Download as pdf or txt
You might also like
- Work Method Statement For Directional DrillingDocument3 pagesWork Method Statement For Directional Drillingnice hossainNo ratings yet
- 02 D017 9074Document10 pages02 D017 9074Rahma Aulia LestariNo ratings yet
- Piis0889540607003277 PDFDocument7 pagesPiis0889540607003277 PDFAly OsmanNo ratings yet
- ADJALEXU - Volume 46 - Issue Issue 2 - Pages 113-120Document8 pagesADJALEXU - Volume 46 - Issue Issue 2 - Pages 113-120imamagarlzNo ratings yet
- INSISIVDocument7 pagesINSISIVLansky TrimeilanaNo ratings yet
- Dimensi Vertikal FotoDocument10 pagesDimensi Vertikal FotoPrevita NindaNo ratings yet
- Three-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFDocument10 pagesThree-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFSoe San KyawNo ratings yet
- Yang. AJODO 2015. Effect of Mesiodistal Angulation of The Maxillary Central Incisors On Esthetic Perceptions of The Smile Frontal ViewDocument9 pagesYang. AJODO 2015. Effect of Mesiodistal Angulation of The Maxillary Central Incisors On Esthetic Perceptions of The Smile Frontal Viewjustin4leNo ratings yet
- Craniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingDocument10 pagesCraniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingMonojit DuttaNo ratings yet
- Dental Anomalies in Different Growth and Skeletal Malocclusion PatternsDocument7 pagesDental Anomalies in Different Growth and Skeletal Malocclusion PatternsShruthi KamarajNo ratings yet
- Self-Perception of The Facial Profile An Aid in TRDocument7 pagesSelf-Perception of The Facial Profile An Aid in TRmehdi chahrourNo ratings yet
- Filip Boeru, Sînziana Constantinescu, Dan-Alexandru Mărîi, Roxana Zăpârţan, Magdalena Enache, UMF Carol Davila', BucureştiDocument1 pageFilip Boeru, Sînziana Constantinescu, Dan-Alexandru Mărîi, Roxana Zăpârţan, Magdalena Enache, UMF Carol Davila', BucureştiRoxana LuţicNo ratings yet
- Anterior Crossbite in The Primary Dentition: Proposal For A New Analytical Method in ChildrenDocument5 pagesAnterior Crossbite in The Primary Dentition: Proposal For A New Analytical Method in ChildrenAri SatriaNo ratings yet
- The Genetic Basis of Facial Skeletal Characteristics and Its Relation With OrthodonticsDocument6 pagesThe Genetic Basis of Facial Skeletal Characteristics and Its Relation With OrthodonticssmritiNo ratings yet
- Comparing The Perception of Dentists and Lay People To Altered Dental EstheticsDocument14 pagesComparing The Perception of Dentists and Lay People To Altered Dental EstheticsDaniel AtiehNo ratings yet
- Hartmann 2004Document7 pagesHartmann 2004ramiro alejandro torres velezNo ratings yet
- Shape Variation and Sex Differences of The Adult Human Mandible Evaluated by Geometric MorphometricsDocument13 pagesShape Variation and Sex Differences of The Adult Human Mandible Evaluated by Geometric MorphometricsMia MikaelaNo ratings yet
- The Effects of Buccal CorridorDocument9 pagesThe Effects of Buccal CorridorTrần Thị Như NgọcNo ratings yet
- Bergman Soft TissueDocument9 pagesBergman Soft TissueClaudia Gamboa FerrerNo ratings yet
- Correlation Between Maxillary Central Incisor Crown Morphology and Mandibular Dental Arch Form in Normal Occlusion SubjectsDocument5 pagesCorrelation Between Maxillary Central Incisor Crown Morphology and Mandibular Dental Arch Form in Normal Occlusion SubjectsJessi RecaldeNo ratings yet
- Annals of Anatomy: Reinhard E. Friedrich, Carsten Ulbricht, Ljuba A. Baronesse Von MaydellDocument12 pagesAnnals of Anatomy: Reinhard E. Friedrich, Carsten Ulbricht, Ljuba A. Baronesse Von MaydellVinay KumarNo ratings yet
- Malocclusion and Orthodontic Treatment Need Among 12-15-Year-Old Children in NairobiDocument6 pagesMalocclusion and Orthodontic Treatment Need Among 12-15-Year-Old Children in NairobiWainaianaNo ratings yet
- Quantitative Investigation of The Esthetic Impact of Lip Prominence in Relation To The Esthetic LineDocument8 pagesQuantitative Investigation of The Esthetic Impact of Lip Prominence in Relation To The Esthetic LineNadila RahmaNo ratings yet
- Diagnosis and Treatment Planning With 3-Dimensional Dentofacial RecordsDocument9 pagesDiagnosis and Treatment Planning With 3-Dimensional Dentofacial RecordsThibaut BossuytNo ratings yet
- Growth Patterns and Overbite Depth Indicators of Long and Short Faces in Korean Adolescents: Revisited Through Mixed Effects AnalysisDocument22 pagesGrowth Patterns and Overbite Depth Indicators of Long and Short Faces in Korean Adolescents: Revisited Through Mixed Effects AnalysisBs PhuocNo ratings yet
- Biometric Study of Human TeethDocument12 pagesBiometric Study of Human TeethKenigal14No ratings yet
- Malocclusion Prevalence in An Ethnic Chinese PopulationDocument8 pagesMalocclusion Prevalence in An Ethnic Chinese PopulationLuis SarmientoNo ratings yet
- Three-Dimensional Evaluation of Morphologic Tooth Symmetry in Various MalocclusionsDocument8 pagesThree-Dimensional Evaluation of Morphologic Tooth Symmetry in Various MalocclusionsSoe San KyawNo ratings yet
- Smile Esthetics From The Layperson 'S Perspective: Online OnlyDocument11 pagesSmile Esthetics From The Layperson 'S Perspective: Online OnlyPae Anusorn AmtanonNo ratings yet
- Role of Cephalometery in Evaluation of Vertical DimensionDocument4 pagesRole of Cephalometery in Evaluation of Vertical DimensionAhmad ShoeibNo ratings yet
- Art. Odontoped BDocument8 pagesArt. Odontoped BfarlyblancoNo ratings yet
- Mercado 2011Document6 pagesMercado 2011Husni mubarakNo ratings yet
- Annual Review JPD 2019 PDFDocument72 pagesAnnual Review JPD 2019 PDFNiaz AhammedNo ratings yet
- Multiple Simple Bone Cysts of The Jaws - Review of The Literature and Report of Three CasesDocument12 pagesMultiple Simple Bone Cysts of The Jaws - Review of The Literature and Report of Three CasesRodolpho VilelaNo ratings yet
- Asymmetry of The Face in Orthodontic PatientsDocument6 pagesAsymmetry of The Face in Orthodontic PatientsplsssssNo ratings yet
- Abstract 2004Document45 pagesAbstract 2004MOHD ISYRAFUDDIN ISMAILNo ratings yet
- Golden Proportion Analysis of Dental-Skeletal Patterns of Class II and III Patients Pre and Post Orthodontic-Orthognathic TreatmentDocument6 pagesGolden Proportion Analysis of Dental-Skeletal Patterns of Class II and III Patients Pre and Post Orthodontic-Orthognathic TreatmentTanya HernandezNo ratings yet
- Morphometric Analysis of Three Normal Facial Types in Mixed Dentition Using Posteroanterior Cephalometric Radiographs: Preliminary ResultsDocument6 pagesMorphometric Analysis of Three Normal Facial Types in Mixed Dentition Using Posteroanterior Cephalometric Radiographs: Preliminary ResultsSEBASTIAN ANDRES MIRANDA GONZALEZNo ratings yet
- Krishan KumarDocument7 pagesKrishan KumarVi LinhNo ratings yet
- Dental Development and Craniofacial Morphology in School-Age ChildrenDocument13 pagesDental Development and Craniofacial Morphology in School-Age ChildrenAyman RaoNo ratings yet
- Evaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyDocument10 pagesEvaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyPututu PatataNo ratings yet
- International Journal of Medical and Health ResearchDocument8 pagesInternational Journal of Medical and Health ResearchIonela MadalinaNo ratings yet
- 2012-X - Relationship Between Dental Arch Dimensions AndveDocument9 pages2012-X - Relationship Between Dental Arch Dimensions AndveAnaFlaviaMedinaNo ratings yet
- Eruption AnomalyDocument7 pagesEruption AnomalyJay BernalNo ratings yet
- Indice FacialDocument7 pagesIndice FacialAli ChaconNo ratings yet
- Developmental Dental Anomalies Assessed by Panoramic Radiographs in A Greek Orthodontic Population SampleDocument6 pagesDevelopmental Dental Anomalies Assessed by Panoramic Radiographs in A Greek Orthodontic Population SamplefghdhmdkhNo ratings yet
- Ferreira 2020Document10 pagesFerreira 2020Dela MedinaNo ratings yet
- Woodworth1985 PDFDocument14 pagesWoodworth1985 PDFacevariel5851No ratings yet
- 6dana373 46 Ijmd v4 I3 IJMD3-2014 PDFDocument7 pages6dana373 46 Ijmd v4 I3 IJMD3-2014 PDFNadia Syifa AmiraNo ratings yet
- Artigo Inglês 4Document4 pagesArtigo Inglês 4Ana LuizaNo ratings yet
- Effects of Extraction and Nonextraction Therapy With Air-Rotor Stripping On Facial Esthetics in Postadolescent Borderline PatientsDocument11 pagesEffects of Extraction and Nonextraction Therapy With Air-Rotor Stripping On Facial Esthetics in Postadolescent Borderline PatientsAly OsmanNo ratings yet
- Incisor Root Resorption Associated With Palatally Displaced Maxillary Canines: Analysis and Prediction Using Discriminant Function AnalysisDocument11 pagesIncisor Root Resorption Associated With Palatally Displaced Maxillary Canines: Analysis and Prediction Using Discriminant Function AnalysisnomanNo ratings yet
- Tracto GubernacularDocument7 pagesTracto GubernacularCarlos MerinoNo ratings yet
- Prevalence of Peg-Shaped Maxillary Permanent Lateral Incisors: A Meta-AnalysisDocument13 pagesPrevalence of Peg-Shaped Maxillary Permanent Lateral Incisors: A Meta-Analysisplayer osamaNo ratings yet
- Comparison of Perceptions On The DentalDocument5 pagesComparison of Perceptions On The DentalRaul GhiurcaNo ratings yet
- Nam SE, Kim YH, Park YS, Baek SH, Hayashi K, Kim KN, Lee SP. Three-Dimensional Dental Model Constructed From An Average Dental Form.Document6 pagesNam SE, Kim YH, Park YS, Baek SH, Hayashi K, Kim KN, Lee SP. Three-Dimensional Dental Model Constructed From An Average Dental Form.HweeHo KimNo ratings yet
- Clinical and CephalometricDocument7 pagesClinical and CephalometricIsmaelLouGomezNo ratings yet
- Lyu 2018Document7 pagesLyu 2018Andres CoboNo ratings yet
- Primary Jaw Tumors in ChildrenDocument6 pagesPrimary Jaw Tumors in ChildrenJeyachandran MariappanNo ratings yet
- Overbite Depth Indicator and Anteroposterior Dysplasia Indicator Cephalometric Norms For African AmericansDocument6 pagesOverbite Depth Indicator and Anteroposterior Dysplasia Indicator Cephalometric Norms For African AmericansLiliana AguilarNo ratings yet
- Ortodoncia Interdisciplinar Margarita VarelaDocument442 pagesOrtodoncia Interdisciplinar Margarita VarelaALEJANDRA INÉS NIETO ARIASNo ratings yet
- Stability and Relapse After Orthodontic Treatment of Deep Bite Cases-A Long-Term Follow-Up StudyDocument9 pagesStability and Relapse After Orthodontic Treatment of Deep Bite Cases-A Long-Term Follow-Up StudyALEJANDRA INÉS NIETO ARIASNo ratings yet
- Development of A Questionnaire For Assessment of The Psychosocial Impact of Dental Aesthetics in Young AdultsDocument9 pagesDevelopment of A Questionnaire For Assessment of The Psychosocial Impact of Dental Aesthetics in Young AdultsALEJANDRA INÉS NIETO ARIASNo ratings yet
- Boton de Nace 2Document11 pagesBoton de Nace 2ALEJANDRA INÉS NIETO ARIASNo ratings yet
- CJM 098Document6 pagesCJM 098ALEJANDRA INÉS NIETO ARIASNo ratings yet
- AJODO 2017aksuetalDocument8 pagesAJODO 2017aksuetalALEJANDRA INÉS NIETO ARIASNo ratings yet
- The Rebel: by D.J.EnrightDocument20 pagesThe Rebel: by D.J.EnrightNandini kNo ratings yet
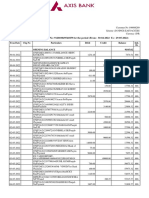
- Statement of Axis Account No:912010049541859 For The Period (From: 30-04-2022 To: 29-05-2022)Document5 pagesStatement of Axis Account No:912010049541859 For The Period (From: 30-04-2022 To: 29-05-2022)Rahul BansalNo ratings yet
- 102 - SCO8048A-Alert - Fixings-FinalDocument3 pages102 - SCO8048A-Alert - Fixings-FinalO SNo ratings yet
- VMX User ManualDocument94 pagesVMX User ManualRoger M OlsonNo ratings yet
- Maharashtra HSC Mathematics Paper 1Document18 pagesMaharashtra HSC Mathematics Paper 1YouTibeNo ratings yet
- Factors Contributing To Burberry'S Failure 1Document16 pagesFactors Contributing To Burberry'S Failure 1benjaminNo ratings yet
- Case Shaping Future Business Leaders 9 June 2016Document7 pagesCase Shaping Future Business Leaders 9 June 2016Alka AggarwalNo ratings yet
- PracticalDocument5 pagesPracticalMarjorrie C. BritalNo ratings yet
- Certified Sirim MIKROTIK PDFDocument3 pagesCertified Sirim MIKROTIK PDFArul Auni AqilNo ratings yet
- Sds Limestone-F-PulverizedDocument6 pagesSds Limestone-F-PulverizedAzuan MABKNo ratings yet
- MonitersDocument25 pagesMonitersJaveed AhamedNo ratings yet
- Altizer - Godhead and The NothingDocument180 pagesAltizer - Godhead and The NothingRocabatus100% (1)
- Part 1 固定常考: Work/StudyDocument31 pagesPart 1 固定常考: Work/Study书签No ratings yet
- Zohdy, Eaton & Mabey - Application of Surface Geophysics To Ground-Water Investigations - USGSDocument63 pagesZohdy, Eaton & Mabey - Application of Surface Geophysics To Ground-Water Investigations - USGSSalman AkbarNo ratings yet
- Parasite - Global Issues - English LPDocument4 pagesParasite - Global Issues - English LPSiddhesh SoodNo ratings yet
- Newborn Studio Guide by Jessica G. PhotographyDocument13 pagesNewborn Studio Guide by Jessica G. PhotographyClau ppNo ratings yet
- Python StuffDocument4 pagesPython Stuffganimator DiscordNo ratings yet
- Avaya G250 Media Gateway With An Avaya S8300 ServerDocument22 pagesAvaya G250 Media Gateway With An Avaya S8300 ServerRoberto MontagnanaNo ratings yet
- Android Quiz App 22617 MADDocument19 pagesAndroid Quiz App 22617 MADSandip kotkarNo ratings yet
- Which Functor Is The Projective Line?Document16 pagesWhich Functor Is The Projective Line?flores3831_814460512No ratings yet
- Islam & Modern Science by Waleed1991Document118 pagesIslam & Modern Science by Waleed1991waleed1991No ratings yet
- Andrea Reaction Paper FinalDocument3 pagesAndrea Reaction Paper FinalIrene SabidNo ratings yet
- Steven Johnsons SyndromeDocument22 pagesSteven Johnsons SyndromeRoselene Mae MarasiganNo ratings yet
- 173x 174X Quadcable Safety Alert CUSTOMER LETTER Rev5 TRDocument3 pages173x 174X Quadcable Safety Alert CUSTOMER LETTER Rev5 TRonurNo ratings yet
- Cronica Report Malcolm McLeanDocument2 pagesCronica Report Malcolm McLeanomar andres rodriguez veraNo ratings yet
- CR Eniram-User-Manual QUEEN SmallDocument62 pagesCR Eniram-User-Manual QUEEN Small赵焕彪No ratings yet
- Godrej and Boyce Corporate ProfileDocument2 pagesGodrej and Boyce Corporate ProfileAyushi JainNo ratings yet
- Is.2042.2006 Insulating BricksDocument8 pagesIs.2042.2006 Insulating BricksGaneshNo ratings yet
- Tos - TrendsDocument2 pagesTos - TrendsBernadette Falceso100% (1)