Download as pdf or txt
You might also like
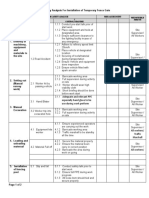
- ULSADO-JSA - Installation of Temporary Fence GateDocument2 pagesULSADO-JSA - Installation of Temporary Fence GateKelvin TanNo ratings yet
- A High-Value, Low-Cost Bubble Continuous Positive Airway Pressure System For Low-Resource Settings: Technical Assessment and Initial Case ReportsDocument6 pagesA High-Value, Low-Cost Bubble Continuous Positive Airway Pressure System For Low-Resource Settings: Technical Assessment and Initial Case ReportsnshamapNo ratings yet
- 146336-Article Text-386661-1-10-20161019Document8 pages146336-Article Text-386661-1-10-20161019Huri AbbasiNo ratings yet
- Saans - Efficacy of Multi-Powered Continuous Positive Airway Pressure DeviceDocument6 pagesSaans - Efficacy of Multi-Powered Continuous Positive Airway Pressure Deviceemailtrinaya30No ratings yet
- Outcomes in Neonates With Respiratory Distress Syndrome Using SAANS NIVDocument5 pagesOutcomes in Neonates With Respiratory Distress Syndrome Using SAANS NIVemailtrinaya30No ratings yet
- Immediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisDocument9 pagesImmediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisBelén María Vega AladueñaNo ratings yet
- Implementation of Conventional Air-Oxygen Blending in Multi-PoweredCPAPDeviceDocument7 pagesImplementation of Conventional Air-Oxygen Blending in Multi-PoweredCPAPDeviceABU TAUHEDNo ratings yet
- Neonatal Noninvasive Ventilation Techniques: Do We Really Need To Intubate?Document25 pagesNeonatal Noninvasive Ventilation Techniques: Do We Really Need To Intubate?sing terriblyNo ratings yet
- Home-Made Continuous Positive Airways Pressure Device May Reduce Mortality in Neonates With Respiratory Distress in Low-Resource SettingDocument5 pagesHome-Made Continuous Positive Airways Pressure Device May Reduce Mortality in Neonates With Respiratory Distress in Low-Resource SettingNovi AryandaNo ratings yet
- Journal NicuDocument4 pagesJournal NicuMargaret LlavorNo ratings yet
- Mechanical Ventilation of The Premature NeonateDocument16 pagesMechanical Ventilation of The Premature NeonateHaitham HafezNo ratings yet
- Intjprevmed6133-2704195 004504Document6 pagesIntjprevmed6133-2704195 004504Ade HabibieNo ratings yet
- Comparison of Saans Neonatal Continuous Positive Airway PressureDocument6 pagesComparison of Saans Neonatal Continuous Positive Airway Pressureemailtrinaya30No ratings yet
- Comparison Between Pre Post VAP Bundle - Kade Cintya PSDocument6 pagesComparison Between Pre Post VAP Bundle - Kade Cintya PSWidarma Atmaja, I KomangNo ratings yet
- Wright Et Al 2022 PDFDocument9 pagesWright Et Al 2022 PDFRadu CiprianNo ratings yet
- Neoreviews 2013 Keszler E237 51Document17 pagesNeoreviews 2013 Keszler E237 51Gun HawkNo ratings yet
- 589-Article Text-1298-1-10-20220830 PDFDocument12 pages589-Article Text-1298-1-10-20220830 PDFBella FebriantiNo ratings yet
- Guidelines For Surfactant Replacement Therapy in Neonates Canadian Paediatric SocietyDocument8 pagesGuidelines For Surfactant Replacement Therapy in Neonates Canadian Paediatric SocietyTiwi QiraNo ratings yet
- NIVHFODocument37 pagesNIVHFOSaleem HamilahNo ratings yet
- Conti 2016Document7 pagesConti 2016Dwi Putri SekariniNo ratings yet
- MainDocument6 pagesMaintrikusumawatiNo ratings yet
- A Pilot Prospective Study On Closed Loop Controlled Ventilation and Oxygenation in Ventilated Children During The Weaning PhaseDocument9 pagesA Pilot Prospective Study On Closed Loop Controlled Ventilation and Oxygenation in Ventilated Children During The Weaning PhaseSiti HumairahNo ratings yet
- GUPTA 2009 - A RCT of Post Extubation BCPAP Versus Infant Flow Driver CPAP in Preterm Infants With RDSDocument8 pagesGUPTA 2009 - A RCT of Post Extubation BCPAP Versus Infant Flow Driver CPAP in Preterm Infants With RDSRafael JustinoNo ratings yet
- VAP in ChildrenDocument19 pagesVAP in Childrensiekasmat upaNo ratings yet
- PILLOW 2012 - Innovation in Surfactant Therapy II-surfactant Administration by Aerosolization.Document8 pagesPILLOW 2012 - Innovation in Surfactant Therapy II-surfactant Administration by Aerosolization.Rafael JustinoNo ratings yet
- Synchronized Nasal Intermittent Positive Pressure Ventilation of The Newborn: Technical Issues and Clinical ResultsDocument7 pagesSynchronized Nasal Intermittent Positive Pressure Ventilation of The Newborn: Technical Issues and Clinical ResultsMaluNo ratings yet
- NakatoIJP Volume6 Issue9 Pages8215-8223Document9 pagesNakatoIJP Volume6 Issue9 Pages8215-8223Siti HumairahNo ratings yet
- Fraction of Inspired Oxygen As A Predictor of CPAP Failure in Preterm Infants With Respiratory Distress Syndrome: A Prospective Multicenter StudyDocument8 pagesFraction of Inspired Oxygen As A Predictor of CPAP Failure in Preterm Infants With Respiratory Distress Syndrome: A Prospective Multicenter StudyMaluNo ratings yet
- New Developments in Neonatal Respiratory MenagmentDocument7 pagesNew Developments in Neonatal Respiratory MenagmentTin TomašićNo ratings yet
- Ventilator Associated Pneumonia in ChildrenDocument7 pagesVentilator Associated Pneumonia in ChildrendarlingcarvajalduqueNo ratings yet
- Pedia ClerkshipDocument4 pagesPedia Clerkshipmarjorie_eyesNo ratings yet
- 09 InglesDocument8 pages09 InglesJulissa BarciaNo ratings yet
- s13063 019 3455 8Document9 pagess13063 019 3455 8Yusuf riskaNo ratings yet
- Fmed 09 920549Document8 pagesFmed 09 920549Fernando DornelNo ratings yet
- 2020 - Long-Term Non-Invasive Ventilation in Children - Current Use, Indications, and ContraindicationsDocument9 pages2020 - Long-Term Non-Invasive Ventilation in Children - Current Use, Indications, and ContraindicationsHack clashNo ratings yet
- Bubble C Pap SopDocument6 pagesBubble C Pap SopSupianto SuoiantoNo ratings yet
- Bmhim 22 79 4 237-247Document11 pagesBmhim 22 79 4 237-247AnapaolaNo ratings yet
- High Flow Nasal Cannula Versus Continuous Positive Airway PressureDocument13 pagesHigh Flow Nasal Cannula Versus Continuous Positive Airway PressurefitriNo ratings yet
- 1 - Immediate Effects and Safety of High-Frequency Chest WallDocument9 pages1 - Immediate Effects and Safety of High-Frequency Chest Wallblancabasquet8No ratings yet
- Jurnal Pubme 1 RdsDocument13 pagesJurnal Pubme 1 Rdsriri risna aNo ratings yet
- Non Invasive Respiratory Support in Preterm I - 2022 - Paediatric Respiratory ReDocument7 pagesNon Invasive Respiratory Support in Preterm I - 2022 - Paediatric Respiratory ReEduardo Rios DuboisNo ratings yet
- Guidelines For Surfactant Replacement Therapy in NeonatesDocument7 pagesGuidelines For Surfactant Replacement Therapy in NeonatesFer45No ratings yet
- American Journal of Infection ControlDocument8 pagesAmerican Journal of Infection ControlRizky AdipratamaNo ratings yet
- Canadian Guidelines 2021Document7 pagesCanadian Guidelines 2021Radu CiprianNo ratings yet
- Pxaa 116Document7 pagesPxaa 116Geísa VasconcelosNo ratings yet
- Global Assistance of Infant ResuscitationDocument8 pagesGlobal Assistance of Infant Resuscitationapi-347118128No ratings yet
- 693 FullDocument12 pages693 FullGilmer alvarez floresNo ratings yet
- Acdfne - Efectos Sistémicos y Pulmonares de Hidrocortisona en Prematuros Ventilados - Nienke HalmeijerDocument245 pagesAcdfne - Efectos Sistémicos y Pulmonares de Hidrocortisona en Prematuros Ventilados - Nienke HalmeijerChristian Isaac Rodriguez MoranNo ratings yet
- POLIN 2009 - Bubble CPAP - A Clash of Science Culture and ReligionDocument2 pagesPOLIN 2009 - Bubble CPAP - A Clash of Science Culture and ReligionRafael JustinoNo ratings yet
- HFGHHJV DocumentDocument7 pagesHFGHHJV DocumentYosi PramelisaNo ratings yet
- GIZZI 2012 - Surfactant and Non Invasive Ventilation For Preterm InfantsDocument4 pagesGIZZI 2012 - Surfactant and Non Invasive Ventilation For Preterm InfantsRafael JustinoNo ratings yet
- Kawaza: Low Cost Bubble CPAP For Managing Neonatal Respiratory Distress in MalawiDocument31 pagesKawaza: Low Cost Bubble CPAP For Managing Neonatal Respiratory Distress in MalawiNewborn2013No ratings yet
- 10 3389-Fped 2022 986695-CitationDocument1 page10 3389-Fped 2022 986695-CitationNuke PratiwiNo ratings yet
- E868 FullDocument10 pagesE868 FullCalvin AffendyNo ratings yet
- Bubble CPAP Vs Ventilatory CPAPDocument9 pagesBubble CPAP Vs Ventilatory CPAPRyan Rahman OesmanNo ratings yet
- Cpap TPPDocument24 pagesCpap TPPEng Evellius KyobyaNo ratings yet
- The Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesDocument5 pagesThe Role of Delayed Cord Clamping in Improving The Outcome in Preterm BabiesJehangir AllamNo ratings yet
- Br. J. Anaesth.-2013-Lee-81-6Document6 pagesBr. J. Anaesth.-2013-Lee-81-6ety lienNo ratings yet
- Non-Invasive Respiratory Support in Preterm Infants 2022Document7 pagesNon-Invasive Respiratory Support in Preterm Infants 2022DraalexNo ratings yet
- Impact Factor: 8.423: Volume 12, Issue 4, April 2023Document9 pagesImpact Factor: 8.423: Volume 12, Issue 4, April 2023ted gcgdNo ratings yet
- Ronshaela Nailer Wholenessisholiness Psy440Document7 pagesRonshaela Nailer Wholenessisholiness Psy440api-558577764No ratings yet
- The Effect of Weekly Training Load Across A Competitive Microcycle On Contextual Variables in Professional SoccerDocument10 pagesThe Effect of Weekly Training Load Across A Competitive Microcycle On Contextual Variables in Professional SoccerAmin CherbitiNo ratings yet
- NSTP CWTS Module 2Document6 pagesNSTP CWTS Module 2Shiedrick Conde BacolodNo ratings yet
- HMB342 Course Syllabus Summer 2020Document5 pagesHMB342 Course Syllabus Summer 2020WangNo ratings yet
- Effective Rejuvenation With Hyaluronic Acid Fillers: Current Advanced ConceptsDocument13 pagesEffective Rejuvenation With Hyaluronic Acid Fillers: Current Advanced ConceptsCamila De Lizier MesquitaNo ratings yet
- CLP Info SheetDocument6 pagesCLP Info SheetCarolina Mateus MoreiraNo ratings yet
- 2020 Tanzania in FiguresDocument110 pages2020 Tanzania in FiguresDaveNo ratings yet
- Bobcat Skid Steer Loader s770 Operation Maintenance ManualsDocument22 pagesBobcat Skid Steer Loader s770 Operation Maintenance Manualsmorganweiss270691imz100% (71)
- Test Bank For Comprehensive Perinatal and Pediatric Respiratory Care, 4th Edition, by Whitaker, ISBN-10: 1439059438, ISBN-13: 9781439059432Document36 pagesTest Bank For Comprehensive Perinatal and Pediatric Respiratory Care, 4th Edition, by Whitaker, ISBN-10: 1439059438, ISBN-13: 9781439059432meghantaylorxzfyijkotm100% (19)
- Unilateral Retinitis Pigmentosa: Case Report and Review of The LiteratureDocument8 pagesUnilateral Retinitis Pigmentosa: Case Report and Review of The LiteratureWidyawati SasmitaNo ratings yet
- Demographic Transition Model 2021Document23 pagesDemographic Transition Model 2021Abigail WaiteNo ratings yet
- Element - 45 - 978-Design ReportDocument15 pagesElement - 45 - 978-Design ReportLeeNo ratings yet
- The Evolution of A Different Voice in Family Therapy: Conversation Between Lynn Hoffman and Darryl WheatDocument12 pagesThe Evolution of A Different Voice in Family Therapy: Conversation Between Lynn Hoffman and Darryl WheatMaNo ratings yet
- Moh. Fahmi Suratinoyo - 0301777 - OsteomielitisDocument43 pagesMoh. Fahmi Suratinoyo - 0301777 - OsteomielitisFahmiNo ratings yet
- Pradipta Diwangkara - 29320469 - SMEMBA 5 - Planning For NegotiationsDocument3 pagesPradipta Diwangkara - 29320469 - SMEMBA 5 - Planning For NegotiationsFau ZanNo ratings yet
- Salutogenesis in Healthcare SettingsDocument10 pagesSalutogenesis in Healthcare SettingsGulienne Randee Mickhaela ZamoraNo ratings yet
- Aeonmed VentilatorDocument6 pagesAeonmed VentilatorStalin SebastirajNo ratings yet
- Analisa Risiko Kecelakaan Kerja Pada Proyek Konstruksi Jembatan Musi Vi PalembangDocument6 pagesAnalisa Risiko Kecelakaan Kerja Pada Proyek Konstruksi Jembatan Musi Vi PalembangRoraNo ratings yet
- Scharlab S.L. Certificate of Analysis: Plate Count Agar (Pca)Document1 pageScharlab S.L. Certificate of Analysis: Plate Count Agar (Pca)Jhon Jairo Riaño MartinezNo ratings yet
- Buntis Congress Report 2021Document24 pagesBuntis Congress Report 2021Giselle ArenasNo ratings yet
- 830 - Advanced Level Grammar Exercise MCQ Test 7Document3 pages830 - Advanced Level Grammar Exercise MCQ Test 7sohailfaisal2006No ratings yet
- Birthday Party - Character SketchesDocument2 pagesBirthday Party - Character SketchesDhivyaNo ratings yet
- ANKYLOS Laboratory ManualDocument100 pagesANKYLOS Laboratory ManualheycoolalexNo ratings yet
- The Wordsley Step Incision For Axillary Lymph-Node DissectionDocument1 pageThe Wordsley Step Incision For Axillary Lymph-Node DissectionVlad GrigoreNo ratings yet
- Hospital List-MD INDIA HealthcareDocument288 pagesHospital List-MD INDIA HealthcarePankaj67% (12)
- Mariano Marcos State University: College of Health SciencesDocument5 pagesMariano Marcos State University: College of Health SciencesLyca Mae Aurelio100% (1)
- Optimal Routine 940813Document23 pagesOptimal Routine 940813Mónica C HycNo ratings yet
- Malpositions and Malpresentations of The Fetal Head: ReviewDocument9 pagesMalpositions and Malpresentations of The Fetal Head: ReviewIntan PermataNo ratings yet
- Unit 4 Vocab ComicDocument10 pagesUnit 4 Vocab ComicTrúc TrúcNo ratings yet