Download as pdf or txt
You might also like
- UWorld Notes NeurologyDocument6 pagesUWorld Notes NeurologysarahNo ratings yet
- Stages of Anaesthesia NotesDocument2 pagesStages of Anaesthesia NotesNomathamsanqa Khumalo100% (2)
- Diagnosing Arnie Grape From The MovieDocument4 pagesDiagnosing Arnie Grape From The MovieAlbert MinNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Autonomic Dysreflexia in Spinal Cord Injury Overview, Pathophysiology, Causes of Autonomic DysreflexiaDocument14 pagesAutonomic Dysreflexia in Spinal Cord Injury Overview, Pathophysiology, Causes of Autonomic Dysreflexiajacque zidaneNo ratings yet
- Reflective Essay-Rexson A. DalanginDocument3 pagesReflective Essay-Rexson A. DalanginRexson Alcantara DalanginNo ratings yet
- Psych of Learning Chapter 3, Psych of Learning Chapter 4, PSYCH of Learning Chapter 5Document14 pagesPsych of Learning Chapter 3, Psych of Learning Chapter 4, PSYCH of Learning Chapter 5CoolNo ratings yet
- The Buying BrainDocument2 pagesThe Buying BrainHussain Aftab Changi50% (2)
- Autonomic Dysreflexia in Spinal Cord InjuryDocument5 pagesAutonomic Dysreflexia in Spinal Cord Injuryjulesubayubay5428No ratings yet
- Differential Diagnosis and StrokeDocument38 pagesDifferential Diagnosis and StrokeAin AmanyNo ratings yet
- Spinal Cord InjuryDocument15 pagesSpinal Cord InjurythereseNo ratings yet
- 09 (Autonomic Dysreflexia)Document15 pages09 (Autonomic Dysreflexia)SardarChangezKhanNo ratings yet
- Disorders of Ns-Reeves and SwensonDocument112 pagesDisorders of Ns-Reeves and SwensonSuganya BalachandranNo ratings yet
- Disreflexia AtonomicaDocument5 pagesDisreflexia AtonomicaNicolás Andrés MontanerNo ratings yet
- Era University College of Nursing Lucknow: Submitted To-: Submitted byDocument7 pagesEra University College of Nursing Lucknow: Submitted To-: Submitted byAru Verma100% (1)
- Chapter 14. The Dizzy Patient The Dizzy Patient: IntroductionDocument9 pagesChapter 14. The Dizzy Patient The Dizzy Patient: IntroductionjumabarrientosNo ratings yet
- Maestroke BriefDocument5 pagesMaestroke BriefNurse NotesNo ratings yet
- Bone FractureDocument15 pagesBone FractureDANITA JEAN V. MATURANNo ratings yet
- Compilation Spinal SsmsDocument35 pagesCompilation Spinal SsmsPiaRomildaTagaoCayetano100% (1)
- Cranial Nerve DisordersDocument218 pagesCranial Nerve DisordersRem AlfelorNo ratings yet
- UnconsciousnessDocument80 pagesUnconsciousnessDivya SomanNo ratings yet
- Diffrent Types of ShockDocument6 pagesDiffrent Types of ShockBasit AliNo ratings yet
- Neuro-Dr AsmaaDocument35 pagesNeuro-Dr AsmaaSoad RedaNo ratings yet
- Report SciDocument25 pagesReport SciHershey Cordero BrionesNo ratings yet
- Class Presentation CVADocument23 pagesClass Presentation CVAAmbika Ghosh SenNo ratings yet
- EXPOSEEDocument9 pagesEXPOSEEMind BlowerNo ratings yet
- Dialnet AccidenteCerebrovascularIsquemico 5460545Document1 pageDialnet AccidenteCerebrovascularIsquemico 5460545Antonella IncaNo ratings yet
- Herniasi OtakDocument5 pagesHerniasi OtakrahmaNo ratings yet
- Stroke, Epilepsy and TB Practical CasesDocument12 pagesStroke, Epilepsy and TB Practical CasesMustahedinNo ratings yet
- 15 Complications of Regional AnaesthesiaDocument6 pages15 Complications of Regional AnaesthesiaParvathy R NairNo ratings yet
- Management of Patients With Neurologic DisordersDocument9 pagesManagement of Patients With Neurologic DisordersJames Felix Gallano GalesNo ratings yet
- Wallenberg Syndrome: Publication DetailsDocument9 pagesWallenberg Syndrome: Publication DetailsHuang Jen Liang100% (1)
- Concept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesDocument6 pagesConcept Map For Anterior Myocardial Infarction: I. Introduction and ObjectivesLouise GudmalinNo ratings yet
- 3 Inflammatory and Immunologic ResponseDocument15 pages3 Inflammatory and Immunologic ResponseJanely EstreraNo ratings yet
- Seizure Disorder, Spinal Injury Neural TumorDocument52 pagesSeizure Disorder, Spinal Injury Neural TumornipoNo ratings yet
- Aracnoditis PDFDocument18 pagesAracnoditis PDFArockia Albert JerosonNo ratings yet
- Focus On StrokeDocument92 pagesFocus On StrokeDIAH RETNO WULAN100% (2)
- Acute Complications of Spinal Cord Injuries: Kemal NAS, Professor, Series EditorDocument8 pagesAcute Complications of Spinal Cord Injuries: Kemal NAS, Professor, Series EditorSeno adipNo ratings yet
- Spinal Cord Injuries (SCI) : DR - Anas AlashramDocument80 pagesSpinal Cord Injuries (SCI) : DR - Anas AlashramMarah AbdulrahimNo ratings yet
- Final Stroke MBDocument79 pagesFinal Stroke MBVanessa Yvonne GurtizaNo ratings yet
- Intracranial HemorrhageDocument5 pagesIntracranial HemorrhageMa. Cathlea SarmientoNo ratings yet
- CVA NotesDocument21 pagesCVA NotesVaibhav BhatiaNo ratings yet
- The Current Role of Physiotherapy in Neurological Practice StrokeDocument6 pagesThe Current Role of Physiotherapy in Neurological Practice StrokeAnne LeeNo ratings yet
- Complications of FracturesDocument13 pagesComplications of FracturesmilananandNo ratings yet
- Ischemic Stroke - 3B5Document77 pagesIschemic Stroke - 3B5Aireen Grace GilosNo ratings yet
- Q1.Flaccid Paresis: Diagnostical VariantsDocument47 pagesQ1.Flaccid Paresis: Diagnostical VariantsNelson OduorNo ratings yet
- Subdural HematomaDocument7 pagesSubdural Hematomamiss RN50% (2)
- Case 2Document3 pagesCase 2AyidhNo ratings yet
- Spontaneous Intracranial Hypotension - Diagnosis and ManagementDocument3 pagesSpontaneous Intracranial Hypotension - Diagnosis and ManagementMazin Al-TahirNo ratings yet
- Lee 2015Document12 pagesLee 2015Bagus Pithu Ha SpingNo ratings yet
- Guillain - Barre SyndromeDocument63 pagesGuillain - Barre SyndrometheamaciasNo ratings yet
- Cerebral Vascular AccidentDocument70 pagesCerebral Vascular AccidentSheda BondNo ratings yet
- Litrev Trauma MuskuloskeletalDocument26 pagesLitrev Trauma Muskuloskeletaldedyalkarni08No ratings yet
- A06 NEJM Neurocardiogenic SyncopeDocument7 pagesA06 NEJM Neurocardiogenic SyncopeGabriel CampolinaNo ratings yet
- Med SurgDocument98 pagesMed SurgKimsha Concepcion88% (8)
- Birth InjuriesDocument103 pagesBirth InjuriesAruna ApNo ratings yet
- Iicp 1Document5 pagesIicp 1Melodia Turqueza GandezaNo ratings yet
- Neurologic Emergencies 2 MergedDocument71 pagesNeurologic Emergencies 2 MergedDanica FrancoNo ratings yet
- Ebp PresentationDocument17 pagesEbp Presentationapi-252593358No ratings yet
- Reports in SciDocument8 pagesReports in SciJarold PerezNo ratings yet
- Spinal Cord Injury: Neck ChestDocument4 pagesSpinal Cord Injury: Neck Chestavinash dhameriyaNo ratings yet
- Approach To Coma GroupDocument10 pagesApproach To Coma GroupFuad AwelNo ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Giant Cell Arteritis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandGiant Cell Arteritis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Acute Complications Following Gamma Knife Radiosurgery Are RareDocument5 pagesAcute Complications Following Gamma Knife Radiosurgery Are Rareadk eijfNo ratings yet
- Neurophysiology: The Central Nervous SystemDocument52 pagesNeurophysiology: The Central Nervous System143roshanNo ratings yet
- Aphasia Visuals:InfoDocument25 pagesAphasia Visuals:InfoLivia Payn100% (1)
- Glasgow Coma ScaleDocument3 pagesGlasgow Coma ScaleLanie Reyes de Guzman0% (1)
- Child SCAT5Document8 pagesChild SCAT5KinesiuzNo ratings yet
- Editable Task CardsDocument7 pagesEditable Task Cardshamza shahareNo ratings yet
- Christian Thibaudeau - High-Threshold Muscle BuildingDocument204 pagesChristian Thibaudeau - High-Threshold Muscle BuildingWojtek Adamczyk93% (14)
- NCP SenalDocument2 pagesNCP SenalJeyser T. GamutiaNo ratings yet
- Nervous System WorksheetDocument2 pagesNervous System WorksheetCamille Comas100% (2)
- Syllabus-Neuroscience 10 Neuroscience in 21st Century-2012FallDocument4 pagesSyllabus-Neuroscience 10 Neuroscience in 21st Century-2012FallJerikko Timm AgatepNo ratings yet
- Neuro Exam SchemeDocument229 pagesNeuro Exam SchemeRanjith KumarNo ratings yet
- Surgery For LBP - DR ManaekDocument44 pagesSurgery For LBP - DR ManaekArsyad MustaminNo ratings yet
- Approaching Acute Vertigo With Diplopia - A Rare Skew Deviation in Vestibular NeuritisDocument7 pagesApproaching Acute Vertigo With Diplopia - A Rare Skew Deviation in Vestibular NeuritisRudolfGerNo ratings yet
- Sensasi Bunyi Emmelia TriciaDocument2 pagesSensasi Bunyi Emmelia TriciaKhaliezs El KhawarizmiNo ratings yet
- Nanotechnology in Biomedical ApplicationsDocument17 pagesNanotechnology in Biomedical ApplicationsAbhiroop KumarNo ratings yet
- Unit 14Document4 pagesUnit 14Fitriana Noor SabrinaNo ratings yet
- CF Host Dept List 2023 24 v12Document111 pagesCF Host Dept List 2023 24 v12Antal Dorin CristianNo ratings yet
- Slide Management Vertigo in Daily PracticeDocument37 pagesSlide Management Vertigo in Daily PracticeHendrikkus AgustinNo ratings yet
- Trigeminal NeuralgiaDocument37 pagesTrigeminal Neuralgiawahyu purnamaNo ratings yet
- Diazepam Drug StudyDocument4 pagesDiazepam Drug StudyCheezy BreadNo ratings yet
- The Brilliance of The BrainDocument5 pagesThe Brilliance of The Brainapi-219083677No ratings yet
- Arteri Cerebellar: Presenter: Dr. Andre Lona Moderator: Dr. Iskandar Nasution, SP.S, FINSDocument40 pagesArteri Cerebellar: Presenter: Dr. Andre Lona Moderator: Dr. Iskandar Nasution, SP.S, FINSAlon RiderNo ratings yet
- Neuroscience For Architecture How Building DesignDocument8 pagesNeuroscience For Architecture How Building DesignKarla CarrascoNo ratings yet
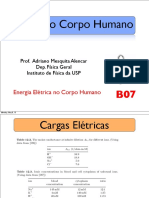
- Física Do Corpo Humano: Prof. Adriano Mesquita Alencar Dep. Física Geral Instituto de Física Da USPDocument31 pagesFísica Do Corpo Humano: Prof. Adriano Mesquita Alencar Dep. Física Geral Instituto de Física Da USPMariaSuzanaDiazNo ratings yet
- Soal Ikfr Unair 2019 - EditDocument5 pagesSoal Ikfr Unair 2019 - EditFusarina MumpuniNo ratings yet
- Cns QuestionsDocument18 pagesCns QuestionsVarun B RenukappaNo ratings yet