
Somatic Symptoms
Somatic Symptoms
You might also like
- Ан яз тестDocument82 pagesАн яз тестPopi PopiNo ratings yet
- PCS-921 - X - Instruction Manual - EN - Overseas General - X - R1.02 - (EN - FZBH5101.0086.0003) PDFDocument276 pagesPCS-921 - X - Instruction Manual - EN - Overseas General - X - R1.02 - (EN - FZBH5101.0086.0003) PDFLeister Carneiro TheodoroNo ratings yet
- Unit 6Document24 pagesUnit 6Kerry KemuntoNo ratings yet
- Nelson en Ingles Capitulos 16 A 20Document81 pagesNelson en Ingles Capitulos 16 A 20Mario TurichNo ratings yet
- Horizon Degree and Commerce College Chakwal: Psychopathology Assignment No. 1 Somatic Symptom and Related DisordersDocument18 pagesHorizon Degree and Commerce College Chakwal: Psychopathology Assignment No. 1 Somatic Symptom and Related DisordersMuhammad Waseem AkhtarNo ratings yet
- Somatic Conditons Dolline and TarahDocument10 pagesSomatic Conditons Dolline and TarahDolline BusoloNo ratings yet
- Somatic Symptom and Related Disorders Presentation by Ngwu GinikaDocument35 pagesSomatic Symptom and Related Disorders Presentation by Ngwu Ginikangwuginika3No ratings yet
- 3 Somatic and DissociativeDocument7 pages3 Somatic and DissociativeMarian AlinoodNo ratings yet
- Somatoform DisordersDocument40 pagesSomatoform DisordersDr-Mohamed EssawyNo ratings yet
- Week 11 Somatic Symptom and Related DisordersDocument55 pagesWeek 11 Somatic Symptom and Related DisordersmballestaNo ratings yet
- PSPA3714 Chapter 6 2021Document59 pagesPSPA3714 Chapter 6 2021Kamogelo Makhura100% (1)
- (FirstAidSeries) Somatic SymptomDocument6 pages(FirstAidSeries) Somatic SymptomLuz Maria RojasNo ratings yet
- Somatoform DisordersDocument18 pagesSomatoform DisordersKaren Garcia AbinsayNo ratings yet
- Somatic Symptoms and Related Disorder: Muh. Irsan HidayatDocument16 pagesSomatic Symptoms and Related Disorder: Muh. Irsan HidayatMuhammad Irsan HidayatNo ratings yet
- Continuing Education Activity: Somatic Syndrome DisordersDocument6 pagesContinuing Education Activity: Somatic Syndrome DisordersAlgifari AdnanNo ratings yet
- Somatoform DisordersDocument41 pagesSomatoform DisordersTulika SarkarNo ratings yet
- Abnormal PsychologyDocument19 pagesAbnormal PsychologyEzekiel LiwanagNo ratings yet
- Psychiatric Aspects of Somatic Disorder in Child andDocument61 pagesPsychiatric Aspects of Somatic Disorder in Child andZubair Mahmood KamalNo ratings yet
- Somatoform DisordersDocument15 pagesSomatoform DisordersSimranjeet KaurNo ratings yet
- Somatic Symptom DisorderDocument55 pagesSomatic Symptom DisorderZubair Mahmood KamalNo ratings yet
- Presentation On Somatic Symptom Disorder and Related Disorders FinalizedDocument26 pagesPresentation On Somatic Symptom Disorder and Related Disorders FinalizedkiptooelvisaNo ratings yet
- Somatic Related Disorders Review LectureDocument7 pagesSomatic Related Disorders Review LectureMane SharNo ratings yet
- Somatic Symptom and Dissociative Disorders: Learning ObjectivesDocument34 pagesSomatic Symptom and Dissociative Disorders: Learning ObjectivesRUIJIE JiangNo ratings yet
- DSM V Background and Criteria: Schizophrenia Spectrum and Other Psychotic DisorderDocument20 pagesDSM V Background and Criteria: Schizophrenia Spectrum and Other Psychotic DisorderRhea Andrea UyNo ratings yet
- Case Study 2 ConversionDocument6 pagesCase Study 2 ConversionTabe TNo ratings yet
- Jurnal Somatoform PDFDocument6 pagesJurnal Somatoform PDFKiky RatnaNo ratings yet
- Advanced Abnormal Psychology: (Somatic Symptoms and Related Disorders)Document19 pagesAdvanced Abnormal Psychology: (Somatic Symptoms and Related Disorders)Rosemary LandanNo ratings yet
- Somatoform Disorders 2019Document91 pagesSomatoform Disorders 2019Poonam RanaNo ratings yet
- Overview of Somatoform DisordersDocument34 pagesOverview of Somatoform DisordersmebibegNo ratings yet
- Week 7Document33 pagesWeek 7Capal Anna MarieNo ratings yet
- Somatoform Disorders in Primary Care: Yeung AS, He DJ. Somatoform Disorder. Western Journal of Medicine 176Document10 pagesSomatoform Disorders in Primary Care: Yeung AS, He DJ. Somatoform Disorder. Western Journal of Medicine 176Ayu Aprilita BastariNo ratings yet
- Medically Unexplained Symptoms Assessment and ManagementDocument6 pagesMedically Unexplained Symptoms Assessment and ManagementMatheus AzevedoNo ratings yet
- Bailey Powell And: Catherine Kircos Third HourDocument22 pagesBailey Powell And: Catherine Kircos Third HourrinnzorNo ratings yet
- A Comparison of Somatic Symptoms Between Depressive Disorder and Somatoform DisorderDocument8 pagesA Comparison of Somatic Symptoms Between Depressive Disorder and Somatoform DisorderInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Major Depression: Reporter'S Neliza P. Aldana Jesus L. Atrero Mhylene Mon Bsn-IvDocument25 pagesMajor Depression: Reporter'S Neliza P. Aldana Jesus L. Atrero Mhylene Mon Bsn-Ivazilen16No ratings yet
- Somatoform DisordersDocument18 pagesSomatoform Disordersapi-376421589% (9)
- Chronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsFrom EverandChronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsNo ratings yet
- Fragmente Anxietate Si Somatica Din DSM 5Document8 pagesFragmente Anxietate Si Somatica Din DSM 51222No ratings yet
- Somatization DisorderDocument3 pagesSomatization DisorderVinceNo ratings yet
- Clinical Practice Guidelines for the Management of.11Document6 pagesClinical Practice Guidelines for the Management of.11Pavitra ShankarNo ratings yet
- Hysteria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHysteria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hypochondriasis, (Illness Anxiety Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypochondriasis, (Illness Anxiety Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Somatic Symptom and Related Disorders: Somatoform Disorder Mental IllnessDocument3 pagesSomatic Symptom and Related Disorders: Somatoform Disorder Mental IllnessmemeyNo ratings yet
- Psychiatry Reporting - Classification in PsychiatryDocument13 pagesPsychiatry Reporting - Classification in PsychiatryJyl Yan SelasorNo ratings yet
- What Is in DSM 5 - Thirusur - Aug 10 2013 - FinalDocument85 pagesWhat Is in DSM 5 - Thirusur - Aug 10 2013 - FinalNavina SureshNo ratings yet
- Unit 4 Somatoform & Dissociative DisorderDocument12 pagesUnit 4 Somatoform & Dissociative DisorderSushant NeupaneNo ratings yet
- Somatic and Related DisordersDocument4 pagesSomatic and Related DisordersSUPRANo ratings yet
- Somatoform DisordersDocument11 pagesSomatoform DisordersDr. Nivas SaminathanNo ratings yet
- Peripartum Depression - Does It Occur in Fathers and Does It Matter?Document11 pagesPeripartum Depression - Does It Occur in Fathers and Does It Matter?Ionela BogdanNo ratings yet
- Care MD ApproachDocument7 pagesCare MD ApproachDewina Dyani Rosari IINo ratings yet
- Somatic Symptom and Related DisordersDocument17 pagesSomatic Symptom and Related DisordersIllu MinaNo ratings yet
- Coa Revised Paper.Document16 pagesCoa Revised Paper.Justine AlexandraNo ratings yet
- 05 Somatic and Eating DisordersDocument79 pages05 Somatic and Eating DisordersSteven T.No ratings yet
- TG 7 Somatoform Des 2013 (DR - Lucky)Document35 pagesTG 7 Somatoform Des 2013 (DR - Lucky)Novi AdriNo ratings yet
- Feb 6 Introd Results Disc GPSY 513 Research Paper References AbstractDocument6 pagesFeb 6 Introd Results Disc GPSY 513 Research Paper References AbstractEva MartinNo ratings yet
- Articulo de RevisionDocument19 pagesArticulo de RevisionConsulta externa Clinica montserratNo ratings yet
- Psychosocial Correlates of Symptoms in Functional DyspepsiaDocument8 pagesPsychosocial Correlates of Symptoms in Functional DyspepsiaTaufiqurrokhman RofiiNo ratings yet
- Summary of Somatic Symptoms DisorderDocument3 pagesSummary of Somatic Symptoms DisorderMarlon BubaNo ratings yet
- 52 Somatic Symptom IbrahimDocument50 pages52 Somatic Symptom Ibrahimngocd6304No ratings yet
- Premenstrual Dysphoric Disorder: Clinical PracticeDocument6 pagesPremenstrual Dysphoric Disorder: Clinical PracticeIrmagian PaleonNo ratings yet
- Somat IC Sympt OM Disor DersDocument9 pagesSomat IC Sympt OM Disor DersShweta DasNo ratings yet
- Schizophrenia - Practice Essentials, Background, PathophysiologyDocument10 pagesSchizophrenia - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- Love in IslamDocument25 pagesLove in IslamSAPFIGUY1No ratings yet
- Impact Test On Steel SampleDocument4 pagesImpact Test On Steel SampleAdil Javed Chaudhary100% (2)
- Tugas Arsitektur Komputer Paralel4Document9 pagesTugas Arsitektur Komputer Paralel4Grasiadi HersantoNo ratings yet
- AutodeskCertifiedUserAutoCADExamOverview PDFDocument5 pagesAutodeskCertifiedUserAutoCADExamOverview PDFAyman KandeelNo ratings yet
- Agilent 54600B Oscilloscope Data SheetDocument8 pagesAgilent 54600B Oscilloscope Data SheetAlejandro CasasNo ratings yet
- Effectiveness of Distribution Channel of Minute MaidDocument29 pagesEffectiveness of Distribution Channel of Minute MaidZil Shah0% (1)
- Ghana Maketing PlanDocument11 pagesGhana Maketing PlanchiranrgNo ratings yet
- Arya PDFDocument26 pagesArya PDFRahmawati JuliaNo ratings yet
- Math Lesson 23Document5 pagesMath Lesson 23api-461550649No ratings yet
- v1 AB4013 DillonDocument12 pagesv1 AB4013 DillonMohammed AlnasharNo ratings yet
- General Instructions:: PRACTICE PAPER (2018-19) Class: Xii Max. Marks:70 Subject: Chemistry Time: 3 HoursDocument8 pagesGeneral Instructions:: PRACTICE PAPER (2018-19) Class: Xii Max. Marks:70 Subject: Chemistry Time: 3 HoursHINDI CARTOONSNo ratings yet
- AlstomGroup - JD For Software EngineerDocument3 pagesAlstomGroup - JD For Software EngineerPraveen PremachandranNo ratings yet
- The Prayer of Faith by Leonard Boase PDFDocument69 pagesThe Prayer of Faith by Leonard Boase PDF6luke3738No ratings yet
- Modernity-An Incomplete Project: Jurg en Habe RM AsDocument8 pagesModernity-An Incomplete Project: Jurg en Habe RM AsLouis DysonNo ratings yet
- Beginning Practicecu EdocDocument128 pagesBeginning Practicecu Edocapi-236393707No ratings yet
- "Behavioral and Experimental Economics": Written Exam For The M.Sc. in Economics 2010-IDocument4 pages"Behavioral and Experimental Economics": Written Exam For The M.Sc. in Economics 2010-ICoxorange94187No ratings yet
- WorkationDocument2 pagesWorkationNadiia BeleiNo ratings yet
- A Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Document67 pagesA Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Juan MendozaNo ratings yet
- Ajay Stats AssignmentDocument21 pagesAjay Stats AssignmentAkhil RawatNo ratings yet
- Setiawan D S, Tjahyono K, Afifah D N. 2016Document7 pagesSetiawan D S, Tjahyono K, Afifah D N. 2016Ismi WahyuniNo ratings yet
- Colas 4 WorkbookDocument86 pagesColas 4 WorkbookTimothyNo ratings yet
- What Got You Here, Won't Get You ThereDocument19 pagesWhat Got You Here, Won't Get You Thereyannis7100% (1)
- Assignment (Case Analysis)Document4 pagesAssignment (Case Analysis)Anupom Hossain SoumikNo ratings yet
- Coleman Puer AscaniusDocument7 pagesColeman Puer AscaniusFabian KänzigNo ratings yet
- Whitefly Biology PDFDocument27 pagesWhitefly Biology PDFJulian LeonardoNo ratings yet
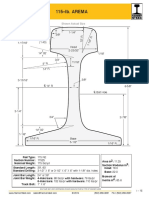
- Arema 115REDocument1 pageArema 115REAntonioNo ratings yet
- Project On Recruit Ment SlectionDocument6 pagesProject On Recruit Ment SlectionSunny KhushdilNo ratings yet
- IMUNISASIDocument26 pagesIMUNISASINadia KhoiriyahNo ratings yet
























































































Download as pdf or txt
You might also like
- Ан яз тестDocument82 pagesАн яз тестPopi PopiNo ratings yet
- PCS-921 - X - Instruction Manual - EN - Overseas General - X - R1.02 - (EN - FZBH5101.0086.0003) PDFDocument276 pagesPCS-921 - X - Instruction Manual - EN - Overseas General - X - R1.02 - (EN - FZBH5101.0086.0003) PDFLeister Carneiro TheodoroNo ratings yet
- Unit 6Document24 pagesUnit 6Kerry KemuntoNo ratings yet
- Nelson en Ingles Capitulos 16 A 20Document81 pagesNelson en Ingles Capitulos 16 A 20Mario TurichNo ratings yet
- Horizon Degree and Commerce College Chakwal: Psychopathology Assignment No. 1 Somatic Symptom and Related DisordersDocument18 pagesHorizon Degree and Commerce College Chakwal: Psychopathology Assignment No. 1 Somatic Symptom and Related DisordersMuhammad Waseem AkhtarNo ratings yet
- Somatic Conditons Dolline and TarahDocument10 pagesSomatic Conditons Dolline and TarahDolline BusoloNo ratings yet
- Somatic Symptom and Related Disorders Presentation by Ngwu GinikaDocument35 pagesSomatic Symptom and Related Disorders Presentation by Ngwu Ginikangwuginika3No ratings yet
- 3 Somatic and DissociativeDocument7 pages3 Somatic and DissociativeMarian AlinoodNo ratings yet
- Somatoform DisordersDocument40 pagesSomatoform DisordersDr-Mohamed EssawyNo ratings yet
- Week 11 Somatic Symptom and Related DisordersDocument55 pagesWeek 11 Somatic Symptom and Related DisordersmballestaNo ratings yet
- PSPA3714 Chapter 6 2021Document59 pagesPSPA3714 Chapter 6 2021Kamogelo Makhura100% (1)
- (FirstAidSeries) Somatic SymptomDocument6 pages(FirstAidSeries) Somatic SymptomLuz Maria RojasNo ratings yet
- Somatoform DisordersDocument18 pagesSomatoform DisordersKaren Garcia AbinsayNo ratings yet
- Somatic Symptoms and Related Disorder: Muh. Irsan HidayatDocument16 pagesSomatic Symptoms and Related Disorder: Muh. Irsan HidayatMuhammad Irsan HidayatNo ratings yet
- Continuing Education Activity: Somatic Syndrome DisordersDocument6 pagesContinuing Education Activity: Somatic Syndrome DisordersAlgifari AdnanNo ratings yet
- Somatoform DisordersDocument41 pagesSomatoform DisordersTulika SarkarNo ratings yet
- Abnormal PsychologyDocument19 pagesAbnormal PsychologyEzekiel LiwanagNo ratings yet
- Psychiatric Aspects of Somatic Disorder in Child andDocument61 pagesPsychiatric Aspects of Somatic Disorder in Child andZubair Mahmood KamalNo ratings yet
- Somatoform DisordersDocument15 pagesSomatoform DisordersSimranjeet KaurNo ratings yet
- Somatic Symptom DisorderDocument55 pagesSomatic Symptom DisorderZubair Mahmood KamalNo ratings yet
- Presentation On Somatic Symptom Disorder and Related Disorders FinalizedDocument26 pagesPresentation On Somatic Symptom Disorder and Related Disorders FinalizedkiptooelvisaNo ratings yet
- Somatic Related Disorders Review LectureDocument7 pagesSomatic Related Disorders Review LectureMane SharNo ratings yet
- Somatic Symptom and Dissociative Disorders: Learning ObjectivesDocument34 pagesSomatic Symptom and Dissociative Disorders: Learning ObjectivesRUIJIE JiangNo ratings yet
- DSM V Background and Criteria: Schizophrenia Spectrum and Other Psychotic DisorderDocument20 pagesDSM V Background and Criteria: Schizophrenia Spectrum and Other Psychotic DisorderRhea Andrea UyNo ratings yet
- Case Study 2 ConversionDocument6 pagesCase Study 2 ConversionTabe TNo ratings yet
- Jurnal Somatoform PDFDocument6 pagesJurnal Somatoform PDFKiky RatnaNo ratings yet
- Advanced Abnormal Psychology: (Somatic Symptoms and Related Disorders)Document19 pagesAdvanced Abnormal Psychology: (Somatic Symptoms and Related Disorders)Rosemary LandanNo ratings yet
- Somatoform Disorders 2019Document91 pagesSomatoform Disorders 2019Poonam RanaNo ratings yet
- Overview of Somatoform DisordersDocument34 pagesOverview of Somatoform DisordersmebibegNo ratings yet
- Week 7Document33 pagesWeek 7Capal Anna MarieNo ratings yet
- Somatoform Disorders in Primary Care: Yeung AS, He DJ. Somatoform Disorder. Western Journal of Medicine 176Document10 pagesSomatoform Disorders in Primary Care: Yeung AS, He DJ. Somatoform Disorder. Western Journal of Medicine 176Ayu Aprilita BastariNo ratings yet
- Medically Unexplained Symptoms Assessment and ManagementDocument6 pagesMedically Unexplained Symptoms Assessment and ManagementMatheus AzevedoNo ratings yet
- Bailey Powell And: Catherine Kircos Third HourDocument22 pagesBailey Powell And: Catherine Kircos Third HourrinnzorNo ratings yet
- A Comparison of Somatic Symptoms Between Depressive Disorder and Somatoform DisorderDocument8 pagesA Comparison of Somatic Symptoms Between Depressive Disorder and Somatoform DisorderInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Major Depression: Reporter'S Neliza P. Aldana Jesus L. Atrero Mhylene Mon Bsn-IvDocument25 pagesMajor Depression: Reporter'S Neliza P. Aldana Jesus L. Atrero Mhylene Mon Bsn-Ivazilen16No ratings yet
- Somatoform DisordersDocument18 pagesSomatoform Disordersapi-376421589% (9)
- Chronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsFrom EverandChronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsNo ratings yet
- Fragmente Anxietate Si Somatica Din DSM 5Document8 pagesFragmente Anxietate Si Somatica Din DSM 51222No ratings yet
- Somatization DisorderDocument3 pagesSomatization DisorderVinceNo ratings yet
- Clinical Practice Guidelines for the Management of.11Document6 pagesClinical Practice Guidelines for the Management of.11Pavitra ShankarNo ratings yet
- Hysteria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHysteria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hypochondriasis, (Illness Anxiety Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypochondriasis, (Illness Anxiety Disorder) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Somatic Symptom and Related Disorders: Somatoform Disorder Mental IllnessDocument3 pagesSomatic Symptom and Related Disorders: Somatoform Disorder Mental IllnessmemeyNo ratings yet
- Psychiatry Reporting - Classification in PsychiatryDocument13 pagesPsychiatry Reporting - Classification in PsychiatryJyl Yan SelasorNo ratings yet
- What Is in DSM 5 - Thirusur - Aug 10 2013 - FinalDocument85 pagesWhat Is in DSM 5 - Thirusur - Aug 10 2013 - FinalNavina SureshNo ratings yet
- Unit 4 Somatoform & Dissociative DisorderDocument12 pagesUnit 4 Somatoform & Dissociative DisorderSushant NeupaneNo ratings yet
- Somatic and Related DisordersDocument4 pagesSomatic and Related DisordersSUPRANo ratings yet
- Somatoform DisordersDocument11 pagesSomatoform DisordersDr. Nivas SaminathanNo ratings yet
- Peripartum Depression - Does It Occur in Fathers and Does It Matter?Document11 pagesPeripartum Depression - Does It Occur in Fathers and Does It Matter?Ionela BogdanNo ratings yet
- Care MD ApproachDocument7 pagesCare MD ApproachDewina Dyani Rosari IINo ratings yet
- Somatic Symptom and Related DisordersDocument17 pagesSomatic Symptom and Related DisordersIllu MinaNo ratings yet
- Coa Revised Paper.Document16 pagesCoa Revised Paper.Justine AlexandraNo ratings yet
- 05 Somatic and Eating DisordersDocument79 pages05 Somatic and Eating DisordersSteven T.No ratings yet
- TG 7 Somatoform Des 2013 (DR - Lucky)Document35 pagesTG 7 Somatoform Des 2013 (DR - Lucky)Novi AdriNo ratings yet
- Feb 6 Introd Results Disc GPSY 513 Research Paper References AbstractDocument6 pagesFeb 6 Introd Results Disc GPSY 513 Research Paper References AbstractEva MartinNo ratings yet
- Articulo de RevisionDocument19 pagesArticulo de RevisionConsulta externa Clinica montserratNo ratings yet
- Psychosocial Correlates of Symptoms in Functional DyspepsiaDocument8 pagesPsychosocial Correlates of Symptoms in Functional DyspepsiaTaufiqurrokhman RofiiNo ratings yet
- Summary of Somatic Symptoms DisorderDocument3 pagesSummary of Somatic Symptoms DisorderMarlon BubaNo ratings yet
- 52 Somatic Symptom IbrahimDocument50 pages52 Somatic Symptom Ibrahimngocd6304No ratings yet
- Premenstrual Dysphoric Disorder: Clinical PracticeDocument6 pagesPremenstrual Dysphoric Disorder: Clinical PracticeIrmagian PaleonNo ratings yet
- Somat IC Sympt OM Disor DersDocument9 pagesSomat IC Sympt OM Disor DersShweta DasNo ratings yet
- Schizophrenia - Practice Essentials, Background, PathophysiologyDocument10 pagesSchizophrenia - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- Love in IslamDocument25 pagesLove in IslamSAPFIGUY1No ratings yet
- Impact Test On Steel SampleDocument4 pagesImpact Test On Steel SampleAdil Javed Chaudhary100% (2)
- Tugas Arsitektur Komputer Paralel4Document9 pagesTugas Arsitektur Komputer Paralel4Grasiadi HersantoNo ratings yet
- AutodeskCertifiedUserAutoCADExamOverview PDFDocument5 pagesAutodeskCertifiedUserAutoCADExamOverview PDFAyman KandeelNo ratings yet
- Agilent 54600B Oscilloscope Data SheetDocument8 pagesAgilent 54600B Oscilloscope Data SheetAlejandro CasasNo ratings yet
- Effectiveness of Distribution Channel of Minute MaidDocument29 pagesEffectiveness of Distribution Channel of Minute MaidZil Shah0% (1)
- Ghana Maketing PlanDocument11 pagesGhana Maketing PlanchiranrgNo ratings yet
- Arya PDFDocument26 pagesArya PDFRahmawati JuliaNo ratings yet
- Math Lesson 23Document5 pagesMath Lesson 23api-461550649No ratings yet
- v1 AB4013 DillonDocument12 pagesv1 AB4013 DillonMohammed AlnasharNo ratings yet
- General Instructions:: PRACTICE PAPER (2018-19) Class: Xii Max. Marks:70 Subject: Chemistry Time: 3 HoursDocument8 pagesGeneral Instructions:: PRACTICE PAPER (2018-19) Class: Xii Max. Marks:70 Subject: Chemistry Time: 3 HoursHINDI CARTOONSNo ratings yet
- AlstomGroup - JD For Software EngineerDocument3 pagesAlstomGroup - JD For Software EngineerPraveen PremachandranNo ratings yet
- The Prayer of Faith by Leonard Boase PDFDocument69 pagesThe Prayer of Faith by Leonard Boase PDF6luke3738No ratings yet
- Modernity-An Incomplete Project: Jurg en Habe RM AsDocument8 pagesModernity-An Incomplete Project: Jurg en Habe RM AsLouis DysonNo ratings yet
- Beginning Practicecu EdocDocument128 pagesBeginning Practicecu Edocapi-236393707No ratings yet
- "Behavioral and Experimental Economics": Written Exam For The M.Sc. in Economics 2010-IDocument4 pages"Behavioral and Experimental Economics": Written Exam For The M.Sc. in Economics 2010-ICoxorange94187No ratings yet
- WorkationDocument2 pagesWorkationNadiia BeleiNo ratings yet
- A Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Document67 pagesA Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Juan MendozaNo ratings yet
- Ajay Stats AssignmentDocument21 pagesAjay Stats AssignmentAkhil RawatNo ratings yet
- Setiawan D S, Tjahyono K, Afifah D N. 2016Document7 pagesSetiawan D S, Tjahyono K, Afifah D N. 2016Ismi WahyuniNo ratings yet
- Colas 4 WorkbookDocument86 pagesColas 4 WorkbookTimothyNo ratings yet
- What Got You Here, Won't Get You ThereDocument19 pagesWhat Got You Here, Won't Get You Thereyannis7100% (1)
- Assignment (Case Analysis)Document4 pagesAssignment (Case Analysis)Anupom Hossain SoumikNo ratings yet
- Coleman Puer AscaniusDocument7 pagesColeman Puer AscaniusFabian KänzigNo ratings yet
- Whitefly Biology PDFDocument27 pagesWhitefly Biology PDFJulian LeonardoNo ratings yet
- Arema 115REDocument1 pageArema 115REAntonioNo ratings yet
- Project On Recruit Ment SlectionDocument6 pagesProject On Recruit Ment SlectionSunny KhushdilNo ratings yet
- IMUNISASIDocument26 pagesIMUNISASINadia KhoiriyahNo ratings yet