 v1 PDFAndrew WilkinsonNo ratings yet
- PSMID Guidelines COVID 19 - EditedDocument8 pagesPSMID Guidelines COVID 19 - EditedIsrael H. ZantuaNo ratings yet
- COVID19 Anticoagulation GuidelinesDocument2 pagesCOVID19 Anticoagulation GuidelinesVladut BibanNo ratings yet
- Acute Liver Failure EASL CPGDocument57 pagesAcute Liver Failure EASL CPGFatima Medriza DuranNo ratings yet
- RINVOQ Extended Prescription InformationDocument39 pagesRINVOQ Extended Prescription InformationLalo AbdoNo ratings yet
- Acute Liver Failure EASL CPGDocument57 pagesAcute Liver Failure EASL CPGRicky Cornelius Tarigan0% (1)
- Covid Coagulopathy Pit Papdi 2020Document46 pagesCovid Coagulopathy Pit Papdi 2020alvarocfad140699No ratings yet
- Dr. Widyati ADR ANALYSIS-PERSIDocument39 pagesDr. Widyati ADR ANALYSIS-PERSIHanaNo ratings yet
- Cossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberDocument2 pagesCossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberRocky BisNo ratings yet
- Sjs Fatal KRN AlopurinolDocument6 pagesSjs Fatal KRN AlopurinolMerliana DebyantiNo ratings yet
- Cossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberDocument2 pagesCossh Risk Assessment: Carried Out By: Department: Date: Substance Name: CRA NumberRocky BisNo ratings yet
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- AmlodipinaDocument2 pagesAmlodipinaCorina-Felicia BabosNo ratings yet
- 3 Pharmacovigilance IntroductionDocument68 pages3 Pharmacovigilance IntroductionPriya VarshneyNo ratings yet
- Guidance For Treatment of Covid-19 in Adults and Children: Patient PopulationDocument7 pagesGuidance For Treatment of Covid-19 in Adults and Children: Patient PopulationonkarratheeNo ratings yet
- Kent and Medway Inflammatory Bowel Disease Ibd Adults High Cost Drug HCD PathwayDocument8 pagesKent and Medway Inflammatory Bowel Disease Ibd Adults High Cost Drug HCD PathwaySavan QilahsNo ratings yet
- The Essential Guide to Prescription Drugs, Update on RemdesivirFrom EverandThe Essential Guide to Prescription Drugs, Update on RemdesivirNo ratings yet
- Patient Blood Management Guidelines Module 6 - Neonatal and Paediatrics.Document27 pagesPatient Blood Management Guidelines Module 6 - Neonatal and Paediatrics.Madalina TalpauNo ratings yet
- Prophylaxis Against Venous Thromboembolism in Pediatric Trauma A Practice Management Guideline From The Eastern Association For The Surgery ofDocument11 pagesProphylaxis Against Venous Thromboembolism in Pediatric Trauma A Practice Management Guideline From The Eastern Association For The Surgery ofMadalina TalpauNo ratings yet
- Treatment of Pressure Ulcers. in Prevention and Treatment of Pressure Ulcers Clinical Practice Guideline.Document33 pagesTreatment of Pressure Ulcers. in Prevention and Treatment of Pressure Ulcers Clinical Practice Guideline.Madalina TalpauNo ratings yet
- Management of Adult Pancreatic Injuries A Practice Management Guideline From The Eastern Association For The Surgery of Trauma.Document11 pagesManagement of Adult Pancreatic Injuries A Practice Management Guideline From The Eastern Association For The Surgery of Trauma.Madalina TalpauNo ratings yet
- Perioperative Management of Antithrombotic Therapy Antithrombotic Therapy and Prevention of ThrombosisDocument20 pagesPerioperative Management of Antithrombotic Therapy Antithrombotic Therapy and Prevention of ThrombosisMadalina TalpauNo ratings yet
- Operative Fixation of Rib Fractures After Blunt Trauma A Practice Management Guideline From The Eastern Association For The Surgery of Trauma.Document10 pagesOperative Fixation of Rib Fractures After Blunt Trauma A Practice Management Guideline From The Eastern Association For The Surgery of Trauma.Madalina TalpauNo ratings yet
- Guideline For Reversal of Antithrombotics in Intracranial Hemorrhage A Statement For Healthcare Professionals From The Neurocritical Care SocietyDocument13 pagesGuideline For Reversal of Antithrombotics in Intracranial Hemorrhage A Statement For Healthcare Professionals From The Neurocritical Care SocietyMadalina TalpauNo ratings yet
- Prevention of VTE in Nonsurgical Patients Antithrombotic Therapy and Prevention of ThrombosisDocument19 pagesPrevention of VTE in Nonsurgical Patients Antithrombotic Therapy and Prevention of ThrombosisMadalina TalpauNo ratings yet
- Pressure Ulcers Prevention and Management of Pressure Ulcers.Document27 pagesPressure Ulcers Prevention and Management of Pressure Ulcers.Madalina TalpauNo ratings yet
- KDIGO Clinical Practice Guideline For Lipid Management in Chronic Kidney Disease.Document13 pagesKDIGO Clinical Practice Guideline For Lipid Management in Chronic Kidney Disease.Madalina TalpauNo ratings yet
- Esophageal Varices.Document15 pagesEsophageal Varices.Madalina TalpauNo ratings yet
- Myocardial Infarction With ST-segment Elevation. The Acute Management of Myocardial Infarction With ST-segment Elevation.Document19 pagesMyocardial Infarction With ST-segment Elevation. The Acute Management of Myocardial Infarction With ST-segment Elevation.Madalina TalpauNo ratings yet
- Guidelines For The Management of Severe Traumatic Brain Injury, 4th Edition.Document17 pagesGuidelines For The Management of Severe Traumatic Brain Injury, 4th Edition.Madalina TalpauNo ratings yet
- A.S.P.E.N. Clinical Guidelines Nutrition Support of Hospitalized Adult Patients With Obesity.Document9 pagesA.S.P.E.N. Clinical Guidelines Nutrition Support of Hospitalized Adult Patients With Obesity.Madalina TalpauNo ratings yet
- Guidelines For The Provision and Assessment of Nutrition Support Therapy in The Adult Critically Ill Patient Society of Critical Care Medicine (SCCM)Document21 pagesGuidelines For The Provision and Assessment of Nutrition Support Therapy in The Adult Critically Ill Patient Society of Critical Care Medicine (SCCM)Madalina TalpauNo ratings yet
- AARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry 2013.Document14 pagesAARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry 2013.Madalina TalpauNo ratings yet
- Guideline On The Management of Bleeding in Patients On Antithrombotic Agents.Document10 pagesGuideline On The Management of Bleeding in Patients On Antithrombotic Agents.Madalina TalpauNo ratings yet
- Evidence-Based Guidelines For The Management of Large Hemispheric Infarction A Statement For Health Care Professionals From The NeurocriticalDocument15 pagesEvidence-Based Guidelines For The Management of Large Hemispheric Infarction A Statement For Health Care Professionals From The NeurocriticalMadalina TalpauNo ratings yet
- Antithrombotic Therapy For VTE Disease CHEST Guideline and Expert Panel Report.Document16 pagesAntithrombotic Therapy For VTE Disease CHEST Guideline and Expert Panel Report.Madalina TalpauNo ratings yet
- Pain Management For Blunt Thoracic Trauma A Joint Practice Management Guideline From The Eastern Association For The Surgery of Trauma andDocument12 pagesPain Management For Blunt Thoracic Trauma A Joint Practice Management Guideline From The Eastern Association For The Surgery of Trauma andMadalina TalpauNo ratings yet
- ACR Appropriateness Criteria® Acute Chest Pain - Suspected Pulmonary Embolism.Document16 pagesACR Appropriateness Criteria® Acute Chest Pain - Suspected Pulmonary Embolism.Madalina TalpauNo ratings yet
- An Official American Thoracic Society Clinical Practice Guideline The Diagnosis of Intensive Care Unit-Acquired Weakness in Adults.Document9 pagesAn Official American Thoracic Society Clinical Practice Guideline The Diagnosis of Intensive Care Unit-Acquired Weakness in Adults.Madalina TalpauNo ratings yet
- Blood Transfusion.Document23 pagesBlood Transfusion.Madalina TalpauNo ratings yet
- BTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Document21 pagesBTSICS Guideline For The Ventilatory Management of Acute Hypercapnic Respiratory Failure in Adults.Madalina TalpauNo ratings yet
- Acute Upper Gastrointestinal Bleeding Management.Document18 pagesAcute Upper Gastrointestinal Bleeding Management.Madalina TalpauNo ratings yet
- Lupu Torace PDFDocument74 pagesLupu Torace PDFMadalina TalpauNo ratings yet
- Saskatoon Ostomy Association Bulletin For April 2016Document12 pagesSaskatoon Ostomy Association Bulletin For April 2016Peter FolkNo ratings yet
- Tugas 1 Menjaga Kesehatan TubuhhDocument9 pagesTugas 1 Menjaga Kesehatan TubuhhDiah Dwi NursyaidahNo ratings yet
- 13 Patient Saefty and Quality ImprovementDocument36 pages13 Patient Saefty and Quality ImprovementShafiq Ur RahmanNo ratings yet
- NEJM ResponseDocument2 pagesNEJM Responseamit545No ratings yet
- Rainwater and Stormwater Harvesting Systems: Continuing Education From The American Society of Plumbing EngineersDocument8 pagesRainwater and Stormwater Harvesting Systems: Continuing Education From The American Society of Plumbing Engineers185412No ratings yet
- Int Endodontic J - January 1995 - RAY - Periapical Status of Endodontically Treated Teeth in Relation To The TechnicalDocument8 pagesInt Endodontic J - January 1995 - RAY - Periapical Status of Endodontically Treated Teeth in Relation To The Technicalj sNo ratings yet
- 1 Identification of The Substance/mixture and of The Company/undertakingDocument5 pages1 Identification of The Substance/mixture and of The Company/undertakingPaul SmithNo ratings yet
- Eye Infection and Blepharitis by MHSNDocument18 pagesEye Infection and Blepharitis by MHSNMhsn0% (1)
- Topnotch Pharma Supertable JAN 2016Document166 pagesTopnotch Pharma Supertable JAN 2016Dar AD50% (2)
- Assignment No.1Document5 pagesAssignment No.1PatrickGonzalesNo ratings yet
- Sample Size CalculationDocument27 pagesSample Size Calculationkai dollNo ratings yet
- Applying Hot and Cold WaterDocument9 pagesApplying Hot and Cold WaterdamarNo ratings yet
- Left Sided & Right Sided Heart FailureDocument29 pagesLeft Sided & Right Sided Heart FailureRachelle Ayn100% (3)
- Management of Chronic Gingivitis PDFDocument5 pagesManagement of Chronic Gingivitis PDFliaamNo ratings yet
- Ecg NoobsDocument103 pagesEcg NoobsGhaidaa Sadeq100% (1)
- Systemic Couple Therapy and DepressionDocument3 pagesSystemic Couple Therapy and DepressionAna MoraisNo ratings yet
- PTJ 99 12 1587Document15 pagesPTJ 99 12 1587ganesh goreNo ratings yet
- Be Your Own Doctor With Acupressure - Dr. Dhiren GalaDocument69 pagesBe Your Own Doctor With Acupressure - Dr. Dhiren GalaParag Chhaper100% (2)
- Healthcare Deposit AccountDocument12 pagesHealthcare Deposit AccountdeonptNo ratings yet
- Telomere AssignmentDocument13 pagesTelomere AssignmentMay OmarNo ratings yet
- Trauma From Occlusion - An Orthodontists PerspectDocument2 pagesTrauma From Occlusion - An Orthodontists PerspectGoutam NookalaNo ratings yet
- A Short Account of Obsessional Neurosis - Hara PepeliDocument9 pagesA Short Account of Obsessional Neurosis - Hara PepelibarisNo ratings yet
- Pip Venix LRDocument2 pagesPip Venix LRThanh VoNo ratings yet
- Clase II Division 1 Terapia MiofuncionalDocument10 pagesClase II Division 1 Terapia MiofuncionalAngely LaraNo ratings yet
- Invitation & Confirmation Respiratory Meet The Expert Meeting 2019Document2 pagesInvitation & Confirmation Respiratory Meet The Expert Meeting 2019WicakNo ratings yet
- American Heart Association: Advanced Cardiovascular Life Support Written ExamsDocument36 pagesAmerican Heart Association: Advanced Cardiovascular Life Support Written ExamsAndrew Sefain56% (9)
- Adjuncts To The Secondary SurveyDocument10 pagesAdjuncts To The Secondary SurveyLaraib KanwalNo ratings yet
- AlcoholDocument12 pagesAlcoholLauraLoaizaNo ratings yet
- Medical Devices in DermatologyDocument7 pagesMedical Devices in DermatologyAKANo ratings yet