
Respect FocusedTherapy CH 1
Respect FocusedTherapy CH 1
You might also like
- Totton Power in The Therapy RoomDocument4 pagesTotton Power in The Therapy RoomMorana Bi100% (1)
- The Healing Codes - Heart Issues FinderDocument10 pagesThe Healing Codes - Heart Issues FinderVladianu Dan100% (1)
- Invitations To Responsibility 1 PDFDocument55 pagesInvitations To Responsibility 1 PDFerikaNo ratings yet
- Elliott Eisner Ex Imp NullDocument1 pageElliott Eisner Ex Imp Nullapi-227888640100% (1)
- Managing Use of Self For Masterful Professional PracticeDocument8 pagesManaging Use of Self For Masterful Professional PracticeIshhikaa ShhukllNo ratings yet
- Impaired Social InteractionDocument4 pagesImpaired Social InteractionAaron ConstantinoNo ratings yet
- Adobe Scan 26-Jul-2023Document10 pagesAdobe Scan 26-Jul-202311B14 Lalrinfeli FanaiNo ratings yet
- Assignment 3 EthicsDocument2 pagesAssignment 3 EthicsDhawal GuptaNo ratings yet
- Dejesus06 ELMS Activity 2 (Essay) - ARGDocument3 pagesDejesus06 ELMS Activity 2 (Essay) - ARGAJ DejesusNo ratings yet
- My Struggle StoryDocument1 pageMy Struggle StoryStephannie AlobNo ratings yet
- Pesigan, BEED3A Engaging&PerformanceTasks MODULE3Document3 pagesPesigan, BEED3A Engaging&PerformanceTasks MODULE3Jezel Joy PesiganNo ratings yet
- Functions of Communication Functions of Communication Nature and Scope Examples/SituationsDocument2 pagesFunctions of Communication Functions of Communication Nature and Scope Examples/SituationsEric LacsiteNo ratings yet
- Communication-The Human Connection-Is The Key To Personal and Career Success.' (Paul J. Meyer)Document6 pagesCommunication-The Human Connection-Is The Key To Personal and Career Success.' (Paul J. Meyer)johnmaximo100% (1)
- Jrma/37 1 117Document14 pagesJrma/37 1 117andrei dradiciNo ratings yet
- Chapter 4Document11 pagesChapter 4Yellow BoxNo ratings yet
- BSBLDR511 Question Answer 2nd FileDocument25 pagesBSBLDR511 Question Answer 2nd Filekavita adhikariNo ratings yet
- Mindfulness and Yoga For Self-Regulation A Primer ... - (Part II The Mindful Self)Document5 pagesMindfulness and Yoga For Self-Regulation A Primer ... - (Part II The Mindful Self)Mayra Alejandra Sanchez Pati�ONo ratings yet
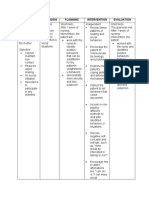
- Assessment Diagnosis Planning Intervention EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention EvaluationSTA INES, ELIJAH DOMINIQUENo ratings yet
- Davis 1987Document14 pagesDavis 1987dingin BerlarutNo ratings yet
- Activity 3 - Moral Recovery ProgramDocument5 pagesActivity 3 - Moral Recovery ProgramYna ForondaNo ratings yet
- Artículo Sobre Liderazgo en PecesDocument8 pagesArtículo Sobre Liderazgo en PecesLucía MaldonadoNo ratings yet
- 7 C'S' and 4 S'S: 10 11.234 © Copy Right: Rai UniversityDocument2 pages7 C'S' and 4 S'S: 10 11.234 © Copy Right: Rai UniversityNicoleNo ratings yet
- ChineseDocument2 pagesChinesejibranredroseNo ratings yet
- 5 CONTENT 6 - Lesson 2 (M)Document8 pages5 CONTENT 6 - Lesson 2 (M)Angel RodriguezNo ratings yet
- AttitudeDocument15 pagesAttitudeAntas KumarNo ratings yet
- Personal Development M5 - CathyDocument3 pagesPersonal Development M5 - CathyCatherine PanoyNo ratings yet
- Adobe Scan 09 Oct 2022Document2 pagesAdobe Scan 09 Oct 2022Minakshi KalraNo ratings yet
- Personality Development 2 ReviewerDocument3 pagesPersonality Development 2 Reviewerralphsimons32No ratings yet
- Textual Summary Lesson 7 12Document6 pagesTextual Summary Lesson 7 12Mai RuizNo ratings yet
- Journal 3 Weeks 5 6 and 7Document3 pagesJournal 3 Weeks 5 6 and 7api-510613864No ratings yet
- Breaches in The Therapeutic Alliance: An Arena For Negotiating Authentic RelatednessDocument14 pagesBreaches in The Therapeutic Alliance: An Arena For Negotiating Authentic RelatednessJorge Rojas GNo ratings yet
- Literature Review Conclusion: Laura TeepleDocument1 pageLiterature Review Conclusion: Laura TeepleLaura TeepleNo ratings yet
- TCSPP Poster Valor PDFDocument1 pageTCSPP Poster Valor PDFLaura TeepleNo ratings yet
- Relationship Boundary Mapping v3Document2 pagesRelationship Boundary Mapping v3KarenGimenezNo ratings yet
- NCM117 Theory Midterm Exam Reviewer PDFDocument31 pagesNCM117 Theory Midterm Exam Reviewer PDFJesil MaroliñaNo ratings yet
- Teaching-Guide-Catchup-FILIPINO Grade 9Document7 pagesTeaching-Guide-Catchup-FILIPINO Grade 9Mhaylene Baria GonzalesNo ratings yet
- Interpersonal Theory PresentationDocument15 pagesInterpersonal Theory PresentationBeche May LumantasNo ratings yet
- Organizational CultureDocument4 pagesOrganizational CultureMoses NielsenNo ratings yet
- Intervencion en Familia Aporte Individual Prueba NacionalDocument5 pagesIntervencion en Familia Aporte Individual Prueba NacionalVictoriaCadenaNo ratings yet
- The Code of Professional ResponsibilityDocument2 pagesThe Code of Professional Responsibilityapi-434048982No ratings yet
- Ethics Lesson 4Document9 pagesEthics Lesson 4Vanessa Ambroce100% (1)
- RitualsDocument35 pagesRitualsAmala Oliveira100% (6)
- Career Portfolio - Bacus Merianne Yvon NicoleiDocument9 pagesCareer Portfolio - Bacus Merianne Yvon Nicoleirose ynqueNo ratings yet
- Intersubjectivity Q2 Week3Document16 pagesIntersubjectivity Q2 Week3Randz TakiawanNo ratings yet
- Module 3 Ethics in Communication 1Document13 pagesModule 3 Ethics in Communication 1Raffy Alovera ArceoNo ratings yet
- Module 1 PDFDocument8 pagesModule 1 PDFVilla Rose Zabala Raposas100% (2)
- Soe Dispositions Rubric-3Document6 pagesSoe Dispositions Rubric-3api-710835909No ratings yet
- Moral Psychology Is Relationship Regulation: Moral Motives For Unity, Hierarchy, Equality, and ProportionalityDocument19 pagesMoral Psychology Is Relationship Regulation: Moral Motives For Unity, Hierarchy, Equality, and ProportionalityWilliam German Benjamin Florez MorenoNo ratings yet
- CA 3 Notes On TCMPDocument49 pagesCA 3 Notes On TCMPnathaniel.domingoNo ratings yet
- Easy Social Psychology Concepts: Aggression Bystander EffectDocument6 pagesEasy Social Psychology Concepts: Aggression Bystander EffectSindhulakshmi BabuNo ratings yet
- PSPE Interaction SSDocument2 pagesPSPE Interaction SSmalissa nugeraNo ratings yet
- Interpersonnal CommunicationDocument14 pagesInterpersonnal CommunicationJavier BenitezNo ratings yet
- 2d A Review of Nonverbal Behaviors of Women and MenDocument14 pages2d A Review of Nonverbal Behaviors of Women and MenVision 12No ratings yet
- Personal Development WHLPDocument4 pagesPersonal Development WHLPNicole ResareNo ratings yet
- Situation Reasons Effect Reaction AdviceDocument11 pagesSituation Reasons Effect Reaction AdviceMariel Samonte VillanuevaNo ratings yet
- 1 - Leavitt Sluss 2015Document25 pages1 - Leavitt Sluss 2015jsteixeiraNo ratings yet
- Love and Intimacy, Psychology Of: Panos Kordoutis, Panteion University of Social and Political Sciences, Athens, GreeceDocument7 pagesLove and Intimacy, Psychology Of: Panos Kordoutis, Panteion University of Social and Political Sciences, Athens, Greeceachmad fatoniNo ratings yet
- Hofstede'S Six Dimensions of Culture: PDI Characteristics TipsDocument8 pagesHofstede'S Six Dimensions of Culture: PDI Characteristics TipsJemilyn Cervantes-SegundoNo ratings yet
- Unit 3 Social LiteracyDocument3 pagesUnit 3 Social LiteracyPherlyn CuadraNo ratings yet
- Managing Use of SelfDocument8 pagesManaging Use of SelfAnnamariaNo ratings yet
- Empath vs Narcissist in Workplace: A Roadmap to Understand and stop the Cycle of Narcissistic Abuse, Co-dependency, Manipulation, Build Self Confidence and Thrive in Your WorkplaceFrom EverandEmpath vs Narcissist in Workplace: A Roadmap to Understand and stop the Cycle of Narcissistic Abuse, Co-dependency, Manipulation, Build Self Confidence and Thrive in Your WorkplaceNo ratings yet
- The Introverts Dilemma: Misunderstood and UniqueFrom EverandThe Introverts Dilemma: Misunderstood and UniqueRating: 4 out of 5 stars4/5 (1)
- Research Proposal - Group 10Document14 pagesResearch Proposal - Group 10Ngọc Diễm PhùngNo ratings yet
- Lesson1 Moral and Non-Moral StandardsDocument25 pagesLesson1 Moral and Non-Moral StandardsManongdo Allan0% (1)
- Part 2: Emotional Intelligence: Spring 2018 Ofa Fellows LeadersDocument53 pagesPart 2: Emotional Intelligence: Spring 2018 Ofa Fellows LeadersSafariNo ratings yet
- Seminar On Demonstration ChitraDocument10 pagesSeminar On Demonstration ChitraShaells Joshi100% (1)
- Agnes MoorsDocument10 pagesAgnes MoorsAndra ToldeanNo ratings yet
- Play Advocacy AssignmentDocument22 pagesPlay Advocacy Assignmentapi-639912537No ratings yet
- Mental Health Status of The BPed in Relation To Academic PerformanceDocument62 pagesMental Health Status of The BPed in Relation To Academic PerformanceMira, RenzoNo ratings yet
- Final - There Is Not Only YouDocument1 pageFinal - There Is Not Only YouAhlea MuscaNo ratings yet
- Keys For Change - Myles Munroe PDFDocument46 pagesKeys For Change - Myles Munroe PDFAndressi Label100% (2)
- Subjects and Their Career LinksDocument22 pagesSubjects and Their Career LinksShivam SinghNo ratings yet
- Foreign Policy AnalysisDocument5 pagesForeign Policy AnalysisHaseeb UllahNo ratings yet
- DISSDocument3 pagesDISSprechi decipoloNo ratings yet
- MODULE 7 - Week 3 - The Child and Adolescent Learners and Learning PrinciplesDocument10 pagesMODULE 7 - Week 3 - The Child and Adolescent Learners and Learning PrinciplesMarsha MGNo ratings yet
- Florence Nightingale'S Environmental Theory: Cortez, C. Madriaga, J. Quitevis, R. Reyes, A. Salamat, NDocument9 pagesFlorence Nightingale'S Environmental Theory: Cortez, C. Madriaga, J. Quitevis, R. Reyes, A. Salamat, NchrizthineeNo ratings yet
- Koretz, Daniel. Measuring UpDocument4 pagesKoretz, Daniel. Measuring UprafadrimarquesNo ratings yet
- Mam Tan Ass.Document3 pagesMam Tan Ass.KimberlyRicamaraNo ratings yet
- 3.moral Non Moral StandardDocument16 pages3.moral Non Moral StandardDaisy Daguplo BautistaNo ratings yet
- Introduction To SMART Objectives and SMART GoalsDocument9 pagesIntroduction To SMART Objectives and SMART GoalsRandy ManaloNo ratings yet
- Are Adolescents Less Mature Than Adults?Document12 pagesAre Adolescents Less Mature Than Adults?Regina OrdoñaNo ratings yet
- Relationship Between Salary and Job SatisfactionDocument28 pagesRelationship Between Salary and Job SatisfactionUyen Tran0% (1)
- HLTB50 Close Reading AssignmentDocument4 pagesHLTB50 Close Reading Assignmentnavafaria03No ratings yet
- HRD Audit Instruments QuestionnaireDocument27 pagesHRD Audit Instruments QuestionnaireSneha Chavan100% (2)
- PE/Health Course OutlineDocument4 pagesPE/Health Course Outlineapi-17070066No ratings yet
- A Review On Peer Correction: Writing 5Document4 pagesA Review On Peer Correction: Writing 5dphvuNo ratings yet
- COM 20041 Address Complex ChallengesDocument12 pagesCOM 20041 Address Complex ChallengesBrian WereNo ratings yet
- KVE401Document10 pagesKVE401sunny SINGHNo ratings yet
- The Science of Making Learning Stick AGES Model PDFDocument19 pagesThe Science of Making Learning Stick AGES Model PDFGilberto GarciaNo ratings yet
- Qualities of A Good Teacher and Techniques in Teaching Maryam BaigDocument7 pagesQualities of A Good Teacher and Techniques in Teaching Maryam Baigapi-310691943No ratings yet





















































































Download as pdf or txt
You might also like
- Totton Power in The Therapy RoomDocument4 pagesTotton Power in The Therapy RoomMorana Bi100% (1)
- The Healing Codes - Heart Issues FinderDocument10 pagesThe Healing Codes - Heart Issues FinderVladianu Dan100% (1)
- Invitations To Responsibility 1 PDFDocument55 pagesInvitations To Responsibility 1 PDFerikaNo ratings yet
- Elliott Eisner Ex Imp NullDocument1 pageElliott Eisner Ex Imp Nullapi-227888640100% (1)
- Managing Use of Self For Masterful Professional PracticeDocument8 pagesManaging Use of Self For Masterful Professional PracticeIshhikaa ShhukllNo ratings yet
- Impaired Social InteractionDocument4 pagesImpaired Social InteractionAaron ConstantinoNo ratings yet
- Adobe Scan 26-Jul-2023Document10 pagesAdobe Scan 26-Jul-202311B14 Lalrinfeli FanaiNo ratings yet
- Assignment 3 EthicsDocument2 pagesAssignment 3 EthicsDhawal GuptaNo ratings yet
- Dejesus06 ELMS Activity 2 (Essay) - ARGDocument3 pagesDejesus06 ELMS Activity 2 (Essay) - ARGAJ DejesusNo ratings yet
- My Struggle StoryDocument1 pageMy Struggle StoryStephannie AlobNo ratings yet
- Pesigan, BEED3A Engaging&PerformanceTasks MODULE3Document3 pagesPesigan, BEED3A Engaging&PerformanceTasks MODULE3Jezel Joy PesiganNo ratings yet
- Functions of Communication Functions of Communication Nature and Scope Examples/SituationsDocument2 pagesFunctions of Communication Functions of Communication Nature and Scope Examples/SituationsEric LacsiteNo ratings yet
- Communication-The Human Connection-Is The Key To Personal and Career Success.' (Paul J. Meyer)Document6 pagesCommunication-The Human Connection-Is The Key To Personal and Career Success.' (Paul J. Meyer)johnmaximo100% (1)
- Jrma/37 1 117Document14 pagesJrma/37 1 117andrei dradiciNo ratings yet
- Chapter 4Document11 pagesChapter 4Yellow BoxNo ratings yet
- BSBLDR511 Question Answer 2nd FileDocument25 pagesBSBLDR511 Question Answer 2nd Filekavita adhikariNo ratings yet
- Mindfulness and Yoga For Self-Regulation A Primer ... - (Part II The Mindful Self)Document5 pagesMindfulness and Yoga For Self-Regulation A Primer ... - (Part II The Mindful Self)Mayra Alejandra Sanchez Pati�ONo ratings yet
- Assessment Diagnosis Planning Intervention EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention EvaluationSTA INES, ELIJAH DOMINIQUENo ratings yet
- Davis 1987Document14 pagesDavis 1987dingin BerlarutNo ratings yet
- Activity 3 - Moral Recovery ProgramDocument5 pagesActivity 3 - Moral Recovery ProgramYna ForondaNo ratings yet
- Artículo Sobre Liderazgo en PecesDocument8 pagesArtículo Sobre Liderazgo en PecesLucía MaldonadoNo ratings yet
- 7 C'S' and 4 S'S: 10 11.234 © Copy Right: Rai UniversityDocument2 pages7 C'S' and 4 S'S: 10 11.234 © Copy Right: Rai UniversityNicoleNo ratings yet
- ChineseDocument2 pagesChinesejibranredroseNo ratings yet
- 5 CONTENT 6 - Lesson 2 (M)Document8 pages5 CONTENT 6 - Lesson 2 (M)Angel RodriguezNo ratings yet
- AttitudeDocument15 pagesAttitudeAntas KumarNo ratings yet
- Personal Development M5 - CathyDocument3 pagesPersonal Development M5 - CathyCatherine PanoyNo ratings yet
- Adobe Scan 09 Oct 2022Document2 pagesAdobe Scan 09 Oct 2022Minakshi KalraNo ratings yet
- Personality Development 2 ReviewerDocument3 pagesPersonality Development 2 Reviewerralphsimons32No ratings yet
- Textual Summary Lesson 7 12Document6 pagesTextual Summary Lesson 7 12Mai RuizNo ratings yet
- Journal 3 Weeks 5 6 and 7Document3 pagesJournal 3 Weeks 5 6 and 7api-510613864No ratings yet
- Breaches in The Therapeutic Alliance: An Arena For Negotiating Authentic RelatednessDocument14 pagesBreaches in The Therapeutic Alliance: An Arena For Negotiating Authentic RelatednessJorge Rojas GNo ratings yet
- Literature Review Conclusion: Laura TeepleDocument1 pageLiterature Review Conclusion: Laura TeepleLaura TeepleNo ratings yet
- TCSPP Poster Valor PDFDocument1 pageTCSPP Poster Valor PDFLaura TeepleNo ratings yet
- Relationship Boundary Mapping v3Document2 pagesRelationship Boundary Mapping v3KarenGimenezNo ratings yet
- NCM117 Theory Midterm Exam Reviewer PDFDocument31 pagesNCM117 Theory Midterm Exam Reviewer PDFJesil MaroliñaNo ratings yet
- Teaching-Guide-Catchup-FILIPINO Grade 9Document7 pagesTeaching-Guide-Catchup-FILIPINO Grade 9Mhaylene Baria GonzalesNo ratings yet
- Interpersonal Theory PresentationDocument15 pagesInterpersonal Theory PresentationBeche May LumantasNo ratings yet
- Organizational CultureDocument4 pagesOrganizational CultureMoses NielsenNo ratings yet
- Intervencion en Familia Aporte Individual Prueba NacionalDocument5 pagesIntervencion en Familia Aporte Individual Prueba NacionalVictoriaCadenaNo ratings yet
- The Code of Professional ResponsibilityDocument2 pagesThe Code of Professional Responsibilityapi-434048982No ratings yet
- Ethics Lesson 4Document9 pagesEthics Lesson 4Vanessa Ambroce100% (1)
- RitualsDocument35 pagesRitualsAmala Oliveira100% (6)
- Career Portfolio - Bacus Merianne Yvon NicoleiDocument9 pagesCareer Portfolio - Bacus Merianne Yvon Nicoleirose ynqueNo ratings yet
- Intersubjectivity Q2 Week3Document16 pagesIntersubjectivity Q2 Week3Randz TakiawanNo ratings yet
- Module 3 Ethics in Communication 1Document13 pagesModule 3 Ethics in Communication 1Raffy Alovera ArceoNo ratings yet
- Module 1 PDFDocument8 pagesModule 1 PDFVilla Rose Zabala Raposas100% (2)
- Soe Dispositions Rubric-3Document6 pagesSoe Dispositions Rubric-3api-710835909No ratings yet
- Moral Psychology Is Relationship Regulation: Moral Motives For Unity, Hierarchy, Equality, and ProportionalityDocument19 pagesMoral Psychology Is Relationship Regulation: Moral Motives For Unity, Hierarchy, Equality, and ProportionalityWilliam German Benjamin Florez MorenoNo ratings yet
- CA 3 Notes On TCMPDocument49 pagesCA 3 Notes On TCMPnathaniel.domingoNo ratings yet
- Easy Social Psychology Concepts: Aggression Bystander EffectDocument6 pagesEasy Social Psychology Concepts: Aggression Bystander EffectSindhulakshmi BabuNo ratings yet
- PSPE Interaction SSDocument2 pagesPSPE Interaction SSmalissa nugeraNo ratings yet
- Interpersonnal CommunicationDocument14 pagesInterpersonnal CommunicationJavier BenitezNo ratings yet
- 2d A Review of Nonverbal Behaviors of Women and MenDocument14 pages2d A Review of Nonverbal Behaviors of Women and MenVision 12No ratings yet
- Personal Development WHLPDocument4 pagesPersonal Development WHLPNicole ResareNo ratings yet
- Situation Reasons Effect Reaction AdviceDocument11 pagesSituation Reasons Effect Reaction AdviceMariel Samonte VillanuevaNo ratings yet
- 1 - Leavitt Sluss 2015Document25 pages1 - Leavitt Sluss 2015jsteixeiraNo ratings yet
- Love and Intimacy, Psychology Of: Panos Kordoutis, Panteion University of Social and Political Sciences, Athens, GreeceDocument7 pagesLove and Intimacy, Psychology Of: Panos Kordoutis, Panteion University of Social and Political Sciences, Athens, Greeceachmad fatoniNo ratings yet
- Hofstede'S Six Dimensions of Culture: PDI Characteristics TipsDocument8 pagesHofstede'S Six Dimensions of Culture: PDI Characteristics TipsJemilyn Cervantes-SegundoNo ratings yet
- Unit 3 Social LiteracyDocument3 pagesUnit 3 Social LiteracyPherlyn CuadraNo ratings yet
- Managing Use of SelfDocument8 pagesManaging Use of SelfAnnamariaNo ratings yet
- Empath vs Narcissist in Workplace: A Roadmap to Understand and stop the Cycle of Narcissistic Abuse, Co-dependency, Manipulation, Build Self Confidence and Thrive in Your WorkplaceFrom EverandEmpath vs Narcissist in Workplace: A Roadmap to Understand and stop the Cycle of Narcissistic Abuse, Co-dependency, Manipulation, Build Self Confidence and Thrive in Your WorkplaceNo ratings yet
- The Introverts Dilemma: Misunderstood and UniqueFrom EverandThe Introverts Dilemma: Misunderstood and UniqueRating: 4 out of 5 stars4/5 (1)
- Research Proposal - Group 10Document14 pagesResearch Proposal - Group 10Ngọc Diễm PhùngNo ratings yet
- Lesson1 Moral and Non-Moral StandardsDocument25 pagesLesson1 Moral and Non-Moral StandardsManongdo Allan0% (1)
- Part 2: Emotional Intelligence: Spring 2018 Ofa Fellows LeadersDocument53 pagesPart 2: Emotional Intelligence: Spring 2018 Ofa Fellows LeadersSafariNo ratings yet
- Seminar On Demonstration ChitraDocument10 pagesSeminar On Demonstration ChitraShaells Joshi100% (1)
- Agnes MoorsDocument10 pagesAgnes MoorsAndra ToldeanNo ratings yet
- Play Advocacy AssignmentDocument22 pagesPlay Advocacy Assignmentapi-639912537No ratings yet
- Mental Health Status of The BPed in Relation To Academic PerformanceDocument62 pagesMental Health Status of The BPed in Relation To Academic PerformanceMira, RenzoNo ratings yet
- Final - There Is Not Only YouDocument1 pageFinal - There Is Not Only YouAhlea MuscaNo ratings yet
- Keys For Change - Myles Munroe PDFDocument46 pagesKeys For Change - Myles Munroe PDFAndressi Label100% (2)
- Subjects and Their Career LinksDocument22 pagesSubjects and Their Career LinksShivam SinghNo ratings yet
- Foreign Policy AnalysisDocument5 pagesForeign Policy AnalysisHaseeb UllahNo ratings yet
- DISSDocument3 pagesDISSprechi decipoloNo ratings yet
- MODULE 7 - Week 3 - The Child and Adolescent Learners and Learning PrinciplesDocument10 pagesMODULE 7 - Week 3 - The Child and Adolescent Learners and Learning PrinciplesMarsha MGNo ratings yet
- Florence Nightingale'S Environmental Theory: Cortez, C. Madriaga, J. Quitevis, R. Reyes, A. Salamat, NDocument9 pagesFlorence Nightingale'S Environmental Theory: Cortez, C. Madriaga, J. Quitevis, R. Reyes, A. Salamat, NchrizthineeNo ratings yet
- Koretz, Daniel. Measuring UpDocument4 pagesKoretz, Daniel. Measuring UprafadrimarquesNo ratings yet
- Mam Tan Ass.Document3 pagesMam Tan Ass.KimberlyRicamaraNo ratings yet
- 3.moral Non Moral StandardDocument16 pages3.moral Non Moral StandardDaisy Daguplo BautistaNo ratings yet
- Introduction To SMART Objectives and SMART GoalsDocument9 pagesIntroduction To SMART Objectives and SMART GoalsRandy ManaloNo ratings yet
- Are Adolescents Less Mature Than Adults?Document12 pagesAre Adolescents Less Mature Than Adults?Regina OrdoñaNo ratings yet
- Relationship Between Salary and Job SatisfactionDocument28 pagesRelationship Between Salary and Job SatisfactionUyen Tran0% (1)
- HLTB50 Close Reading AssignmentDocument4 pagesHLTB50 Close Reading Assignmentnavafaria03No ratings yet
- HRD Audit Instruments QuestionnaireDocument27 pagesHRD Audit Instruments QuestionnaireSneha Chavan100% (2)
- PE/Health Course OutlineDocument4 pagesPE/Health Course Outlineapi-17070066No ratings yet
- A Review On Peer Correction: Writing 5Document4 pagesA Review On Peer Correction: Writing 5dphvuNo ratings yet
- COM 20041 Address Complex ChallengesDocument12 pagesCOM 20041 Address Complex ChallengesBrian WereNo ratings yet
- KVE401Document10 pagesKVE401sunny SINGHNo ratings yet
- The Science of Making Learning Stick AGES Model PDFDocument19 pagesThe Science of Making Learning Stick AGES Model PDFGilberto GarciaNo ratings yet
- Qualities of A Good Teacher and Techniques in Teaching Maryam BaigDocument7 pagesQualities of A Good Teacher and Techniques in Teaching Maryam Baigapi-310691943No ratings yet