Download as pdf or txt
You might also like
- Diabetic Ketoacidosis (DKA)Document33 pagesDiabetic Ketoacidosis (DKA)Eric Chye Teck100% (1)
- 100 NCLEX QuestionsDocument69 pages100 NCLEX QuestionsIke Agbor100% (12)
- Insulin Wall ChartDocument1 pageInsulin Wall Charturcrony10No ratings yet
- Hyperglycaemic Emergencies Inpatient Draft-1-3Document13 pagesHyperglycaemic Emergencies Inpatient Draft-1-3Cik JaaNo ratings yet
- DKA Management-2Document7 pagesDKA Management-2NisaNo ratings yet
- DKA Guidelines Version 4.0 28 Dec 2016FINALDocument4 pagesDKA Guidelines Version 4.0 28 Dec 2016FINALbenNo ratings yet
- Dka ProtocolDocument3 pagesDka ProtocolRed DevilNo ratings yet
- Fluid and Electrolytes ManagementDocument21 pagesFluid and Electrolytes ManagementRasYa DINo ratings yet
- Guidelines in The Treatment of Hyper Osmolar Non Ketotic Coma (Honk)Document4 pagesGuidelines in The Treatment of Hyper Osmolar Non Ketotic Coma (Honk)picassowaffleNo ratings yet
- Item 6f - Acute Management of Hyperosmolar Hyperglycaemic StateDocument1 pageItem 6f - Acute Management of Hyperosmolar Hyperglycaemic StateStef AnNo ratings yet
- High CBS in Medical EmergencyDocument37 pagesHigh CBS in Medical EmergencyHansika GunasekaraNo ratings yet
- DKA PosterDocument2 pagesDKA PosterainizatiNo ratings yet
- Commonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Document23 pagesCommonly Prescribed Medications in Surgical Ed Sivakami Ver 5.0Suiweng WongNo ratings yet
- Diabetic Ketoacidosis Mangment GuidlinesDocument23 pagesDiabetic Ketoacidosis Mangment Guidlines21910589No ratings yet
- NFCC. Chapter 8. ElectrolytesDocument13 pagesNFCC. Chapter 8. ElectrolytesOsman fadilNo ratings yet
- IVFluids Guideline Poster July 2017Document1 pageIVFluids Guideline Poster July 2017rana muzamilNo ratings yet
- Guideline Title: Management of Diabetic KetoacidosisDocument9 pagesGuideline Title: Management of Diabetic KetoacidosisJorge Salazar GomezNo ratings yet
- Dka Guidelines - 2012Document4 pagesDka Guidelines - 2012djizhieeNo ratings yet
- Electrolyte Disturbance Quick GuideDocument11 pagesElectrolyte Disturbance Quick GuideTianaNo ratings yet
- MGT of D KetoacidosisDocument5 pagesMGT of D Ketoacidosisshabatat2002No ratings yet
- Guideline For The Management of Children and Young People Under The Age of 18 Years With Diabetic Ketoacidosis (DKA)Document26 pagesGuideline For The Management of Children and Young People Under The Age of 18 Years With Diabetic Ketoacidosis (DKA)Arslan SiddiquiNo ratings yet
- Paed Parenteral Fluid ThyDocument1 pagePaed Parenteral Fluid ThyZulia Ahmad BurhaniNo ratings yet
- Hyperglycaemic Hyperosmolar State - HHS Nov15Document12 pagesHyperglycaemic Hyperosmolar State - HHS Nov15Nader NURESNo ratings yet
- HyperkalaemiaDocument1 pageHyperkalaemiaRekaBNo ratings yet
- LTHT Paediatric Administration Guide Intravenous Sodium BicarbonateDocument2 pagesLTHT Paediatric Administration Guide Intravenous Sodium BicarbonateAjay KumarNo ratings yet
- Management of Hyperosmolar Hyperglycaemic StateDocument11 pagesManagement of Hyperosmolar Hyperglycaemic StateTowhidulIslamNo ratings yet
- Diabetic Emergencies: 1. Diabetic Ketoacidosis 2. Hyperglycemic Hyperosmolar State 3. HypoglycemiaDocument24 pagesDiabetic Emergencies: 1. Diabetic Ketoacidosis 2. Hyperglycemic Hyperosmolar State 3. HypoglycemiachooNo ratings yet
- Hypokalaemia Guidelines v1 - May 2018Document9 pagesHypokalaemia Guidelines v1 - May 2018EmaNo ratings yet
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisDocument1 pageDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- Fluid Therapy: Presenter: Chew Zi Qi Supervisor: Dr. Tan KWDocument43 pagesFluid Therapy: Presenter: Chew Zi Qi Supervisor: Dr. Tan KWaslanNo ratings yet
- Diabetes MellitusDocument20 pagesDiabetes MellitusNICHOLAS KAUMBANo ratings yet
- Early Symptoms: Insidious Increase in Polydipsia and PolyuriaDocument3 pagesEarly Symptoms: Insidious Increase in Polydipsia and Polyuriabes3rkerNo ratings yet
- Potassium-Chloride-Intravenous ANMF1.0 20201208Document5 pagesPotassium-Chloride-Intravenous ANMF1.0 20201208aldyNo ratings yet
- 12 - Diabetic Emergencies-DKADocument13 pages12 - Diabetic Emergencies-DKABalqis AqisNo ratings yet
- Diabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyDocument24 pagesDiabetic Ketoacidosis Acute Management: A State of Absolute Insulin BankruptcyGwEn LimNo ratings yet
- Compressed Emilyokelly PetchkutchaDocument20 pagesCompressed Emilyokelly Petchkutchaapi-269001337No ratings yet
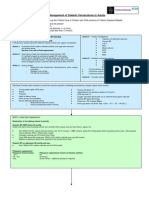
- Management of Hyperglycemic Crises in Adult Patients With DiabetesDocument5 pagesManagement of Hyperglycemic Crises in Adult Patients With DiabetesJisaNo ratings yet
- Clinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Document13 pagesClinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Azim Abd Razak100% (1)
- Management of Anesthesia: Diabetes MellitusDocument29 pagesManagement of Anesthesia: Diabetes MellitusHari PrasadNo ratings yet
- Cisplatin-and-Etoposide (Ovarian Cancer)Document4 pagesCisplatin-and-Etoposide (Ovarian Cancer)Sindu SankarNo ratings yet
- IRIS 2009 Treatment Recommendations SummaryDocument5 pagesIRIS 2009 Treatment Recommendations SummaryJessicaHernandezNo ratings yet
- By Melese A (Mi) Kalkidan A (Mi)Document38 pagesBy Melese A (Mi) Kalkidan A (Mi)Tegegn LegesseNo ratings yet
- Intravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)Document4 pagesIntravenous Insulin Prescription and Fluid Protocol: For Diabetic Keto-Acidosis (Dka)sunrise755No ratings yet
- Too Much of A Good Thing: Danielle BlouinDocument5 pagesToo Much of A Good Thing: Danielle BlouinAndry GoniusNo ratings yet
- Labetalolivhyper 18Document2 pagesLabetalolivhyper 18TOJO JOSEPH TOMNo ratings yet
- Dka-Hhs Topic DiscussionDocument2 pagesDka-Hhs Topic Discussionapi-648401824No ratings yet
- Acute Hyperkalaemia in AdultsDocument12 pagesAcute Hyperkalaemia in AdultsMeilina FitrianiNo ratings yet
- Metabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSDocument5 pagesMetabolic Disorders LONG CHAIN FAT OXIDATION DISORDERSMahmoud khedrNo ratings yet
- Calcitriol - Drug InformationDocument13 pagesCalcitriol - Drug InformationNikesh DoshiNo ratings yet
- Management of Diabetic Ketoacidosis: MW SavageDocument3 pagesManagement of Diabetic Ketoacidosis: MW Savagedramaysingh100% (1)
- 3-Management of DF-DHF2018Document36 pages3-Management of DF-DHF2018koengphearom9No ratings yet
- Idiot NotesDocument53 pagesIdiot NotesRay PerezNo ratings yet
- Contact Details Name: Hospital Telephone:: This Protocol Has 4 PagesDocument4 pagesContact Details Name: Hospital Telephone:: This Protocol Has 4 PagesCaterina PrepelitaNo ratings yet
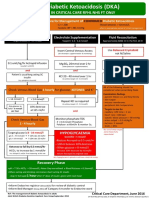
- Adult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyDocument1 pageAdult Diabetic Ketoacidosis (DKA) : For Use in Critical Care RFHL Nhs FT OnlyJung Bahadur SinghNo ratings yet
- 2017 Refeeding Syndrome A Case Report PDFDocument6 pages2017 Refeeding Syndrome A Case Report PDFManual de VacunaciónNo ratings yet
- HyperkalaemiaDocument2 pagesHyperkalaemiapaleviNo ratings yet
- New Format MasterDocument34 pagesNew Format MasterMuhammad FurqanNo ratings yet
- Diabetic Ketoacidosis Dka Hyperglycemic Hyperosmolar State Hhs Adult PDFDocument4 pagesDiabetic Ketoacidosis Dka Hyperglycemic Hyperosmolar State Hhs Adult PDFyayaNo ratings yet
- HyperkalaemiaDocument6 pagesHyperkalaemiathinzarNo ratings yet
- Kuwait PICU Taskforce DKA V1 5 June 2022Document2 pagesKuwait PICU Taskforce DKA V1 5 June 2022Emad MashaalNo ratings yet
- Diabetic Ketoacidosis Treatment Protocol PDFDocument3 pagesDiabetic Ketoacidosis Treatment Protocol PDFMoses MalungaNo ratings yet
- Should Ultra-Rapid Acting Analogs Be The New Standard of Mealtime Insulins Care?Document51 pagesShould Ultra-Rapid Acting Analogs Be The New Standard of Mealtime Insulins Care?Oscar CastañonNo ratings yet
- Insulin and The Oral HypoglycemicsDocument9 pagesInsulin and The Oral HypoglycemicsHasibNo ratings yet
- Heparin and Insulin DripsDocument11 pagesHeparin and Insulin DripsCeleste Chapman100% (2)
- Analgesics: AnticonvulsantsDocument8 pagesAnalgesics: AnticonvulsantsGina Giammalvo100% (1)
- Diabetes TreatmentDocument14 pagesDiabetes TreatmentmusimsemiNo ratings yet
- Carbohydrate CountingDocument32 pagesCarbohydrate CountingMatthew NathanielNo ratings yet
- Insulin TherapyDocument55 pagesInsulin TherapyShriyank BhargavaNo ratings yet
- Pre Op GuidelinesDocument11 pagesPre Op GuidelinesHanif FebrianNo ratings yet
- Case Study Diabetes MellitusDocument4 pagesCase Study Diabetes MellitusGabbii CincoNo ratings yet
- Pink Panther - Diabetes Management - Chapter 4Document8 pagesPink Panther - Diabetes Management - Chapter 4jennmoyerNo ratings yet
- Generički Naziv Lijeka (Zabranjena Supstanca) Registrovani Preparati (Komercijalni Naziv) Zaštićeno Ime Lijeka Oznaka U LZS 2015 Oznaka U ATCDocument7 pagesGenerički Naziv Lijeka (Zabranjena Supstanca) Registrovani Preparati (Komercijalni Naziv) Zaštićeno Ime Lijeka Oznaka U LZS 2015 Oznaka U ATCДраган ЧолићNo ratings yet
- Diabetes in The Elderly: Sanjay Kalra Suresh K. SharmaDocument8 pagesDiabetes in The Elderly: Sanjay Kalra Suresh K. SharmaNicthe Ruiz RodríguezNo ratings yet
- Dosage CalculationsDocument56 pagesDosage Calculationsrustiejade100% (6)
- Antidiabetic Agents-WPS OfficeDocument4 pagesAntidiabetic Agents-WPS OfficeSourajyoti GoswamiNo ratings yet
- Role of The Diabetes Educator in Inpatient Diabetes ManagementDocument8 pagesRole of The Diabetes Educator in Inpatient Diabetes ManagementVinay KushawahaNo ratings yet
- Accu Chek Aviva Expert Quick Start GuideDocument2 pagesAccu Chek Aviva Expert Quick Start Guideasyraf khairyNo ratings yet
- Diabetes Drug Notes (2022)Document393 pagesDiabetes Drug Notes (2022)evansNo ratings yet
- DM AAFP ManagementDocument8 pagesDM AAFP ManagementphilsguNo ratings yet
- Farmakologi DMDocument41 pagesFarmakologi DMZainul MuttaqinNo ratings yet
- BIOD - Biodel: Catalyst Date: 10/30/10 Drug: Linjeta Run-Up Potential: StrongDocument8 pagesBIOD - Biodel: Catalyst Date: 10/30/10 Drug: Linjeta Run-Up Potential: StrongemagooNo ratings yet
- Remar Nurse Pharmacology Review: Brought To You by Regina M. Callion MSN, RN Creator of The NCLEX Virtual TrainerDocument50 pagesRemar Nurse Pharmacology Review: Brought To You by Regina M. Callion MSN, RN Creator of The NCLEX Virtual TrainerMonalizaSantos100% (2)
- Chapter 60 - Insulin, Oral Hypoglycaemic Agents, and The Pharmacology of The Endocrine PancreasDocument17 pagesChapter 60 - Insulin, Oral Hypoglycaemic Agents, and The Pharmacology of The Endocrine PancreasGiliana P. García AcevedoNo ratings yet
- 60-2005 - Pregestational Diabetes MellitusDocument11 pages60-2005 - Pregestational Diabetes MellitusGrupo Atlas100% (1)
- DM Type IIDocument48 pagesDM Type IILila HeridyatnoNo ratings yet
- Rapid-Acting Insulin (Onset: 15-30 MinsDocument5 pagesRapid-Acting Insulin (Onset: 15-30 MinsBea TanNo ratings yet
- The Basics of Diabetes: Phar 811 Peyton Teets Pharmd Candidate School of Pharmacy - West Virginia UniversityDocument39 pagesThe Basics of Diabetes: Phar 811 Peyton Teets Pharmd Candidate School of Pharmacy - West Virginia UniversityMa'rifatulAuliaNo ratings yet
- Antidiabetic Drugs: DR Naser Ashraf Tadvi Associate Professor, Pharmacology Ayaan Institute of Medical SciencesDocument63 pagesAntidiabetic Drugs: DR Naser Ashraf Tadvi Associate Professor, Pharmacology Ayaan Institute of Medical SciencesMelati SatriasNo ratings yet
- Protocolo Da BombaDocument52 pagesProtocolo Da BombaEmerson SaNo ratings yet