Download as pdf or txt
You might also like
- Bobcat CT335 Compact Tractor Service ManualDocument1,161 pagesBobcat CT335 Compact Tractor Service ManualShawn StevensNo ratings yet
- INTERCHANGE 2 - RQUIZ UNITS 13 & 14 - Revisión Del IntentoDocument5 pagesINTERCHANGE 2 - RQUIZ UNITS 13 & 14 - Revisión Del IntentoAURA ARTEAGA100% (4)
- Test Bank For Neebs Mental Health Nursing 5th by GormanDocument8 pagesTest Bank For Neebs Mental Health Nursing 5th by GormanWilliam Williams100% (34)
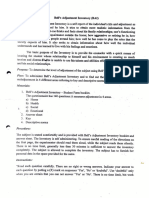
- Bells Adjustment Inventory MaterialsDocument13 pagesBells Adjustment Inventory MaterialsArpitha Rao100% (16)
- EDRA HealthcareTools 2013Document56 pagesEDRA HealthcareTools 2013janeNo ratings yet
- Confined Space PlanDocument16 pagesConfined Space PlanMohd Firdaus Kamaruddin100% (1)
- FIFA 18 - Data Analysis: - Harsh Takrani - Pranay LullaDocument16 pagesFIFA 18 - Data Analysis: - Harsh Takrani - Pranay LullaSovan DashNo ratings yet
- Biometry NoteDocument89 pagesBiometry NotetofakalidNo ratings yet
- Going Beyond Simple Sample Size Calculations: A Practitioner's GuideDocument56 pagesGoing Beyond Simple Sample Size Calculations: A Practitioner's GuideManuel BéjarNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Experiments Reading List With Abstracts - April 6 2020Document63 pagesExperiments Reading List With Abstracts - April 6 2020jshen5No ratings yet
- The Contextual Inquiry: Hanneke Kip Nienke Beerlage-De JongDocument20 pagesThe Contextual Inquiry: Hanneke Kip Nienke Beerlage-De JongamalNo ratings yet
- McConnel, Brendon and Vera-Hernandez (2015)Document53 pagesMcConnel, Brendon and Vera-Hernandez (2015)María Ignacia Valenzuela NavarroNo ratings yet
- Effect Size Estimates: Current Use, Calculations, and InterpretationDocument19 pagesEffect Size Estimates: Current Use, Calculations, and InterpretationsofianiddaNo ratings yet
- Lakens2013-Calculating and Reporting Effect Sizes To Facilitate Cumulative Science PDFDocument12 pagesLakens2013-Calculating and Reporting Effect Sizes To Facilitate Cumulative Science PDFDanielNo ratings yet
- 1 s2.0 S014829631500630X Main 2 PDFDocument9 pages1 s2.0 S014829631500630X Main 2 PDFAltair CamargoNo ratings yet
- Assumptions of The Study Thesis ExampleDocument8 pagesAssumptions of The Study Thesis ExampleCourtney Esco100% (2)
- 10 Experimental Learning GuideDocument5 pages10 Experimental Learning GuideDewa PutraNo ratings yet
- Power To The People ManuscriptDocument42 pagesPower To The People ManuscriptZerlinda SanamNo ratings yet
- 2010 November 01 Agung Santoso With Cover Page v2Document18 pages2010 November 01 Agung Santoso With Cover Page v2muhammad ismailNo ratings yet
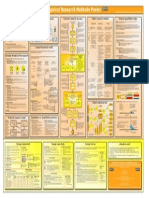
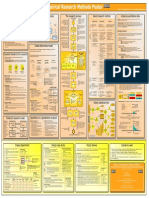
- ResearchMethods Poster A4 en Ver 1.0Document1 pageResearchMethods Poster A4 en Ver 1.0Gitarja SandiNo ratings yet
- Review of LiteratureDocument10 pagesReview of LiteraturePrasanth KumarNo ratings yet
- Statistical Significance Versus Clinical ImportanceDocument5 pagesStatistical Significance Versus Clinical ImportanceKaren Sanchez AcostaNo ratings yet
- Andrew Gelman - The Problem With P-Values - AddendumDocument3 pagesAndrew Gelman - The Problem With P-Values - AddendumLoki OdinsonNo ratings yet
- Aim Research PaperDocument7 pagesAim Research Paperqwgqavvhf100% (1)
- U02d1 Scientific Merit and Internal ValidityDocument4 pagesU02d1 Scientific Merit and Internal Validityarhodes777No ratings yet
- Research Paper Null HypothesisDocument7 pagesResearch Paper Null Hypothesisshvximwhf100% (1)
- Kelley y Preacher, 2012Document16 pagesKelley y Preacher, 2012DiegoNo ratings yet
- Experimental Design and Statistics in Speech Science - The Handbook of Phonetic Sciences - Blackwell Reference OnlineDocument14 pagesExperimental Design and Statistics in Speech Science - The Handbook of Phonetic Sciences - Blackwell Reference OnlineHAKAN ÖZTEMÜRNo ratings yet
- Solution IMT-120 3Document8 pagesSolution IMT-120 3Kishor kumar BhatiaNo ratings yet
- Stating Null Hypothesis in Research PaperDocument7 pagesStating Null Hypothesis in Research Paperalrasexlie1986100% (2)
- Core Processes Preprint-2018-10-01t09 31 40.904ZDocument36 pagesCore Processes Preprint-2018-10-01t09 31 40.904Zwaleed hussainNo ratings yet
- The Research Prospectus Is A Brief Overview of The Key Components of A Research StudyDocument6 pagesThe Research Prospectus Is A Brief Overview of The Key Components of A Research StudyLucciana BolañosNo ratings yet
- Meta AnalysisofPrevalenceStudiesusingR August2021Document6 pagesMeta AnalysisofPrevalenceStudiesusingR August2021Juris JustinNo ratings yet
- Scope: How Much Should A Good Theory Account For?: ActknowledgeDocument5 pagesScope: How Much Should A Good Theory Account For?: ActknowledgexasteNo ratings yet
- Emperical Research Methods PosterDocument1 pageEmperical Research Methods PosterДмитрий ТокаренкоNo ratings yet
- Estadistica #4Document3 pagesEstadistica #4azael garciaNo ratings yet
- Dissertation MSCDocument8 pagesDissertation MSCWhatShouldIWriteMyPaperOnCincinnati100% (1)
- Imd121 Assignment 1Document5 pagesImd121 Assignment 1NUR IZZAH ISKANDARNo ratings yet
- 3150 2010 November 01 Agung Santoso-with-cover-page-V2Document18 pages3150 2010 November 01 Agung Santoso-with-cover-page-V2fauzi djNo ratings yet
- Limitations Systematic Literature ReviewDocument5 pagesLimitations Systematic Literature Reviewc5rqq644100% (1)
- Propensity Scores: A Practical Introduction Using RDocument21 pagesPropensity Scores: A Practical Introduction Using RMunirul UlaNo ratings yet
- Methods in Business ResearchDocument66 pagesMethods in Business ResearchosamaNo ratings yet
- Mathematics 11 01982Document10 pagesMathematics 11 01982eder rodriguesNo ratings yet
- Case Study Research in Counselling and PsychotherapyDocument24 pagesCase Study Research in Counselling and PsychotherapyRyan BlakeNo ratings yet
- Scale Development ThesisDocument7 pagesScale Development Thesiskarennelsoncolumbia100% (2)
- List of Research Papers in StatisticsDocument8 pagesList of Research Papers in Statisticsgpnovecnd100% (1)
- Mental Health Services Research Methodology 2002Document8 pagesMental Health Services Research Methodology 2002Kats CoelloNo ratings yet
- Literature Review of Operational ResearchDocument8 pagesLiterature Review of Operational Researchc5dg36am100% (1)
- Designing A Research Project: Randomised Controlled Trials and Their Principles J M KendallDocument21 pagesDesigning A Research Project: Randomised Controlled Trials and Their Principles J M KendallNefta BaptisteNo ratings yet
- Research SeriesDocument21 pagesResearch SeriesNefta BaptisteNo ratings yet
- PR2 - SLHT 1 - January 4 To 8Document5 pagesPR2 - SLHT 1 - January 4 To 8JESSA SUMAYANGNo ratings yet
- Kang (2021)Document12 pagesKang (2021)Syara Shazanna ZulkifliNo ratings yet
- Social Science Dissertation Methodology SampleDocument5 pagesSocial Science Dissertation Methodology SamplePaySomeoneToWriteYourPaperSpringfield100% (1)
- Literature Review On Behaviour ModificationDocument8 pagesLiterature Review On Behaviour Modificationc5sx83ws100% (1)
- Business Plan HypothesisDocument8 pagesBusiness Plan Hypothesisafcnzfamt100% (2)
- To Adjust or Not Adjust Nonparametric Effect Sizes, Confidence Intervals, and Real-World Meaning PDFDocument7 pagesTo Adjust or Not Adjust Nonparametric Effect Sizes, Confidence Intervals, and Real-World Meaning PDFTodd MartinezNo ratings yet
- Believe It or Not - How Much Can We Rely On Published Data On Potential Drug Targets - Nature Reviews Drug DiscoveryDocument14 pagesBelieve It or Not - How Much Can We Rely On Published Data On Potential Drug Targets - Nature Reviews Drug DiscoverycipinaNo ratings yet
- Artikel 2 Greenwald, Within Subjects Designs To Use or Not To UseDocument7 pagesArtikel 2 Greenwald, Within Subjects Designs To Use or Not To UseBilqis HumairaNo ratings yet
- Descriptive Statistics Thesis PDFDocument6 pagesDescriptive Statistics Thesis PDFtsivhqvcf100% (2)
- Studi Deskriptif Effect Size PenelitianDocument17 pagesStudi Deskriptif Effect Size PenelitianRatiih YuniiartyNo ratings yet
- Sharma 2021 CBT Asd Anxiety SRDocument16 pagesSharma 2021 CBT Asd Anxiety SRIoanna SachaNo ratings yet
- Clinical Prediction Models: A Practical Approach to Development, Validation, and UpdatingFrom EverandClinical Prediction Models: A Practical Approach to Development, Validation, and UpdatingNo ratings yet
- Effect SizeDocument17 pagesEffect SizeandriyoethNo ratings yet
- Effect Sizes Based On MeansDocument2 pagesEffect Sizes Based On MeansMundNo ratings yet
- Biostatistics Explored Through R Software: An OverviewFrom EverandBiostatistics Explored Through R Software: An OverviewRating: 3.5 out of 5 stars3.5/5 (2)
- Certificate of ComplianceDocument7 pagesCertificate of ComplianceCaner KURTNo ratings yet
- 139-1 L12R-L16R 0503 GB PDFDocument67 pages139-1 L12R-L16R 0503 GB PDFDanielNo ratings yet
- User Manual - 5'' Round (Hotplate) Magnetic Stirrer PDFDocument19 pagesUser Manual - 5'' Round (Hotplate) Magnetic Stirrer PDFMaxele ChavezNo ratings yet
- 7SR242 - Duobias Technical Manual Chapter 02 Settings, Configuration and InstrumentsDocument20 pages7SR242 - Duobias Technical Manual Chapter 02 Settings, Configuration and InstrumentsssNo ratings yet
- Moisture Suppressant For Electrical FittingsDocument2 pagesMoisture Suppressant For Electrical FittingsFraz AhmadNo ratings yet
- Fireworks and Dream Weaver CS3 Under UbuntuDocument2 pagesFireworks and Dream Weaver CS3 Under UbuntuMucahit YilmazNo ratings yet
- T070800480-A5tmn-001 FS 1.0Document26 pagesT070800480-A5tmn-001 FS 1.0megatornadoNo ratings yet
- HL109201 Strobe - 29 Candela, Hazardous Location DatasheetDocument2 pagesHL109201 Strobe - 29 Candela, Hazardous Location Datasheetjose medinaNo ratings yet
- Microwave and Millimeter Wave Power BeamingDocument31 pagesMicrowave and Millimeter Wave Power BeamingMonkeyFromMarsNo ratings yet
- Individual Inventory FormDocument1 pageIndividual Inventory FormNorhana LumambasNo ratings yet
- Fruit ArmaDocument4 pagesFruit ArmaDana CanfieldNo ratings yet
- E Governance UPSC NotesDocument5 pagesE Governance UPSC NotesranbirkhanNo ratings yet
- Instruction Manual Transformer Oil BDV Tester IIJ-II-80KVDocument10 pagesInstruction Manual Transformer Oil BDV Tester IIJ-II-80KVCLAUDE BIRIKUNZIRANo ratings yet
- IENA 2020 Annales Concours AnglaisDocument82 pagesIENA 2020 Annales Concours AnglaisMarie MorganNo ratings yet
- Nabhasa Yogas Nabhasa Yogas Nabhasa Yogas Nabhasa Yogas: Sara "Arrow" Yoga: All Planets in All 4 Houses Commencing FromDocument1 pageNabhasa Yogas Nabhasa Yogas Nabhasa Yogas Nabhasa Yogas: Sara "Arrow" Yoga: All Planets in All 4 Houses Commencing FromNeoHoodaNo ratings yet
- 'Burrmalala': Indigenous Cyclone Knowledge Shared in Arnhem Land Film - ABC NewsDocument2 pages'Burrmalala': Indigenous Cyclone Knowledge Shared in Arnhem Land Film - ABC NewsRQL83appNo ratings yet
- DF AntennaDocument5 pagesDF Antennajose eliasNo ratings yet
- 203 Artifact 2 Field ObservationDocument6 pages203 Artifact 2 Field Observationapi-582885919No ratings yet
- Reyes Tag Ppt-PrefinalsDocument11 pagesReyes Tag Ppt-PrefinalsRaphaella Mae Alegre ReyesNo ratings yet
- WELD-Electrical Characteristics of An Arc (With Diagram) - MetallurgyDocument4 pagesWELD-Electrical Characteristics of An Arc (With Diagram) - MetallurgypeterNo ratings yet
- Mishkin Economics of Money 9th Edition PDFDocument8 pagesMishkin Economics of Money 9th Edition PDFSalman Farizi25% (4)
- Tagore and NationalismDocument6 pagesTagore and NationalismTanya ChopraNo ratings yet
- Recruitment - Dalda: Human Resource ManagementDocument13 pagesRecruitment - Dalda: Human Resource ManagementMubaraka QuaidNo ratings yet
- E Commerce Business PlanDocument4 pagesE Commerce Business Planpraveenzte50% (2)