
Stress and Social Support Among Registered Nurses in A Level II NICU
Stress and Social Support Among Registered Nurses in A Level II NICU
You might also like
- Recalling Stress and Trauma in The Workplace - A Qualitative Study of Pediatric NursesDocument7 pagesRecalling Stress and Trauma in The Workplace - A Qualitative Study of Pediatric NursesnanaNo ratings yet
- Gagne's Conditions of LearningDocument3 pagesGagne's Conditions of LearningCza Mae ArsenalNo ratings yet
- Reducing Nurses' Stress - A Randomized Controlled Trial of A Web-BasedDocument8 pagesReducing Nurses' Stress - A Randomized Controlled Trial of A Web-BasedHilal Mohamed Nor0% (1)
- Applied Linear Regression Models by John Neter, William Wasserman, Michael H. KutnerDocument561 pagesApplied Linear Regression Models by John Neter, William Wasserman, Michael H. KutnerGina McCaffrey91% (11)
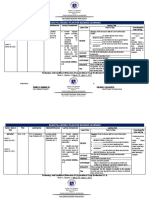
- RAISE Plus WEEKLY PLAN FOR BLENDED LEARNING TleDocument3 pagesRAISE Plus WEEKLY PLAN FOR BLENDED LEARNING TleRomeo jr RamirezNo ratings yet
- 10 1016@j Pedn 2020 05 006Document7 pages10 1016@j Pedn 2020 05 006Mohammad Al-arrabi AldhidiNo ratings yet
- Foro Critico NarDocument23 pagesForo Critico NarrelaxenfermeriaumbNo ratings yet
- Family Center Care VisitingDocument2 pagesFamily Center Care VisitinginaNo ratings yet
- 1 s2.0 S1471595322002207 MainDocument6 pages1 s2.0 S1471595322002207 MainYudi Tubagja SiregarNo ratings yet
- An Effective Communication Initiative UsDocument8 pagesAn Effective Communication Initiative UsIsabel Cuéllar FloresNo ratings yet
- Van Patten 2019Document6 pagesVan Patten 2019Amrinder RandhawaNo ratings yet
- E N ' P: F A C: Mergency Urses Erspectives Actors Ffecting AringDocument7 pagesE N ' P: F A C: Mergency Urses Erspectives Actors Ffecting AringAngelina PondeteNo ratings yet
- 06 IngDocument14 pages06 IngTerapia Ocupacional Apae BrotasNo ratings yet
- Transition Shock, Preceptor Support and Nursing Competency Among NewlyDocument7 pagesTransition Shock, Preceptor Support and Nursing Competency Among NewlyNurfadhila IlhamNo ratings yet
- Emergency Nurses' PerspectivesDocument7 pagesEmergency Nurses' PerspectivesRima Isnaimun SitompulNo ratings yet
- Nurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesDocument5 pagesNurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesShiee Nevhie ParaDinata WapersNo ratings yet
- Children: Nursing Perspective of The Humanized Care of The Neonate and Family: A Systematic ReviewDocument19 pagesChildren: Nursing Perspective of The Humanized Care of The Neonate and Family: A Systematic ReviewMacarena Cortes CarvalloNo ratings yet
- 1 s2.0 S0260691723000199 MainDocument8 pages1 s2.0 S0260691723000199 MainJonathan LollarNo ratings yet
- 2013NCCWeisEnhancingperson CentredcommunicationDocument13 pages2013NCCWeisEnhancingperson CentredcommunicationDiulia SantanaNo ratings yet
- Nurse Education Today: Angel C.K. Lee, Sharron S.K. Leung, Y.W. MakDocument7 pagesNurse Education Today: Angel C.K. Lee, Sharron S.K. Leung, Y.W. MakSri YantiNo ratings yet
- SJMPS 34282 290Document10 pagesSJMPS 34282 290Ronel ResurricionNo ratings yet
- Developing Interprofessional Communication SkillsDocument5 pagesDeveloping Interprofessional Communication SkillsWai AbrahamNo ratings yet
- Novice Nurse Support Group: A Pilot StudyDocument21 pagesNovice Nurse Support Group: A Pilot Studyastor toNo ratings yet
- Assessment of Stress and Coping Strategies For Mothers of Hospitalized ChildrenDocument16 pagesAssessment of Stress and Coping Strategies For Mothers of Hospitalized ChildrenNovelty JournalsNo ratings yet
- Nurse Education Today: Snjezana Cukljek, Vesna Juresa, Janko BabicDocument5 pagesNurse Education Today: Snjezana Cukljek, Vesna Juresa, Janko BabicYunita AmiliaNo ratings yet
- Anato y Fisio Percepcion Del LaboratorioDocument4 pagesAnato y Fisio Percepcion Del LaboratorioOscarito ArriagadaNo ratings yet
- District Nursing and FamilywhDocument11 pagesDistrict Nursing and Familywhnoventina7marbunNo ratings yet
- Gholami 2021Document5 pagesGholami 2021C109 Muhammad Fahmi amrullohNo ratings yet
- Causas de Satisfacción e Insatisfaccion en Enfermeras - OhioDocument7 pagesCausas de Satisfacción e Insatisfaccion en Enfermeras - OhioMelissa Tello EspinozaNo ratings yet
- The Collaboration of General Practitioners and SpainDocument15 pagesThe Collaboration of General Practitioners and SpainVindy LesnussaNo ratings yet
- Praktek Komunikasi Di Ruangan ANak Petecost Hospital MadinaDocument9 pagesPraktek Komunikasi Di Ruangan ANak Petecost Hospital Madinaatika indriyadiNo ratings yet
- Finding Your PlaceDocument11 pagesFinding Your PlacetiniliciousNo ratings yet
- Rae 2021Document11 pagesRae 2021Salome MwangiNo ratings yet
- 2014JCNWeisImprovednurse ParentcommunicationDocument13 pages2014JCNWeisImprovednurse ParentcommunicationIsabel Cuéllar FloresNo ratings yet
- 1 s2.0 S0260691722000132 MainDocument9 pages1 s2.0 S0260691722000132 MainUmiNo ratings yet
- Nurse Education in Practice: Xiaoyi Cao, Lei Wang, Shenyi Wei, Jin Li, Shu GongDocument7 pagesNurse Education in Practice: Xiaoyi Cao, Lei Wang, Shenyi Wei, Jin Li, Shu GongR kshaafNo ratings yet
- Andre, 2016. Embedding Evidence-Based Practice Among Nursing UndergraduatesDocument6 pagesAndre, 2016. Embedding Evidence-Based Practice Among Nursing UndergraduatesLina MarcelaNo ratings yet
- Cilar 2020Document7 pagesCilar 2020Laiza May LampadNo ratings yet
- Journal SynthesisDocument4 pagesJournal SynthesisJharel Verbo EspirituNo ratings yet
- Scholarly Article PaperDocument7 pagesScholarly Article Paperapi-545697687No ratings yet
- The Relationship of Nursing TeamworkDocument12 pagesThe Relationship of Nursing TeamworkJovanna YatacoNo ratings yet
- 10 1016@j Ijnurstu 2017 02 009 PDFDocument18 pages10 1016@j Ijnurstu 2017 02 009 PDFDesiNo ratings yet
- Scholarly Paper CapstoneDocument6 pagesScholarly Paper Capstoneapi-662404021No ratings yet
- Tugas Bahasa Inggris - Temu 1 - KLP 8 - A12 BDocument8 pagesTugas Bahasa Inggris - Temu 1 - KLP 8 - A12 BErina NiluhNo ratings yet
- Effect of Nursing Care Delivery Models On Registered Nurse OutcomesDocument10 pagesEffect of Nursing Care Delivery Models On Registered Nurse OutcomesEva SahabNo ratings yet
- Expert Intrapartum Maternity Care: A Meta-Synthesis: ReviewpaperDocument14 pagesExpert Intrapartum Maternity Care: A Meta-Synthesis: ReviewpaperNines RíosNo ratings yet
- Therapeutic Communication Through Simulation PDFDocument5 pagesTherapeutic Communication Through Simulation PDFNicole GadrinabNo ratings yet
- Stress Among Mothers Whose Neonate Admitted in NICUDocument4 pagesStress Among Mothers Whose Neonate Admitted in NICUInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Doede 2020Document10 pagesDoede 2020cindymaulidahsalsabilahNo ratings yet
- Nursing Care in The Neonatal Intensive Care Unit ForDocument5 pagesNursing Care in The Neonatal Intensive Care Unit Forroldao.carlosNo ratings yet
- J Nepr 2020 102963Document9 pagesJ Nepr 2020 102963cruzchristophertangaNo ratings yet
- Improving The Quality of Nursing Students Clinical Plac 2014 Nurse EducatioDocument7 pagesImproving The Quality of Nursing Students Clinical Plac 2014 Nurse EducatioNurhidayah NoordinNo ratings yet
- Decision Making During Obstetric Emergencies A Narrative ApproachDocument21 pagesDecision Making During Obstetric Emergencies A Narrative Approachrafenia nayaniNo ratings yet
- 10 5923 J Nursing PhilipensDocument7 pages10 5923 J Nursing PhilipensnasimhsNo ratings yet
- Article in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudyDocument7 pagesArticle in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudySimson TameonNo ratings yet
- Perceptions of Nursing: A Study Involving Nurses, Nursing Students, Patients and Non-Nursing StudentsDocument12 pagesPerceptions of Nursing: A Study Involving Nurses, Nursing Students, Patients and Non-Nursing StudentsErditha MirandaNo ratings yet
- Family Centere Care Di NICUDocument11 pagesFamily Centere Care Di NICUNeni SiraitNo ratings yet
- Thomas 2016Document6 pagesThomas 2016Septyana M ANo ratings yet
- G2 3rd Revision FIRST HALFDocument20 pagesG2 3rd Revision FIRST HALFSbs Nhanxzkie Jountey MushroomxzNo ratings yet
- Applying Legitimation Code Theory To Teach Breastfeedi - 2023 - Nurse EducationDocument8 pagesApplying Legitimation Code Theory To Teach Breastfeedi - 2023 - Nurse EducationRonald QuezadaNo ratings yet
- Nurse Education Today: Joelle Yan Xin Chua, Shefaly ShoreyDocument9 pagesNurse Education Today: Joelle Yan Xin Chua, Shefaly ShoreyflorenceNo ratings yet
- Caring For Sick Kids An Integrative Review of TheDocument11 pagesCaring For Sick Kids An Integrative Review of TheShermaigne Ananayo BuyaNo ratings yet
- Perinatal Palliative Care: A Clinical GuideFrom EverandPerinatal Palliative Care: A Clinical GuideErin M. Denney-KoelschNo ratings yet
- CHCCCS017 STDNT Assess BK V1 29.05.19 2Document71 pagesCHCCCS017 STDNT Assess BK V1 29.05.19 2Silvia BuiNo ratings yet
- ComparisonofAxialLoadonColumn FormattedPaperDocument7 pagesComparisonofAxialLoadonColumn FormattedPaperVictor Omotoriogun100% (1)
- 1 - PilotSPM206 Branch Circuit Power Meter Catalog (KVA) (230523 - CUN - B)Document4 pages1 - PilotSPM206 Branch Circuit Power Meter Catalog (KVA) (230523 - CUN - B)KhairilMunawarNo ratings yet
- EC 02 - Species - GM BinderDocument114 pagesEC 02 - Species - GM BinderAlbyNo ratings yet
- Terhadap Pola Hidup Sehat Masyarakat Kecamatan PrambananDocument10 pagesTerhadap Pola Hidup Sehat Masyarakat Kecamatan PrambananNurul HidayatNo ratings yet
- KH53 US EnglishDocument12 pagesKH53 US EnglishmohamedsamimorsiNo ratings yet
- Public Administration (OB)Document4 pagesPublic Administration (OB)kiran100% (1)
- 1 - 1 Elements of ClimateDocument8 pages1 - 1 Elements of Climatekhalfani jumaNo ratings yet
- MSC Thesis Defense Presentation - TufailDocument38 pagesMSC Thesis Defense Presentation - TufailNeerajNo ratings yet
- Programme - DIES Alumni Forum - Preliminary 2022 - 10.10Document6 pagesProgramme - DIES Alumni Forum - Preliminary 2022 - 10.10D SusiloNo ratings yet
- 1.2 Bus Admittance Matrix: FormulationDocument11 pages1.2 Bus Admittance Matrix: FormulationMohamed Elsir100% (1)
- Chapter1 Microchip FabricationDocument39 pagesChapter1 Microchip Fabrication吳文嘉100% (1)
- Presentation, Analysis, and Interpretation of Data: Tongco ST., Maysan, Valenzuela CityDocument10 pagesPresentation, Analysis, and Interpretation of Data: Tongco ST., Maysan, Valenzuela CityAnne BustilloNo ratings yet
- Physiological FeelingsDocument202 pagesPhysiological Feelingsoscarin123456789No ratings yet
- Lorenz 1986Document10 pagesLorenz 1986Jessica Lienlaf RojasNo ratings yet
- Ground Water EngineeringDocument3 pagesGround Water EngineeringAnil MarsaniNo ratings yet
- Dwnload Full Fundamentals of Cost Accounting 3rd Edition Lanen Solutions Manual PDFDocument35 pagesDwnload Full Fundamentals of Cost Accounting 3rd Edition Lanen Solutions Manual PDFmatte.caudalebvf100% (13)
- Anthropology NOTESDocument4 pagesAnthropology NOTESPraful N K100% (2)
- Assignment # 2 MethodDocument4 pagesAssignment # 2 MethodEmy heartNo ratings yet
- 2000 Words EssayDocument6 pages2000 Words Essaylwfdwwwhd100% (2)
- What Is Research Collaboration?Document19 pagesWhat Is Research Collaboration?adni_wgNo ratings yet
- Checking of Forms Sample TemplateDocument3 pagesChecking of Forms Sample TemplateMilain NabiaNo ratings yet
- Unit 1 Lessons 1 and 2Document8 pagesUnit 1 Lessons 1 and 2ivanNo ratings yet
- SCZ Salongo Bio 1 2020Document11 pagesSCZ Salongo Bio 1 2020JoanNo ratings yet
- Literature Review Harvard Style SampleDocument5 pagesLiterature Review Harvard Style Sampleiigheacnd100% (1)
- SimbuDocument3 pagesSimbu84- R. SilamabarasanNo ratings yet
- Lec 3 (Linked List)Document12 pagesLec 3 (Linked List)Dr LolaNo ratings yet
























































































Download as pdf or txt
You might also like
- Recalling Stress and Trauma in The Workplace - A Qualitative Study of Pediatric NursesDocument7 pagesRecalling Stress and Trauma in The Workplace - A Qualitative Study of Pediatric NursesnanaNo ratings yet
- Gagne's Conditions of LearningDocument3 pagesGagne's Conditions of LearningCza Mae ArsenalNo ratings yet
- Reducing Nurses' Stress - A Randomized Controlled Trial of A Web-BasedDocument8 pagesReducing Nurses' Stress - A Randomized Controlled Trial of A Web-BasedHilal Mohamed Nor0% (1)
- Applied Linear Regression Models by John Neter, William Wasserman, Michael H. KutnerDocument561 pagesApplied Linear Regression Models by John Neter, William Wasserman, Michael H. KutnerGina McCaffrey91% (11)
- RAISE Plus WEEKLY PLAN FOR BLENDED LEARNING TleDocument3 pagesRAISE Plus WEEKLY PLAN FOR BLENDED LEARNING TleRomeo jr RamirezNo ratings yet
- 10 1016@j Pedn 2020 05 006Document7 pages10 1016@j Pedn 2020 05 006Mohammad Al-arrabi AldhidiNo ratings yet
- Foro Critico NarDocument23 pagesForo Critico NarrelaxenfermeriaumbNo ratings yet
- Family Center Care VisitingDocument2 pagesFamily Center Care VisitinginaNo ratings yet
- 1 s2.0 S1471595322002207 MainDocument6 pages1 s2.0 S1471595322002207 MainYudi Tubagja SiregarNo ratings yet
- An Effective Communication Initiative UsDocument8 pagesAn Effective Communication Initiative UsIsabel Cuéllar FloresNo ratings yet
- Van Patten 2019Document6 pagesVan Patten 2019Amrinder RandhawaNo ratings yet
- E N ' P: F A C: Mergency Urses Erspectives Actors Ffecting AringDocument7 pagesE N ' P: F A C: Mergency Urses Erspectives Actors Ffecting AringAngelina PondeteNo ratings yet
- 06 IngDocument14 pages06 IngTerapia Ocupacional Apae BrotasNo ratings yet
- Transition Shock, Preceptor Support and Nursing Competency Among NewlyDocument7 pagesTransition Shock, Preceptor Support and Nursing Competency Among NewlyNurfadhila IlhamNo ratings yet
- Emergency Nurses' PerspectivesDocument7 pagesEmergency Nurses' PerspectivesRima Isnaimun SitompulNo ratings yet
- Nurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesDocument5 pagesNurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesShiee Nevhie ParaDinata WapersNo ratings yet
- Children: Nursing Perspective of The Humanized Care of The Neonate and Family: A Systematic ReviewDocument19 pagesChildren: Nursing Perspective of The Humanized Care of The Neonate and Family: A Systematic ReviewMacarena Cortes CarvalloNo ratings yet
- 1 s2.0 S0260691723000199 MainDocument8 pages1 s2.0 S0260691723000199 MainJonathan LollarNo ratings yet
- 2013NCCWeisEnhancingperson CentredcommunicationDocument13 pages2013NCCWeisEnhancingperson CentredcommunicationDiulia SantanaNo ratings yet
- Nurse Education Today: Angel C.K. Lee, Sharron S.K. Leung, Y.W. MakDocument7 pagesNurse Education Today: Angel C.K. Lee, Sharron S.K. Leung, Y.W. MakSri YantiNo ratings yet
- SJMPS 34282 290Document10 pagesSJMPS 34282 290Ronel ResurricionNo ratings yet
- Developing Interprofessional Communication SkillsDocument5 pagesDeveloping Interprofessional Communication SkillsWai AbrahamNo ratings yet
- Novice Nurse Support Group: A Pilot StudyDocument21 pagesNovice Nurse Support Group: A Pilot Studyastor toNo ratings yet
- Assessment of Stress and Coping Strategies For Mothers of Hospitalized ChildrenDocument16 pagesAssessment of Stress and Coping Strategies For Mothers of Hospitalized ChildrenNovelty JournalsNo ratings yet
- Nurse Education Today: Snjezana Cukljek, Vesna Juresa, Janko BabicDocument5 pagesNurse Education Today: Snjezana Cukljek, Vesna Juresa, Janko BabicYunita AmiliaNo ratings yet
- Anato y Fisio Percepcion Del LaboratorioDocument4 pagesAnato y Fisio Percepcion Del LaboratorioOscarito ArriagadaNo ratings yet
- District Nursing and FamilywhDocument11 pagesDistrict Nursing and Familywhnoventina7marbunNo ratings yet
- Gholami 2021Document5 pagesGholami 2021C109 Muhammad Fahmi amrullohNo ratings yet
- Causas de Satisfacción e Insatisfaccion en Enfermeras - OhioDocument7 pagesCausas de Satisfacción e Insatisfaccion en Enfermeras - OhioMelissa Tello EspinozaNo ratings yet
- The Collaboration of General Practitioners and SpainDocument15 pagesThe Collaboration of General Practitioners and SpainVindy LesnussaNo ratings yet
- Praktek Komunikasi Di Ruangan ANak Petecost Hospital MadinaDocument9 pagesPraktek Komunikasi Di Ruangan ANak Petecost Hospital Madinaatika indriyadiNo ratings yet
- Finding Your PlaceDocument11 pagesFinding Your PlacetiniliciousNo ratings yet
- Rae 2021Document11 pagesRae 2021Salome MwangiNo ratings yet
- 2014JCNWeisImprovednurse ParentcommunicationDocument13 pages2014JCNWeisImprovednurse ParentcommunicationIsabel Cuéllar FloresNo ratings yet
- 1 s2.0 S0260691722000132 MainDocument9 pages1 s2.0 S0260691722000132 MainUmiNo ratings yet
- Nurse Education in Practice: Xiaoyi Cao, Lei Wang, Shenyi Wei, Jin Li, Shu GongDocument7 pagesNurse Education in Practice: Xiaoyi Cao, Lei Wang, Shenyi Wei, Jin Li, Shu GongR kshaafNo ratings yet
- Andre, 2016. Embedding Evidence-Based Practice Among Nursing UndergraduatesDocument6 pagesAndre, 2016. Embedding Evidence-Based Practice Among Nursing UndergraduatesLina MarcelaNo ratings yet
- Cilar 2020Document7 pagesCilar 2020Laiza May LampadNo ratings yet
- Journal SynthesisDocument4 pagesJournal SynthesisJharel Verbo EspirituNo ratings yet
- Scholarly Article PaperDocument7 pagesScholarly Article Paperapi-545697687No ratings yet
- The Relationship of Nursing TeamworkDocument12 pagesThe Relationship of Nursing TeamworkJovanna YatacoNo ratings yet
- 10 1016@j Ijnurstu 2017 02 009 PDFDocument18 pages10 1016@j Ijnurstu 2017 02 009 PDFDesiNo ratings yet
- Scholarly Paper CapstoneDocument6 pagesScholarly Paper Capstoneapi-662404021No ratings yet
- Tugas Bahasa Inggris - Temu 1 - KLP 8 - A12 BDocument8 pagesTugas Bahasa Inggris - Temu 1 - KLP 8 - A12 BErina NiluhNo ratings yet
- Effect of Nursing Care Delivery Models On Registered Nurse OutcomesDocument10 pagesEffect of Nursing Care Delivery Models On Registered Nurse OutcomesEva SahabNo ratings yet
- Expert Intrapartum Maternity Care: A Meta-Synthesis: ReviewpaperDocument14 pagesExpert Intrapartum Maternity Care: A Meta-Synthesis: ReviewpaperNines RíosNo ratings yet
- Therapeutic Communication Through Simulation PDFDocument5 pagesTherapeutic Communication Through Simulation PDFNicole GadrinabNo ratings yet
- Stress Among Mothers Whose Neonate Admitted in NICUDocument4 pagesStress Among Mothers Whose Neonate Admitted in NICUInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Doede 2020Document10 pagesDoede 2020cindymaulidahsalsabilahNo ratings yet
- Nursing Care in The Neonatal Intensive Care Unit ForDocument5 pagesNursing Care in The Neonatal Intensive Care Unit Forroldao.carlosNo ratings yet
- J Nepr 2020 102963Document9 pagesJ Nepr 2020 102963cruzchristophertangaNo ratings yet
- Improving The Quality of Nursing Students Clinical Plac 2014 Nurse EducatioDocument7 pagesImproving The Quality of Nursing Students Clinical Plac 2014 Nurse EducatioNurhidayah NoordinNo ratings yet
- Decision Making During Obstetric Emergencies A Narrative ApproachDocument21 pagesDecision Making During Obstetric Emergencies A Narrative Approachrafenia nayaniNo ratings yet
- 10 5923 J Nursing PhilipensDocument7 pages10 5923 J Nursing PhilipensnasimhsNo ratings yet
- Article in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudyDocument7 pagesArticle in Press: The Experience of Intensive Care Nurses Caring For Patients With Delirium: A Phenomenological StudySimson TameonNo ratings yet
- Perceptions of Nursing: A Study Involving Nurses, Nursing Students, Patients and Non-Nursing StudentsDocument12 pagesPerceptions of Nursing: A Study Involving Nurses, Nursing Students, Patients and Non-Nursing StudentsErditha MirandaNo ratings yet
- Family Centere Care Di NICUDocument11 pagesFamily Centere Care Di NICUNeni SiraitNo ratings yet
- Thomas 2016Document6 pagesThomas 2016Septyana M ANo ratings yet
- G2 3rd Revision FIRST HALFDocument20 pagesG2 3rd Revision FIRST HALFSbs Nhanxzkie Jountey MushroomxzNo ratings yet
- Applying Legitimation Code Theory To Teach Breastfeedi - 2023 - Nurse EducationDocument8 pagesApplying Legitimation Code Theory To Teach Breastfeedi - 2023 - Nurse EducationRonald QuezadaNo ratings yet
- Nurse Education Today: Joelle Yan Xin Chua, Shefaly ShoreyDocument9 pagesNurse Education Today: Joelle Yan Xin Chua, Shefaly ShoreyflorenceNo ratings yet
- Caring For Sick Kids An Integrative Review of TheDocument11 pagesCaring For Sick Kids An Integrative Review of TheShermaigne Ananayo BuyaNo ratings yet
- Perinatal Palliative Care: A Clinical GuideFrom EverandPerinatal Palliative Care: A Clinical GuideErin M. Denney-KoelschNo ratings yet
- CHCCCS017 STDNT Assess BK V1 29.05.19 2Document71 pagesCHCCCS017 STDNT Assess BK V1 29.05.19 2Silvia BuiNo ratings yet
- ComparisonofAxialLoadonColumn FormattedPaperDocument7 pagesComparisonofAxialLoadonColumn FormattedPaperVictor Omotoriogun100% (1)
- 1 - PilotSPM206 Branch Circuit Power Meter Catalog (KVA) (230523 - CUN - B)Document4 pages1 - PilotSPM206 Branch Circuit Power Meter Catalog (KVA) (230523 - CUN - B)KhairilMunawarNo ratings yet
- EC 02 - Species - GM BinderDocument114 pagesEC 02 - Species - GM BinderAlbyNo ratings yet
- Terhadap Pola Hidup Sehat Masyarakat Kecamatan PrambananDocument10 pagesTerhadap Pola Hidup Sehat Masyarakat Kecamatan PrambananNurul HidayatNo ratings yet
- KH53 US EnglishDocument12 pagesKH53 US EnglishmohamedsamimorsiNo ratings yet
- Public Administration (OB)Document4 pagesPublic Administration (OB)kiran100% (1)
- 1 - 1 Elements of ClimateDocument8 pages1 - 1 Elements of Climatekhalfani jumaNo ratings yet
- MSC Thesis Defense Presentation - TufailDocument38 pagesMSC Thesis Defense Presentation - TufailNeerajNo ratings yet
- Programme - DIES Alumni Forum - Preliminary 2022 - 10.10Document6 pagesProgramme - DIES Alumni Forum - Preliminary 2022 - 10.10D SusiloNo ratings yet
- 1.2 Bus Admittance Matrix: FormulationDocument11 pages1.2 Bus Admittance Matrix: FormulationMohamed Elsir100% (1)
- Chapter1 Microchip FabricationDocument39 pagesChapter1 Microchip Fabrication吳文嘉100% (1)
- Presentation, Analysis, and Interpretation of Data: Tongco ST., Maysan, Valenzuela CityDocument10 pagesPresentation, Analysis, and Interpretation of Data: Tongco ST., Maysan, Valenzuela CityAnne BustilloNo ratings yet
- Physiological FeelingsDocument202 pagesPhysiological Feelingsoscarin123456789No ratings yet
- Lorenz 1986Document10 pagesLorenz 1986Jessica Lienlaf RojasNo ratings yet
- Ground Water EngineeringDocument3 pagesGround Water EngineeringAnil MarsaniNo ratings yet
- Dwnload Full Fundamentals of Cost Accounting 3rd Edition Lanen Solutions Manual PDFDocument35 pagesDwnload Full Fundamentals of Cost Accounting 3rd Edition Lanen Solutions Manual PDFmatte.caudalebvf100% (13)
- Anthropology NOTESDocument4 pagesAnthropology NOTESPraful N K100% (2)
- Assignment # 2 MethodDocument4 pagesAssignment # 2 MethodEmy heartNo ratings yet
- 2000 Words EssayDocument6 pages2000 Words Essaylwfdwwwhd100% (2)
- What Is Research Collaboration?Document19 pagesWhat Is Research Collaboration?adni_wgNo ratings yet
- Checking of Forms Sample TemplateDocument3 pagesChecking of Forms Sample TemplateMilain NabiaNo ratings yet
- Unit 1 Lessons 1 and 2Document8 pagesUnit 1 Lessons 1 and 2ivanNo ratings yet
- SCZ Salongo Bio 1 2020Document11 pagesSCZ Salongo Bio 1 2020JoanNo ratings yet
- Literature Review Harvard Style SampleDocument5 pagesLiterature Review Harvard Style Sampleiigheacnd100% (1)
- SimbuDocument3 pagesSimbu84- R. SilamabarasanNo ratings yet
- Lec 3 (Linked List)Document12 pagesLec 3 (Linked List)Dr LolaNo ratings yet