
Prevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian City
Prevalence and Antimicrobial Resistance Profile of Pathogens Isolated From Patients With Urine Tract Infections Admitted To A University Hospital in A Medium-Sized Brazilian City
You might also like
- Title: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupDocument4 pagesTitle: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupFatima MNo ratings yet
- 11 The Epidemiology of Intestinal MicrosporidiosisDocument7 pages11 The Epidemiology of Intestinal MicrosporidiosisDaniel VargasNo ratings yet
- Laboratory Diagnosis of Urinary Tract InfectionsDocument9 pagesLaboratory Diagnosis of Urinary Tract InfectionsArturo OrtúñezNo ratings yet
- Laboratory Diagnosis of Urinary Tract Infections in Adult PatientsDocument9 pagesLaboratory Diagnosis of Urinary Tract Infections in Adult PatientsTony ZhangNo ratings yet
- Brink 2002Document8 pagesBrink 2002Diego SarmientoNo ratings yet
- Resistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaDocument4 pagesResistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaMiguel AnguianoNo ratings yet
- 10) Blood Culture Contaminants - S.dawsonDocument10 pages10) Blood Culture Contaminants - S.dawsonimaguestuserNo ratings yet
- Laboratory Diagnosis of Urinary Tract Infections in Adult PatientsDocument9 pagesLaboratory Diagnosis of Urinary Tract Infections in Adult PatientsAngga Krisna ArthaNo ratings yet
- Urinary Tract InfectionsDocument13 pagesUrinary Tract InfectionsJeannina Alvarez YannarellaNo ratings yet
- Lab UtiDocument9 pagesLab UtiAni RahayuNo ratings yet
- Clinical Therapy of UTI in Children Under The Age of Five Varies WidelyDocument21 pagesClinical Therapy of UTI in Children Under The Age of Five Varies WidelyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 10.1515 - Labmed 2021 0085Document13 pages10.1515 - Labmed 2021 0085Tony ZhangNo ratings yet
- Risk Factors and The Resistance Mechanisms Involved in Pseudomonas Aeruginosa Mutation in Critically Ill PatientsDocument9 pagesRisk Factors and The Resistance Mechanisms Involved in Pseudomonas Aeruginosa Mutation in Critically Ill PatientsElsiana LaurenciaNo ratings yet
- Jurnal Interna 123456Document9 pagesJurnal Interna 123456vonnyandira28No ratings yet
- Bacteriuria in Individuals Who Become Delirious: CommentaryDocument3 pagesBacteriuria in Individuals Who Become Delirious: CommentaryGabreilla HanochNo ratings yet
- Newly Identified Viruses in Human Gastroenteritis: Espid R RDocument4 pagesNewly Identified Viruses in Human Gastroenteritis: Espid R RArianne LasamNo ratings yet
- Mojbm 03 00082Document5 pagesMojbm 03 00082Sohrab RohaneNo ratings yet
- 43 Pukar EtalDocument3 pages43 Pukar EtaleditorijmrhsNo ratings yet
- Antimicrobial Susceptibility Pattern of Urinary Pathogens Isolated From Two Tertiary Hospitals in Southwestern NigeriaDocument11 pagesAntimicrobial Susceptibility Pattern of Urinary Pathogens Isolated From Two Tertiary Hospitals in Southwestern NigeriaKenneth Mark B. TevesNo ratings yet
- Urinary GuidelinesDocument9 pagesUrinary GuidelinesCabinet VeterinarNo ratings yet
- Highly Effective Against EsblDocument9 pagesHighly Effective Against Esblgaurav rawalNo ratings yet
- Antibiotic Sensitivity of Gram-Negative Bacteria Isolated From Urine Sample of Patient in Delsu Health CentreDocument10 pagesAntibiotic Sensitivity of Gram-Negative Bacteria Isolated From Urine Sample of Patient in Delsu Health CentreAmado Hernandez BautistaNo ratings yet
- 1 s2.0 S009042951930963X Main PDFDocument8 pages1 s2.0 S009042951930963X Main PDFCris FischerNo ratings yet
- Cambio en La Susceptibilidad de Escherichia Coli y Aumento de LaDocument18 pagesCambio en La Susceptibilidad de Escherichia Coli y Aumento de LaNelly Castro GordilloNo ratings yet
- Changing The Paradigm For Hospital Outbreak Detection by Leading With Genomic Surveillance of Nosocomial PathogensDocument7 pagesChanging The Paradigm For Hospital Outbreak Detection by Leading With Genomic Surveillance of Nosocomial PathogensDalibor P. DrljacaNo ratings yet
- The Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioDocument7 pagesThe Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioMaharaniNo ratings yet
- IMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSDocument5 pagesIMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSjavelezhNo ratings yet
- MaybeDocument4 pagesMaybepertama bestNo ratings yet
- Anuradha NDocument4 pagesAnuradha NIJAMNo ratings yet
- Bloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesDocument4 pagesBloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesrasioputraNo ratings yet
- Microbial Profile and Antibiotic Sensitivity Pattern in Bile Cultures From Endoscopic Retrograde Cholangiography PatientsDocument12 pagesMicrobial Profile and Antibiotic Sensitivity Pattern in Bile Cultures From Endoscopic Retrograde Cholangiography PatientsMandar PatilNo ratings yet
- Far Eastern University: Evidence Based NursingDocument4 pagesFar Eastern University: Evidence Based NursingKhaye MendozaNo ratings yet
- Vol. 3 No. 02 (2024) 102-117Document16 pagesVol. 3 No. 02 (2024) 102-117muradchy321No ratings yet
- Prevalence of Urinary Tract Infections and Their Antibiotic Sensitivity in Tertiary Care Hospital LahoreDocument5 pagesPrevalence of Urinary Tract Infections and Their Antibiotic Sensitivity in Tertiary Care Hospital LahoreInternational Organization of Scientific Research (IOSR)No ratings yet
- BJBMS 14 227Document7 pagesBJBMS 14 227enesNo ratings yet
- Microbiology Laboratory: By: Edessa S. Valenzuela, RMTDocument16 pagesMicrobiology Laboratory: By: Edessa S. Valenzuela, RMTKaren Urbien Del Valle - CabilloNo ratings yet
- Acute Bacterial Gastroenteritis: A Study of Adult Patients With Positive Stool Cultures Treated in The Emergency DepartmentDocument4 pagesAcute Bacterial Gastroenteritis: A Study of Adult Patients With Positive Stool Cultures Treated in The Emergency DepartmentJuvel PerochoNo ratings yet
- Rotavirus en La Diarrea AgudaDocument6 pagesRotavirus en La Diarrea Agudajb.mgarrido96No ratings yet
- PDFDocument7 pagesPDFFredNo ratings yet
- Atencio Azucena Besares Special ProblemDocument18 pagesAtencio Azucena Besares Special ProblemShane Catherine BesaresNo ratings yet
- Detection of Typhoid CarriersDocument6 pagesDetection of Typhoid CarriersClarestaNo ratings yet
- 2016 Article 645Document10 pages2016 Article 645Betharia TriayuNo ratings yet
- ISSN: 2616 - 0668: UjmrDocument8 pagesISSN: 2616 - 0668: UjmrUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Received: Accepted:: UJMR, Volume 5 Number 1, June, 2020, PP 18 - 23Document7 pagesReceived: Accepted:: UJMR, Volume 5 Number 1, June, 2020, PP 18 - 23UMYU Journal of Microbiology Research (UJMR)No ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- Isolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiaDocument12 pagesIsolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiadrpklalNo ratings yet
- A Study On The Bacteriological Profile of UrinaryDocument7 pagesA Study On The Bacteriological Profile of Urinarycendy oktariNo ratings yet
- 335 FullDocument4 pages335 FullJinu AuraNo ratings yet
- The+Urinary+Microbiome+AssociatedDocument8 pagesThe+Urinary+Microbiome+AssociatedcamilaNo ratings yet
- Molecular DiagnosDocument2 pagesMolecular Diagnos128182No ratings yet
- Antibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenDocument5 pagesAntibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenLavfy NjlaaNo ratings yet
- Cryptosporidiosis in Children During A Massive Waterborne Outbreak in Milwaukee Wisconsin Clinical Laboratory and Epidemiologic FindingsDocument8 pagesCryptosporidiosis in Children During A Massive Waterborne Outbreak in Milwaukee Wisconsin Clinical Laboratory and Epidemiologic FindingsJOSE LUIS CARRASCO CHUQUILLANQUINo ratings yet
- Original Article - EnterococcusDocument7 pagesOriginal Article - EnterococcusQworldNo ratings yet
- 546-Texto Del Artículo-2262-1-10-20200124Document14 pages546-Texto Del Artículo-2262-1-10-20200124Paul Coacalla JuaresNo ratings yet
- Comparative Diagnosis of Urinary Tract Infection (UTI) Using Urinary Nitrite and Significant Bacteriuria (SBU)Document10 pagesComparative Diagnosis of Urinary Tract Infection (UTI) Using Urinary Nitrite and Significant Bacteriuria (SBU)Luis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- CandaDocument21 pagesCandazurique32No ratings yet
- EJMCM - Volume 8 - Issue 3 - Pages 2605-2615Document11 pagesEJMCM - Volume 8 - Issue 3 - Pages 2605-2615dr_joe23No ratings yet
- Different Diagnostic Procedure of Typhoid Fever ADocument8 pagesDifferent Diagnostic Procedure of Typhoid Fever AdjebrutNo ratings yet
- Research Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriaDocument6 pagesResearch Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriariniNo ratings yet
- Comprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsFrom EverandComprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsNo ratings yet
- Genato BSP2G123 M5 Case StudiesDocument4 pagesGenato BSP2G123 M5 Case StudiesCHARLES RONALD GENATONo ratings yet
- My Co BacteriumDocument15 pagesMy Co BacteriumPatrickNo ratings yet
- Exrcise Topic4 Infection ControlDocument3 pagesExrcise Topic4 Infection Controlfroosedd777No ratings yet
- Raws 2020-2021 Final Performance TaskDocument3 pagesRaws 2020-2021 Final Performance TaskEDMAR POLVOROZANo ratings yet
- Highlighted Lange Microbiology (Some Chapter)Document66 pagesHighlighted Lange Microbiology (Some Chapter)naimNo ratings yet
- New Microsoft Word Document 1Document25 pagesNew Microsoft Word Document 1Aleksandar DimovskiNo ratings yet
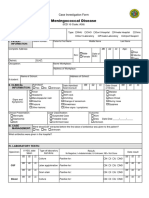
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- ABSTRACT BOOK LA SOVE 2022 - Final VersionDocument120 pagesABSTRACT BOOK LA SOVE 2022 - Final VersionMARLON MAURICIO ARDILA CHAVEZNo ratings yet
- Case Files® EnterococcusDocument4 pagesCase Files® EnterococcusAHMAD ADE SAPUTRANo ratings yet
- COVID 19 Risk Assessment High PeakDocument4 pagesCOVID 19 Risk Assessment High PeakShayan KhanNo ratings yet
- UNTAN Neurosains Parasit 2008Document72 pagesUNTAN Neurosains Parasit 2008Indhy Windhy ValentineNo ratings yet
- Severe Acute Respiratory SyndromeDocument12 pagesSevere Acute Respiratory SyndromeprincejeyarajpjsNo ratings yet
- Drug Study - AlgesiaDocument4 pagesDrug Study - AlgesiaRonel ResurricionNo ratings yet
- AspergillusDocument13 pagesAspergillusangelNo ratings yet
- Sexually Transmitted Diseases: PresentationDocument17 pagesSexually Transmitted Diseases: PresentationBonface NdunguNo ratings yet
- What Is ScabiesDocument7 pagesWhat Is ScabiesKenNo ratings yet
- AIDS/HIV An Overview 1Document7 pagesAIDS/HIV An Overview 1tiffrenfitNo ratings yet
- StridorDocument1 pageStridorhrg79qzwc2No ratings yet
- Chicken Pox ReportDocument25 pagesChicken Pox ReportDyanne Bautista100% (1)
- Micro para OSCE For YL6 BacteriaDocument2 pagesMicro para OSCE For YL6 Bacteriagzldiwa100% (1)
- Imci 1Document78 pagesImci 1nucahersheyskatNo ratings yet
- CONTINGENCY PLAN For Limited Face To FaceDocument15 pagesCONTINGENCY PLAN For Limited Face To FaceMaricar Dimas100% (3)
- Level of Awareness and Attitude of Grade 12 GAS Students On Selected Sexually Transmitted Diseases Quantitative Research ProposalDocument37 pagesLevel of Awareness and Attitude of Grade 12 GAS Students On Selected Sexually Transmitted Diseases Quantitative Research ProposalCharlz HizonNo ratings yet
- Parasitology Study GuideDocument35 pagesParasitology Study GuidesamkennedybusinessNo ratings yet
- Employee Health Policy TemplateDocument4 pagesEmployee Health Policy Templatebromberg.alexaNo ratings yet
- Carmona Uscanga Luis Angel Hernandez Muñoz Maria Fernanda Ortiz Jimenez Mario Enrique Ramos Rivera Cristian Eduardo Rodriguez Olmos Araceli Ssanchez Pablo Rosario Vazquez Blancas Lisset AnahiDocument11 pagesCarmona Uscanga Luis Angel Hernandez Muñoz Maria Fernanda Ortiz Jimenez Mario Enrique Ramos Rivera Cristian Eduardo Rodriguez Olmos Araceli Ssanchez Pablo Rosario Vazquez Blancas Lisset AnahiItzel SanchezNo ratings yet
- For Professional and in Vitro Diagnostic Use OnlyDocument6 pagesFor Professional and in Vitro Diagnostic Use OnlySheilla DifaNo ratings yet
- Prevalence of Giardiasis and Personal Hygiene Conditions in Pre-School Students in KB-TK Al Amin Paciran LamonganDocument7 pagesPrevalence of Giardiasis and Personal Hygiene Conditions in Pre-School Students in KB-TK Al Amin Paciran LamonganMadhury DixitNo ratings yet
- Micropara-Lab c5-c7Document10 pagesMicropara-Lab c5-c7Monica JoyceNo ratings yet
- Orchid Virus Diseases in Taiwan and Their Control StrategiesDocument54 pagesOrchid Virus Diseases in Taiwan and Their Control StrategiesPham Lanphuong100% (1)























































































Download as pdf or txt
You might also like
- Title: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupDocument4 pagesTitle: Culture and Sensitivity Pattern of Urinary Tract Infection Among Women of Reproductive Age GroupFatima MNo ratings yet
- 11 The Epidemiology of Intestinal MicrosporidiosisDocument7 pages11 The Epidemiology of Intestinal MicrosporidiosisDaniel VargasNo ratings yet
- Laboratory Diagnosis of Urinary Tract InfectionsDocument9 pagesLaboratory Diagnosis of Urinary Tract InfectionsArturo OrtúñezNo ratings yet
- Laboratory Diagnosis of Urinary Tract Infections in Adult PatientsDocument9 pagesLaboratory Diagnosis of Urinary Tract Infections in Adult PatientsTony ZhangNo ratings yet
- Brink 2002Document8 pagesBrink 2002Diego SarmientoNo ratings yet
- Resistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaDocument4 pagesResistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaMiguel AnguianoNo ratings yet
- 10) Blood Culture Contaminants - S.dawsonDocument10 pages10) Blood Culture Contaminants - S.dawsonimaguestuserNo ratings yet
- Laboratory Diagnosis of Urinary Tract Infections in Adult PatientsDocument9 pagesLaboratory Diagnosis of Urinary Tract Infections in Adult PatientsAngga Krisna ArthaNo ratings yet
- Urinary Tract InfectionsDocument13 pagesUrinary Tract InfectionsJeannina Alvarez YannarellaNo ratings yet
- Lab UtiDocument9 pagesLab UtiAni RahayuNo ratings yet
- Clinical Therapy of UTI in Children Under The Age of Five Varies WidelyDocument21 pagesClinical Therapy of UTI in Children Under The Age of Five Varies WidelyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 10.1515 - Labmed 2021 0085Document13 pages10.1515 - Labmed 2021 0085Tony ZhangNo ratings yet
- Risk Factors and The Resistance Mechanisms Involved in Pseudomonas Aeruginosa Mutation in Critically Ill PatientsDocument9 pagesRisk Factors and The Resistance Mechanisms Involved in Pseudomonas Aeruginosa Mutation in Critically Ill PatientsElsiana LaurenciaNo ratings yet
- Jurnal Interna 123456Document9 pagesJurnal Interna 123456vonnyandira28No ratings yet
- Bacteriuria in Individuals Who Become Delirious: CommentaryDocument3 pagesBacteriuria in Individuals Who Become Delirious: CommentaryGabreilla HanochNo ratings yet
- Newly Identified Viruses in Human Gastroenteritis: Espid R RDocument4 pagesNewly Identified Viruses in Human Gastroenteritis: Espid R RArianne LasamNo ratings yet
- Mojbm 03 00082Document5 pagesMojbm 03 00082Sohrab RohaneNo ratings yet
- 43 Pukar EtalDocument3 pages43 Pukar EtaleditorijmrhsNo ratings yet
- Antimicrobial Susceptibility Pattern of Urinary Pathogens Isolated From Two Tertiary Hospitals in Southwestern NigeriaDocument11 pagesAntimicrobial Susceptibility Pattern of Urinary Pathogens Isolated From Two Tertiary Hospitals in Southwestern NigeriaKenneth Mark B. TevesNo ratings yet
- Urinary GuidelinesDocument9 pagesUrinary GuidelinesCabinet VeterinarNo ratings yet
- Highly Effective Against EsblDocument9 pagesHighly Effective Against Esblgaurav rawalNo ratings yet
- Antibiotic Sensitivity of Gram-Negative Bacteria Isolated From Urine Sample of Patient in Delsu Health CentreDocument10 pagesAntibiotic Sensitivity of Gram-Negative Bacteria Isolated From Urine Sample of Patient in Delsu Health CentreAmado Hernandez BautistaNo ratings yet
- 1 s2.0 S009042951930963X Main PDFDocument8 pages1 s2.0 S009042951930963X Main PDFCris FischerNo ratings yet
- Cambio en La Susceptibilidad de Escherichia Coli y Aumento de LaDocument18 pagesCambio en La Susceptibilidad de Escherichia Coli y Aumento de LaNelly Castro GordilloNo ratings yet
- Changing The Paradigm For Hospital Outbreak Detection by Leading With Genomic Surveillance of Nosocomial PathogensDocument7 pagesChanging The Paradigm For Hospital Outbreak Detection by Leading With Genomic Surveillance of Nosocomial PathogensDalibor P. DrljacaNo ratings yet
- The Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioDocument7 pagesThe Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioMaharaniNo ratings yet
- IMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSDocument5 pagesIMMUNOLOGICAL AND BIOCHEMICAL RESPONSE FROM OLDER ADULTS WITH URINARY TRACT INFECTION TO UROPATHOGENIC Escherichia Coli VIRULENCE FACTORSjavelezhNo ratings yet
- MaybeDocument4 pagesMaybepertama bestNo ratings yet
- Anuradha NDocument4 pagesAnuradha NIJAMNo ratings yet
- Bloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesDocument4 pagesBloodstream Infections in Hospitalized Children: Epidemiology and Antimicrobial SusceptibilitiesrasioputraNo ratings yet
- Microbial Profile and Antibiotic Sensitivity Pattern in Bile Cultures From Endoscopic Retrograde Cholangiography PatientsDocument12 pagesMicrobial Profile and Antibiotic Sensitivity Pattern in Bile Cultures From Endoscopic Retrograde Cholangiography PatientsMandar PatilNo ratings yet
- Far Eastern University: Evidence Based NursingDocument4 pagesFar Eastern University: Evidence Based NursingKhaye MendozaNo ratings yet
- Vol. 3 No. 02 (2024) 102-117Document16 pagesVol. 3 No. 02 (2024) 102-117muradchy321No ratings yet
- Prevalence of Urinary Tract Infections and Their Antibiotic Sensitivity in Tertiary Care Hospital LahoreDocument5 pagesPrevalence of Urinary Tract Infections and Their Antibiotic Sensitivity in Tertiary Care Hospital LahoreInternational Organization of Scientific Research (IOSR)No ratings yet
- BJBMS 14 227Document7 pagesBJBMS 14 227enesNo ratings yet
- Microbiology Laboratory: By: Edessa S. Valenzuela, RMTDocument16 pagesMicrobiology Laboratory: By: Edessa S. Valenzuela, RMTKaren Urbien Del Valle - CabilloNo ratings yet
- Acute Bacterial Gastroenteritis: A Study of Adult Patients With Positive Stool Cultures Treated in The Emergency DepartmentDocument4 pagesAcute Bacterial Gastroenteritis: A Study of Adult Patients With Positive Stool Cultures Treated in The Emergency DepartmentJuvel PerochoNo ratings yet
- Rotavirus en La Diarrea AgudaDocument6 pagesRotavirus en La Diarrea Agudajb.mgarrido96No ratings yet
- PDFDocument7 pagesPDFFredNo ratings yet
- Atencio Azucena Besares Special ProblemDocument18 pagesAtencio Azucena Besares Special ProblemShane Catherine BesaresNo ratings yet
- Detection of Typhoid CarriersDocument6 pagesDetection of Typhoid CarriersClarestaNo ratings yet
- 2016 Article 645Document10 pages2016 Article 645Betharia TriayuNo ratings yet
- ISSN: 2616 - 0668: UjmrDocument8 pagesISSN: 2616 - 0668: UjmrUMYU Journal of Microbiology Research (UJMR)No ratings yet
- Received: Accepted:: UJMR, Volume 5 Number 1, June, 2020, PP 18 - 23Document7 pagesReceived: Accepted:: UJMR, Volume 5 Number 1, June, 2020, PP 18 - 23UMYU Journal of Microbiology Research (UJMR)No ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- Isolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiaDocument12 pagesIsolation, Identification and Antibiogram of Coagulase Negative Tertiary Care Teaching Hospital, Jaipur, IndiadrpklalNo ratings yet
- A Study On The Bacteriological Profile of UrinaryDocument7 pagesA Study On The Bacteriological Profile of Urinarycendy oktariNo ratings yet
- 335 FullDocument4 pages335 FullJinu AuraNo ratings yet
- The+Urinary+Microbiome+AssociatedDocument8 pagesThe+Urinary+Microbiome+AssociatedcamilaNo ratings yet
- Molecular DiagnosDocument2 pagesMolecular Diagnos128182No ratings yet
- Antibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenDocument5 pagesAntibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenLavfy NjlaaNo ratings yet
- Cryptosporidiosis in Children During A Massive Waterborne Outbreak in Milwaukee Wisconsin Clinical Laboratory and Epidemiologic FindingsDocument8 pagesCryptosporidiosis in Children During A Massive Waterborne Outbreak in Milwaukee Wisconsin Clinical Laboratory and Epidemiologic FindingsJOSE LUIS CARRASCO CHUQUILLANQUINo ratings yet
- Original Article - EnterococcusDocument7 pagesOriginal Article - EnterococcusQworldNo ratings yet
- 546-Texto Del Artículo-2262-1-10-20200124Document14 pages546-Texto Del Artículo-2262-1-10-20200124Paul Coacalla JuaresNo ratings yet
- Comparative Diagnosis of Urinary Tract Infection (UTI) Using Urinary Nitrite and Significant Bacteriuria (SBU)Document10 pagesComparative Diagnosis of Urinary Tract Infection (UTI) Using Urinary Nitrite and Significant Bacteriuria (SBU)Luis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- CandaDocument21 pagesCandazurique32No ratings yet
- EJMCM - Volume 8 - Issue 3 - Pages 2605-2615Document11 pagesEJMCM - Volume 8 - Issue 3 - Pages 2605-2615dr_joe23No ratings yet
- Different Diagnostic Procedure of Typhoid Fever ADocument8 pagesDifferent Diagnostic Procedure of Typhoid Fever AdjebrutNo ratings yet
- Research Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriaDocument6 pagesResearch Article: Viral Agents of Diarrhea in Young Children in Two Primary Health Centers in Edo State, NigeriariniNo ratings yet
- Comprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsFrom EverandComprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsNo ratings yet
- Genato BSP2G123 M5 Case StudiesDocument4 pagesGenato BSP2G123 M5 Case StudiesCHARLES RONALD GENATONo ratings yet
- My Co BacteriumDocument15 pagesMy Co BacteriumPatrickNo ratings yet
- Exrcise Topic4 Infection ControlDocument3 pagesExrcise Topic4 Infection Controlfroosedd777No ratings yet
- Raws 2020-2021 Final Performance TaskDocument3 pagesRaws 2020-2021 Final Performance TaskEDMAR POLVOROZANo ratings yet
- Highlighted Lange Microbiology (Some Chapter)Document66 pagesHighlighted Lange Microbiology (Some Chapter)naimNo ratings yet
- New Microsoft Word Document 1Document25 pagesNew Microsoft Word Document 1Aleksandar DimovskiNo ratings yet
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- ABSTRACT BOOK LA SOVE 2022 - Final VersionDocument120 pagesABSTRACT BOOK LA SOVE 2022 - Final VersionMARLON MAURICIO ARDILA CHAVEZNo ratings yet
- Case Files® EnterococcusDocument4 pagesCase Files® EnterococcusAHMAD ADE SAPUTRANo ratings yet
- COVID 19 Risk Assessment High PeakDocument4 pagesCOVID 19 Risk Assessment High PeakShayan KhanNo ratings yet
- UNTAN Neurosains Parasit 2008Document72 pagesUNTAN Neurosains Parasit 2008Indhy Windhy ValentineNo ratings yet
- Severe Acute Respiratory SyndromeDocument12 pagesSevere Acute Respiratory SyndromeprincejeyarajpjsNo ratings yet
- Drug Study - AlgesiaDocument4 pagesDrug Study - AlgesiaRonel ResurricionNo ratings yet
- AspergillusDocument13 pagesAspergillusangelNo ratings yet
- Sexually Transmitted Diseases: PresentationDocument17 pagesSexually Transmitted Diseases: PresentationBonface NdunguNo ratings yet
- What Is ScabiesDocument7 pagesWhat Is ScabiesKenNo ratings yet
- AIDS/HIV An Overview 1Document7 pagesAIDS/HIV An Overview 1tiffrenfitNo ratings yet
- StridorDocument1 pageStridorhrg79qzwc2No ratings yet
- Chicken Pox ReportDocument25 pagesChicken Pox ReportDyanne Bautista100% (1)
- Micro para OSCE For YL6 BacteriaDocument2 pagesMicro para OSCE For YL6 Bacteriagzldiwa100% (1)
- Imci 1Document78 pagesImci 1nucahersheyskatNo ratings yet
- CONTINGENCY PLAN For Limited Face To FaceDocument15 pagesCONTINGENCY PLAN For Limited Face To FaceMaricar Dimas100% (3)
- Level of Awareness and Attitude of Grade 12 GAS Students On Selected Sexually Transmitted Diseases Quantitative Research ProposalDocument37 pagesLevel of Awareness and Attitude of Grade 12 GAS Students On Selected Sexually Transmitted Diseases Quantitative Research ProposalCharlz HizonNo ratings yet
- Parasitology Study GuideDocument35 pagesParasitology Study GuidesamkennedybusinessNo ratings yet
- Employee Health Policy TemplateDocument4 pagesEmployee Health Policy Templatebromberg.alexaNo ratings yet
- Carmona Uscanga Luis Angel Hernandez Muñoz Maria Fernanda Ortiz Jimenez Mario Enrique Ramos Rivera Cristian Eduardo Rodriguez Olmos Araceli Ssanchez Pablo Rosario Vazquez Blancas Lisset AnahiDocument11 pagesCarmona Uscanga Luis Angel Hernandez Muñoz Maria Fernanda Ortiz Jimenez Mario Enrique Ramos Rivera Cristian Eduardo Rodriguez Olmos Araceli Ssanchez Pablo Rosario Vazquez Blancas Lisset AnahiItzel SanchezNo ratings yet
- For Professional and in Vitro Diagnostic Use OnlyDocument6 pagesFor Professional and in Vitro Diagnostic Use OnlySheilla DifaNo ratings yet
- Prevalence of Giardiasis and Personal Hygiene Conditions in Pre-School Students in KB-TK Al Amin Paciran LamonganDocument7 pagesPrevalence of Giardiasis and Personal Hygiene Conditions in Pre-School Students in KB-TK Al Amin Paciran LamonganMadhury DixitNo ratings yet
- Micropara-Lab c5-c7Document10 pagesMicropara-Lab c5-c7Monica JoyceNo ratings yet
- Orchid Virus Diseases in Taiwan and Their Control StrategiesDocument54 pagesOrchid Virus Diseases in Taiwan and Their Control StrategiesPham Lanphuong100% (1)