Download as pdf or txt
You might also like
- IOM NetProDual Daikin Rev 4 PDFDocument15 pagesIOM NetProDual Daikin Rev 4 PDFVin Ken0% (1)
- Audit Checklist For Purified Water SystemDocument2 pagesAudit Checklist For Purified Water Systempradeep28100171% (7)
- Anafilaxia y LatexDocument17 pagesAnafilaxia y LatexMARIA JOSE MARIN GOMEZNo ratings yet
- Seizures in Infancy in The Offspring of Women With Epilepsy 2019Document5 pagesSeizures in Infancy in The Offspring of Women With Epilepsy 2019Josefco RiveroNo ratings yet
- Woo 2017Document4 pagesWoo 2017Manickam BlatzNo ratings yet
- Alpha-1 Antitrypsin Deficiency and Pregnancy Complications and Birth Outcomes - A Population-Based Cohort Study in DenmarkDocument14 pagesAlpha-1 Antitrypsin Deficiency and Pregnancy Complications and Birth Outcomes - A Population-Based Cohort Study in Denmarkfasya azzahraNo ratings yet
- Chakravarty 2005Document8 pagesChakravarty 2005Sergio Henrique O. SantosNo ratings yet
- Biology 11 01608Document14 pagesBiology 11 01608Siti Zainab Bani PurwanaNo ratings yet
- Amniotic Fluid Embolism: Irene Stafford, MD, Jeanne She Eld, MDDocument9 pagesAmniotic Fluid Embolism: Irene Stafford, MD, Jeanne She Eld, MDChristian JuarezNo ratings yet
- Less Is More Modern NeonatologyDocument11 pagesLess Is More Modern NeonatologyEN BUNo ratings yet
- PIIS0016508506008651Document29 pagesPIIS0016508506008651Ongoongoseven b. e. bNo ratings yet
- Anaphylaxis in Children: Current Understanding and Key Issues in Diagnosis and TreatmentDocument9 pagesAnaphylaxis in Children: Current Understanding and Key Issues in Diagnosis and TreatmentangsetNo ratings yet
- Autism, Inflammatory Bowel Disease, and MMR VaccineDocument1 pageAutism, Inflammatory Bowel Disease, and MMR VaccineSinn VolleNo ratings yet
- WILKERSONDocument17 pagesWILKERSONkevina suwandiNo ratings yet
- Pneumonia in PregnancyDocument8 pagesPneumonia in PregnancymeliabudiNo ratings yet
- Dengue in Pregnancy: An Under-Reported Illness, With Special Reference To Other Existing Co-InfectionsDocument3 pagesDengue in Pregnancy: An Under-Reported Illness, With Special Reference To Other Existing Co-InfectionsLeonardoMartínezNo ratings yet
- Antipsikotik Pregnancy 3Document9 pagesAntipsikotik Pregnancy 3ThalNo ratings yet
- Neonatal Seizures in Calabar: A Revisit: J. J. Udo, M. E. Eyong, M. U. Anah, I. S. Etuk, C. I. Uzomba and A. A. AsindiDocument7 pagesNeonatal Seizures in Calabar: A Revisit: J. J. Udo, M. E. Eyong, M. U. Anah, I. S. Etuk, C. I. Uzomba and A. A. Asindiambachew bizunehNo ratings yet
- ANESTHESIOLOGY (R) 2016 - Refresher Course Lecture Summaries副本(被拖移)Document9 pagesANESTHESIOLOGY (R) 2016 - Refresher Course Lecture Summaries副本(被拖移)Han biaoNo ratings yet
- Acute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisDocument6 pagesAcute Pyelonephritis in Pregnancy: An 18-Year Retrospective AnalysisIntan Wahyu CahyaniNo ratings yet
- Mcdonnell 2013Document8 pagesMcdonnell 2013Erlyn SevilleNo ratings yet
- Pregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninDocument5 pagesPregnancy Complications and Outcomes in Women With Epilepsy: Mirzaei Fatemeh, Ebrahimi B. NazaninMentari SetiawatiNo ratings yet
- Jurnal KehamilanDocument13 pagesJurnal KehamilanNuraini Putri UtamiNo ratings yet
- Final Research Paper 1 Enc 1102 Tamryn Webb-GurleyDocument11 pagesFinal Research Paper 1 Enc 1102 Tamryn Webb-Gurleyapi-490436143100% (1)
- Jurnal Abrupsio PlasentaDocument13 pagesJurnal Abrupsio Plasentaperussi pranadiptaNo ratings yet
- Acr 23251Document5 pagesAcr 23251Krisna PutraNo ratings yet
- Compli UCI GestaciónDocument4 pagesCompli UCI GestaciónAmanqui Alex DerlyNo ratings yet
- Activity 1-13 StudentDocument3 pagesActivity 1-13 StudentTian KevinNo ratings yet
- American J Hematol - 2022 - Bussel - Romiplostim Use in Pregnant Women With Immune ThrombocytopeniaDocument10 pagesAmerican J Hematol - 2022 - Bussel - Romiplostim Use in Pregnant Women With Immune ThrombocytopeniaAfnindyas AtikaNo ratings yet
- AbruptionDocument13 pagesAbruptionMauricio Lopez MejiaNo ratings yet
- Clinical Profiles of Patients With Wheat Induced ADocument11 pagesClinical Profiles of Patients With Wheat Induced AjosehannaNo ratings yet
- Hypersensitivity To Pyrazolones: Micha LevyDocument4 pagesHypersensitivity To Pyrazolones: Micha Levydario2711No ratings yet
- Obstetric Infections and Clinical Characteristics of Maternal Sepsis: A Hospital Based Retrospective Cohort StudyDocument12 pagesObstetric Infections and Clinical Characteristics of Maternal Sepsis: A Hospital Based Retrospective Cohort StudyblanquishemNo ratings yet
- Hookworm-Related Anaemia Among Pregnant Women: A Systematic ReviewDocument10 pagesHookworm-Related Anaemia Among Pregnant Women: A Systematic ReviewAjay DNo ratings yet
- Antimicrobial Therapy and Late Onset SepsisDocument10 pagesAntimicrobial Therapy and Late Onset SepsisKendy LópezNo ratings yet
- Guia Wao Anafilaxia 2015Document16 pagesGuia Wao Anafilaxia 2015Diego Alexander ChingoNo ratings yet
- AbruptionDocument13 pagesAbruptionAnghelo Aldair Velásquez CarrilloNo ratings yet
- Maternal Morbidity and Mortality From Severe Sepsis: A National Cohort StudyDocument8 pagesMaternal Morbidity and Mortality From Severe Sepsis: A National Cohort StudyAbdu GodanaNo ratings yet
- Lepine2018 PDFDocument6 pagesLepine2018 PDFYaddi Fernanda Solarte MenjuraNo ratings yet
- An-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Document4 pagesAn-Evaluation-Of-Risk-Factors-In-Cases-Of-Perinatal-Asphyxia-9563 2021Chiki CacaNo ratings yet
- Preterm Labour, Antibiotics, and Cerebral Palsy: Scientific Impact Paper No. 33Document8 pagesPreterm Labour, Antibiotics, and Cerebral Palsy: Scientific Impact Paper No. 33oscarNo ratings yet
- New PDFDocument6 pagesNew PDFDann RoblezNo ratings yet
- Piis0190962207010626Document6 pagesPiis0190962207010626Tiara MardalifaNo ratings yet
- Aurelio - Afe PBLDocument26 pagesAurelio - Afe PBLLyca Mae AurelioNo ratings yet
- Journal Ectopic Pregnancy-A Rising TrendDocument5 pagesJournal Ectopic Pregnancy-A Rising TrendEricNo ratings yet
- Aplastic Anemia During Pregnancy: A Review of Obstetric and Anesthetic ConsiderationsDocument9 pagesAplastic Anemia During Pregnancy: A Review of Obstetric and Anesthetic Considerationsalston96No ratings yet
- Management of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice GuidelineDocument6 pagesManagement of Varicella Infection (Chickenpox) in Pregnancy: Sogc Clinical Practice GuidelineAndi NugrohoNo ratings yet
- Manejo Cancer in Pregnancy Fetal and Neonatal OutcomesDocument17 pagesManejo Cancer in Pregnancy Fetal and Neonatal OutcomesLaura LealNo ratings yet
- Tinjauan Pustaka: DefinisiDocument19 pagesTinjauan Pustaka: DefinisiKhandar YosuaNo ratings yet
- Physiological Reviews: Pregnancy and Covid-19Document17 pagesPhysiological Reviews: Pregnancy and Covid-19fajar cahyadiNo ratings yet
- Syphilis in PregnancyDocument17 pagesSyphilis in PregnancyKevin Stanley HalimNo ratings yet
- 1564 3951 1 PBDocument5 pages1564 3951 1 PBsandy candyNo ratings yet
- PPEpidemiol 97Document13 pagesPPEpidemiol 97umberto de vonderweidNo ratings yet
- Predictores Tempranos Del Síndrome de Guillain-Barré en El Curso de La Vida de Las MujeresDocument9 pagesPredictores Tempranos Del Síndrome de Guillain-Barré en El Curso de La Vida de Las Mujeresfrancisco bacaNo ratings yet
- PIIS2210778916303701Document2 pagesPIIS2210778916303701Fatimah AssagafNo ratings yet
- P ('t':'3', 'I':'3053807383') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document4 pagesP ('t':'3', 'I':'3053807383') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Ni Wayan Ana PsNo ratings yet
- Kern IcterusDocument4 pagesKern IcterusAlwin SoetandarNo ratings yet
- Ni Hms 775233Document16 pagesNi Hms 775233Mikhail NurhariNo ratings yet
- Celiac and Infertility Sana'a2018Document3 pagesCeliac and Infertility Sana'a2018gamal attamNo ratings yet
- Acute Respiratory Distress Syndrome Among Premature Neonates: Prevalence, Mortality Rate and Risk Factors of MortalityDocument5 pagesAcute Respiratory Distress Syndrome Among Premature Neonates: Prevalence, Mortality Rate and Risk Factors of MortalityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Food Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementFrom EverandFood Protein Induced Enterocolitis (FPIES): Diagnosis and ManagementTerri Faye Brown-WhitehornNo ratings yet
- Pediatric Immunology: A Case-Based Collection with MCQs, Volume 2From EverandPediatric Immunology: A Case-Based Collection with MCQs, Volume 2No ratings yet
- Analysis of Indian Paint IndustryDocument7 pagesAnalysis of Indian Paint IndustryJoshua FinnyNo ratings yet
- Region III Tourism MasterPlanDocument34 pagesRegion III Tourism MasterPlanVenus Leilani Villanueva-GranadoNo ratings yet
- 30MHZ AM ReceiverDocument1 page30MHZ AM ReceiverrujNo ratings yet
- PRIME: Phobos Reconnaissance & International Mars ExplorationDocument1 pagePRIME: Phobos Reconnaissance & International Mars ExplorationRick FeedNo ratings yet
- ATIC112Document1 pageATIC112lennon rNo ratings yet
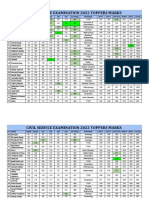
- Selected Candidates Marks CSE 2022Document6 pagesSelected Candidates Marks CSE 2022hara vardhan reddy naruNo ratings yet
- Carlip-Is Quantum Gravity Necessary? (2008)Document8 pagesCarlip-Is Quantum Gravity Necessary? (2008)bhpliaoNo ratings yet
- PURSUIT Newsletter No. 34, April 1976 - Ivan T. SandersonDocument28 pagesPURSUIT Newsletter No. 34, April 1976 - Ivan T. SandersonuforteanNo ratings yet
- Lecture 12 - Unit Sample Response For Signals and SystemDocument4 pagesLecture 12 - Unit Sample Response For Signals and SystemSergeMghabghabNo ratings yet
- B. I Felt So Bad About It.: 3. The Best Answer To Fill The Blank Is ..Document8 pagesB. I Felt So Bad About It.: 3. The Best Answer To Fill The Blank Is ..yepe prtitamaNo ratings yet
- Sources of Stem CellsDocument13 pagesSources of Stem CellsAnshi AroraNo ratings yet
- Quantum-Like Networks: An Approach To Neural Behavior Through Their Mathematics and Logic 1st Edition Stephen A. SelesnickDocument70 pagesQuantum-Like Networks: An Approach To Neural Behavior Through Their Mathematics and Logic 1st Edition Stephen A. Selesnickamberavila557619100% (5)
- Nega Bizuye To New Cobble RoadDocument36 pagesNega Bizuye To New Cobble RoadAsmerom MosinehNo ratings yet
- Mf1S70Yyx/V1: 1. General DescriptionDocument41 pagesMf1S70Yyx/V1: 1. General DescriptionPintér SándorNo ratings yet
- q1 Week 1 PhilosophyDocument22 pagesq1 Week 1 PhilosophyStiffany FlordelizaNo ratings yet
- B02. Junior Engineer MechanicalDocument115 pagesB02. Junior Engineer MechanicalRafay MohiuddinNo ratings yet
- Hello, Hello and Hello Vol 2Document257 pagesHello, Hello and Hello Vol 2muhammad anginNo ratings yet
- WWW - Swrs.ap - Gov.in: of 1753 Vacant Posts of Teachers, Special Teachers & Staff NursesDocument14 pagesWWW - Swrs.ap - Gov.in: of 1753 Vacant Posts of Teachers, Special Teachers & Staff NursesVijay KsheresagarNo ratings yet
- Formulas Physics B CH 11, 12, 22, 23, 24, 25 WavesDocument6 pagesFormulas Physics B CH 11, 12, 22, 23, 24, 25 WavesEpic WinNo ratings yet
- Drummond - Conceptualizing The Efficacy of Vipassana Meditation As Taught by SN GoenkaDocument18 pagesDrummond - Conceptualizing The Efficacy of Vipassana Meditation As Taught by SN GoenkamikeXF100% (1)
- Aragasi, Jonaysa Module11-Ba2ma-Nstp2Document5 pagesAragasi, Jonaysa Module11-Ba2ma-Nstp2Jon AragasiNo ratings yet
- Signal Integrity Characterization Techniques Agilent PDFDocument806 pagesSignal Integrity Characterization Techniques Agilent PDFlusinNo ratings yet
- Date of Test: Non-Destructive Testing (NDT) / Ultrasonic Pulse Velocity (UPV) & Compressive Testing Strenght (CTM)Document65 pagesDate of Test: Non-Destructive Testing (NDT) / Ultrasonic Pulse Velocity (UPV) & Compressive Testing Strenght (CTM)GaneshNo ratings yet
- D3K D4K D5K TRGDocument111 pagesD3K D4K D5K TRGDania Zataline GusenkaNo ratings yet
- MCQ's For Operating SystemsDocument11 pagesMCQ's For Operating SystemsYussif AliNo ratings yet
- Reed Switch Appln PDFDocument15 pagesReed Switch Appln PDFJeeva BharathiNo ratings yet
- TOEFL Test 1Document10 pagesTOEFL Test 1Chantha Neav ChanthaNo ratings yet
- List Down The Types of Connective Tissues and Their FunctionsDocument3 pagesList Down The Types of Connective Tissues and Their FunctionsZahir Jayvee Gayak IINo ratings yet