Download as pdf or txt
You might also like
- Daily ReportDocument3 pagesDaily ReportHussein AbumaisNo ratings yet
- Collective Bargaining, Strikes and The Quest For Industrial Peace in NigeriaDocument23 pagesCollective Bargaining, Strikes and The Quest For Industrial Peace in Nigeriafarad6a0% (1)
- Morth 2100 Open FoundationsDocument6 pagesMorth 2100 Open FoundationsRameshNo ratings yet
- Soc 621 Final PaperDocument16 pagesSoc 621 Final Paperapi-478028340No ratings yet
- Grade 3 Vocabulary Expander Writing Workbook PDFDocument39 pagesGrade 3 Vocabulary Expander Writing Workbook PDFJasmin Manio100% (1)
- Krohne - Stress (26 Mei 2011)Document13 pagesKrohne - Stress (26 Mei 2011)niaambarsari100% (1)
- Health Psych Module-2Document32 pagesHealth Psych Module-2Jahnvi KumarNo ratings yet
- Stress and Coping PDFDocument11 pagesStress and Coping PDFAnnika AcordaNo ratings yet
- Coping and Stress in PsychologyDocument20 pagesCoping and Stress in Psychologyhabiba zulfiqarNo ratings yet
- StressDocument8 pagesStressashrestha2108No ratings yet
- A Discussion and Summary of Acute Stress Response - SiedleckiDocument19 pagesA Discussion and Summary of Acute Stress Response - SiedleckiDr. Varah SiedleckiNo ratings yet
- 5927 22980 1 PBDocument10 pages5927 22980 1 PBAnonymous c3F8HW6IFNo ratings yet
- Stress and HealthDocument66 pagesStress and HealthVasundhara RanaNo ratings yet
- MODULE 10 - 11 Stress, Coping and Immune FunctionDocument16 pagesMODULE 10 - 11 Stress, Coping and Immune Functionartadiel28No ratings yet
- Literature Review Stress ManagementDocument19 pagesLiterature Review Stress ManagementMartin Abiemo50% (4)
- Models - of - Stress - Levine & Scotch 1970Document21 pagesModels - of - Stress - Levine & Scotch 1970MadeleineNo ratings yet
- StressDocument6 pagesStressSrestha GhoshNo ratings yet
- Definition and Evolution of StressDocument1 pageDefinition and Evolution of StressBenita SumitaNo ratings yet
- Stress 1Document36 pagesStress 1Martun XurshudyanNo ratings yet
- Introduction of Stress ManagementDocument7 pagesIntroduction of Stress Managementcoolguru_2050No ratings yet
- Page 3Document2 pagesPage 3Ikechukwu OnuohaNo ratings yet
- Chandanpreet KaurDocument54 pagesChandanpreet KaurHarpreet ThindNo ratings yet
- Examination StressDocument42 pagesExamination StresssofiaislamianNo ratings yet
- 5 PB PDFDocument11 pages5 PB PDFJustikaNo ratings yet
- The Health Effects of StressDocument8 pagesThe Health Effects of Stressapi-291302613No ratings yet
- 04 - Chapter 1Document31 pages04 - Chapter 1MageshNo ratings yet
- Stress: Concepts, Theoretical Models and Nursing InterventionsDocument6 pagesStress: Concepts, Theoretical Models and Nursing Interventionsanna regarNo ratings yet
- 7 Review of Related Literature and StudiesDocument14 pages7 Review of Related Literature and StudiesRon AracoNo ratings yet
- Stress ManagementDocument100 pagesStress ManagementAnjuu Dhar Koul100% (1)
- Stress ManagementDocument122 pagesStress ManagementAnjuu Dhar Koul100% (3)
- Vivekananda College (University of Delhi) : Organizational behaviour-II Practical TOPIC: Organisational Role StressDocument30 pagesVivekananda College (University of Delhi) : Organizational behaviour-II Practical TOPIC: Organisational Role StressSrishti GaurNo ratings yet
- Introduction To Stress TheoryDocument6 pagesIntroduction To Stress TheoryJocelyn PanduyosNo ratings yet
- Stress Models and ApproachesDocument10 pagesStress Models and Approachesgod_26100% (1)
- Atestat Engleza - A Stressful LifeDocument11 pagesAtestat Engleza - A Stressful LifeD3nimNo ratings yet
- Stimulus Oriented ApproachDocument14 pagesStimulus Oriented Approacharyan mukherjeeNo ratings yet
- Academic Paper NotesDocument5 pagesAcademic Paper NotesGracija GaloićNo ratings yet
- StressDocument16 pagesStresssurendragupta8No ratings yet
- Stress PDFDocument7 pagesStress PDFBrett StevensNo ratings yet
- Beh. Sci. 4 - GRP PresentationDocument16 pagesBeh. Sci. 4 - GRP PresentationAnushka NayakNo ratings yet
- Present LatestDocument10 pagesPresent LatestAzwin ZulkufliNo ratings yet
- Stress: Stress Has A Different Meaning For Different People Under DifferentDocument8 pagesStress: Stress Has A Different Meaning For Different People Under DifferentRdiPc ArdyNo ratings yet
- Lesson 16 PDFDocument20 pagesLesson 16 PDFrajamsc2003No ratings yet
- Principles of Psychology PresentationDocument36 pagesPrinciples of Psychology PresentationQueneiceNo ratings yet
- Stress BookletDocument17 pagesStress Bookletraluka120No ratings yet
- Hobfoll ModelDocument12 pagesHobfoll Modeladri90No ratings yet
- Stressors & Reactions Related To Disease Process:: StressDocument14 pagesStressors & Reactions Related To Disease Process:: StressShreyas WalvekarNo ratings yet
- Stress ManagementDocument1 pageStress ManagementAnusha KunduNo ratings yet
- Stress, Coping, and Health: A Conceptual OverviewDocument19 pagesStress, Coping, and Health: A Conceptual OverviewNova ElvaniNo ratings yet
- Stress ManagementDocument16 pagesStress Managementshreyasmohite16No ratings yet
- Stress: Dr. Jayesh PatidarDocument56 pagesStress: Dr. Jayesh PatidarDr. Jayesh Patidar100% (2)
- 04 - Literature ReviewDocument77 pages04 - Literature ReviewVijayaragavan MNo ratings yet
- CrumSaloveyAchor RethinkingStress JPSP2013 PDFDocument18 pagesCrumSaloveyAchor RethinkingStress JPSP2013 PDFAbe AdanNo ratings yet
- Workplace Stress: A Review of The LiteratureDocument34 pagesWorkplace Stress: A Review of The LiteratureRosu MariusNo ratings yet
- Final Research 12 - Nerona and SumaoyDocument57 pagesFinal Research 12 - Nerona and SumaoyJabez CabahugNo ratings yet
- Workplace Stress: A Review of The LiteratureDocument34 pagesWorkplace Stress: A Review of The LiteratureRot MariusNo ratings yet
- Hari Kee Edited ProjectDocument78 pagesHari Kee Edited ProjectVijayaragavan MNo ratings yet
- Erika Louise G. Alison: Heterostasis, Allostasis, Hormesis, and Adaptive Homeostasis. The Term HeterostasisDocument4 pagesErika Louise G. Alison: Heterostasis, Allostasis, Hormesis, and Adaptive Homeostasis. The Term HeterostasisJanice Gentile AlisonNo ratings yet
- Unit 2Document9 pagesUnit 2Sushma LathNo ratings yet
- Physical Stress Theory by Mueller and Maluf (2002)Document2 pagesPhysical Stress Theory by Mueller and Maluf (2002)Maureen Joy Cascayan EspirituNo ratings yet
- Ajpr1 2Document10 pagesAjpr1 2fian christianNo ratings yet
- Project Report On Stress ManagementDocument73 pagesProject Report On Stress ManagementPriya KuttyNo ratings yet
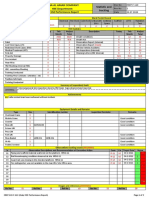
- Welding-Standards 23-03-2014Document1 pageWelding-Standards 23-03-2014givali100% (7)
- Tecnoseal Catalogo Anodos 16Document212 pagesTecnoseal Catalogo Anodos 16JorgeNo ratings yet
- Histology EssayDocument4 pagesHistology EssayalzayyanauroraNo ratings yet
- Unstable Angina PectorisDocument35 pagesUnstable Angina PectorisAkbar IskandarNo ratings yet
- BHI (Brain Heart Infusion) BrothDocument3 pagesBHI (Brain Heart Infusion) BrothHaidar HanifNo ratings yet
- Drone UnfinishedDocument10 pagesDrone UnfinishedLance Kelly ManlangitNo ratings yet
- ACLS Practical Case Scenarios (1 June 2011)Document15 pagesACLS Practical Case Scenarios (1 June 2011)nersNo ratings yet
- DSTC 1586861258Document139 pagesDSTC 1586861258Manjeet Thakur100% (2)
- System of Wheat IntensificationDocument25 pagesSystem of Wheat IntensificationPappu Yadav100% (1)
- 990-736 ABL80 FLEX Service ManualDocument409 pages990-736 ABL80 FLEX Service ManualIsmael MorinigoNo ratings yet
- Administering Oral Medication ScriptDocument4 pagesAdministering Oral Medication ScriptJoanna MontebonNo ratings yet
- Cleanskin K SDS PDFDocument5 pagesCleanskin K SDS PDFIris BetancourtNo ratings yet
- London Food Strategy Implementation 07Document24 pagesLondon Food Strategy Implementation 07Martyn ClarkNo ratings yet
- Female Reproductive SystemDocument8 pagesFemale Reproductive SystemEfanPutraNo ratings yet
- General Chemistry 2Document10 pagesGeneral Chemistry 2Aubrey GuilaranNo ratings yet
- TDS ASP-epoxyCoveDocument2 pagesTDS ASP-epoxyCovetatenda mhuruNo ratings yet
- Pelayanan Kesehatan Peduli Remaja Menurut Perspektif Remaja Di Kota MagelangDocument9 pagesPelayanan Kesehatan Peduli Remaja Menurut Perspektif Remaja Di Kota MagelangArviera KayNo ratings yet
- Programme Fire Sprinkler International 2023 3Document4 pagesProgramme Fire Sprinkler International 2023 3Carlos_MKTRNo ratings yet
- Hoja AnestesiaDocument9 pagesHoja AnestesiaCAMILO ANDRES MANTILLANo ratings yet
- 1 Bengaluru Urban Dist:: Sl. No. Industrial Area Date of Revision (B.M.Date) Prevailing Price/Acre (Rs. in Lakhs) 1 2 3 4Document8 pages1 Bengaluru Urban Dist:: Sl. No. Industrial Area Date of Revision (B.M.Date) Prevailing Price/Acre (Rs. in Lakhs) 1 2 3 4Raju BMNo ratings yet
- Esterification For Butyl Butyrate Formation Using CandidaDocument7 pagesEsterification For Butyl Butyrate Formation Using CandidaDeodata Leela AndiavitriNo ratings yet
- BCE FM Blue+ User Manual - EN 1.2Document48 pagesBCE FM Blue+ User Manual - EN 1.2Zoltan MarosanNo ratings yet
- College Adjustment Scale (CAS)Document7 pagesCollege Adjustment Scale (CAS)Bianca CarmenNo ratings yet
- Lehx9590-02 Emcp II+Document4 pagesLehx9590-02 Emcp II+Jorge Luis Tanaka ConchaNo ratings yet
- Hygroscopic Deliquensce Efflorescence PDFDocument2 pagesHygroscopic Deliquensce Efflorescence PDFJedd MattNo ratings yet