Download as pdf or txt
You might also like
- Oman Prometric Exam NotesDocument417 pagesOman Prometric Exam NotesMuhammad Amin93% (14)
- Cardiac RehabilitationDocument9 pagesCardiac RehabilitationJisha JanardhanNo ratings yet
- Clinical Outcome of Periodontal Regenerative Therapy Using Collagen Membrane and Deproteinized Bovine Bone Mineral: A 2.5-Year Follow-Up StudyDocument8 pagesClinical Outcome of Periodontal Regenerative Therapy Using Collagen Membrane and Deproteinized Bovine Bone Mineral: A 2.5-Year Follow-Up Studyzakia velasufaNo ratings yet
- 2014 - Five-Year Clinical Results For Treatment of Intrabony Defects With EMD, Guided Tissue Regeneration and Open-Flap Debridement: A Case SeriesDocument8 pages2014 - Five-Year Clinical Results For Treatment of Intrabony Defects With EMD, Guided Tissue Regeneration and Open-Flap Debridement: A Case SeriesJontavius GilbertNo ratings yet
- Artigos para Ver MetodologiaDocument22 pagesArtigos para Ver Metodologiafernanda.calvoNo ratings yet
- Reconstructive Surgical Therapy of Peri-Implantitis: A Multicenter Randomized Controlled Clinical TrialDocument24 pagesReconstructive Surgical Therapy of Peri-Implantitis: A Multicenter Randomized Controlled Clinical Trialrmartins76No ratings yet
- Use of Fisiograft in Intrabony Defects-A Clinical and Radiological StudyDocument4 pagesUse of Fisiograft in Intrabony Defects-A Clinical and Radiological StudymaxNo ratings yet
- 2023 Photobiomodulation in Dental Implant Stability and Post-Surgical Healing and Inflammation. A Randomised Double-Blind Study 2023Document11 pages2023 Photobiomodulation in Dental Implant Stability and Post-Surgical Healing and Inflammation. A Randomised Double-Blind Study 2023michelNo ratings yet
- Ferrarotti Et Al. Journal of Clinical Periodontology (2018)Document10 pagesFerrarotti Et Al. Journal of Clinical Periodontology (2018)Jose Luis Bladco MorenoNo ratings yet
- Aatika 8Document7 pagesAatika 8Abhishek GuptaNo ratings yet
- RetrieveDocument10 pagesRetrieveDANTE DELEGUERYNo ratings yet
- Japid 14 26Document6 pagesJapid 14 26rikaNo ratings yet
- Journal of Periodontology - 2022 - Suárez López Del Amo - Efficacy of Biologics For Alveolar Ridge PreservationDocument21 pagesJournal of Periodontology - 2022 - Suárez López Del Amo - Efficacy of Biologics For Alveolar Ridge PreservationDadi SindhuNo ratings yet
- The Rationale of Surgical Treatment in Pediatric Spine TuberculosisDocument6 pagesThe Rationale of Surgical Treatment in Pediatric Spine TuberculosisSpica KentNo ratings yet
- Emdogain Research PDFDocument4 pagesEmdogain Research PDFMohammed NabeelNo ratings yet
- Emdogain Research: Emdogain in Regenerative Periodontal Therapy. A Review of The LiteratureDocument4 pagesEmdogain Research: Emdogain in Regenerative Periodontal Therapy. A Review of The LiteratureMohammed NabeelNo ratings yet
- Surgical Treatment of Peri-Implantitis: 3 - Year Results From A Randomized Controlled Clinical TrialDocument10 pagesSurgical Treatment of Peri-Implantitis: 3 - Year Results From A Randomized Controlled Clinical TrialFabian SanabriaNo ratings yet
- Autogenous - Mineralized - Dentin - Versus - Xenograft - Granules - in - Ridge - Preservation - For Delayed - Implantation - in - Post-Extraction - SitesDocument11 pagesAutogenous - Mineralized - Dentin - Versus - Xenograft - Granules - in - Ridge - Preservation - For Delayed - Implantation - in - Post-Extraction - SitesSamantha TavaresNo ratings yet
- 4280-Article Text-9949-10452-10-20220608Document5 pages4280-Article Text-9949-10452-10-20220608Daniel AtiehNo ratings yet
- Analysis of Clinical Outcomes in Connective Tissue Donor Site Healing With Two Different Suturing Protocols A Prospective Case Control StudyDocument13 pagesAnalysis of Clinical Outcomes in Connective Tissue Donor Site Healing With Two Different Suturing Protocols A Prospective Case Control StudyAthenaeum Scientific PublishersNo ratings yet
- Bone Replacement Grafts With Guided Tissue RegenerationDocument16 pagesBone Replacement Grafts With Guided Tissue RegenerationIrvin EduardoNo ratings yet
- 00-Treatment of Periodontal Intrabony Defects Using Bovine Porous Bone Mineral and Guided Tissue Regeneration With:without Platelet-Rich FibrinDocument8 pages00-Treatment of Periodontal Intrabony Defects Using Bovine Porous Bone Mineral and Guided Tissue Regeneration With:without Platelet-Rich FibrinaemontoNo ratings yet
- J Clinic Periodontology - 2019 - Dai - Long Term Stability of Root Coverage Procedures For Single Gingival Recessions ADocument14 pagesJ Clinic Periodontology - 2019 - Dai - Long Term Stability of Root Coverage Procedures For Single Gingival Recessions ADr.Niveditha SNo ratings yet
- Acute-Phase Response Following Full-Mouth Versus Quadrant Non-Surgical Periodontal Treatment: A Randomized Clinical TrialDocument10 pagesAcute-Phase Response Following Full-Mouth Versus Quadrant Non-Surgical Periodontal Treatment: A Randomized Clinical TrialValeria ParraNo ratings yet
- Journal of Periodontology - 2022 - Monje - Significance of Barrier Membrane On The Reconstructive Therapy ofDocument13 pagesJournal of Periodontology - 2022 - Monje - Significance of Barrier Membrane On The Reconstructive Therapy of安西 泰規No ratings yet
- Cirugia PeriodontalDocument7 pagesCirugia PeriodontalMelissa Muñoz GómezNo ratings yet
- Lasers: Effect of Low-Level Laser Therapy and Platelet-Rich Fibrin On The Treatment of Intra-Bony DefectsDocument8 pagesLasers: Effect of Low-Level Laser Therapy and Platelet-Rich Fibrin On The Treatment of Intra-Bony DefectsMegha PoojaryNo ratings yet
- 4Document23 pages4jeeveshNo ratings yet
- Clinical Paper Orthognathic Surgery: Int. J. Oral Maxillofac. Surg. 2015 XXX: XXX-XXXDocument8 pagesClinical Paper Orthognathic Surgery: Int. J. Oral Maxillofac. Surg. 2015 XXX: XXX-XXXRicardo BarcoNo ratings yet
- Clinical Benefits of Ridge Preservation For Implant Placement Compared To Natural Healing in Maxillary Teeth - A Retrospective StudyDocument10 pagesClinical Benefits of Ridge Preservation For Implant Placement Compared To Natural Healing in Maxillary Teeth - A Retrospective StudyCamilo Andrés Sabogal ArguelloNo ratings yet
- Comparison of Patient-Reported Outcomes Between Immediately and Conventionally Loaded Mandibular Two-Implant Overdentures: A Preliminary StudyDocument8 pagesComparison of Patient-Reported Outcomes Between Immediately and Conventionally Loaded Mandibular Two-Implant Overdentures: A Preliminary StudyGianna CrismariuNo ratings yet
- 18 - Clinical, Inflammatory and Microbiological Outcomes of Full-Mouth Scaling With Adjunctive Glycine Powder Air-Polishing - A Randomized TrialDocument25 pages18 - Clinical, Inflammatory and Microbiological Outcomes of Full-Mouth Scaling With Adjunctive Glycine Powder Air-Polishing - A Randomized TrialPietro SanzNo ratings yet
- Injectable Platelet Rich Fibrin With DemineralizedDocument22 pagesInjectable Platelet Rich Fibrin With DemineralizedDadi SindhuNo ratings yet
- Implant Supported Dentures and Masticatory PerformanceDocument1 pageImplant Supported Dentures and Masticatory PerformanceSandrinaPufinaNo ratings yet
- Bone Reports: Case ReportDocument8 pagesBone Reports: Case ReportDaniella NúñezNo ratings yet
- Journal of Clinical PeriodontolDocument11 pagesJournal of Clinical PeriodontolIonut HusdupNo ratings yet
- Evaluation of Effects of 1.2% Atorvastatin As A Local Drug Delivery: A Randomized Controlled Clinical StudyDocument8 pagesEvaluation of Effects of 1.2% Atorvastatin As A Local Drug Delivery: A Randomized Controlled Clinical StudyIJAR JOURNALNo ratings yet
- Case Report: Bull Tokyo Dent Coll (2023) 64 (4) : 145-155Document11 pagesCase Report: Bull Tokyo Dent Coll (2023) 64 (4) : 145-155gat.depthNo ratings yet
- 2023 Heitz-Mayfield Et Al - Surgical Peri-Implantitis Treatment With and Without Guided Bone Regeneration RCTDocument19 pages2023 Heitz-Mayfield Et Al - Surgical Peri-Implantitis Treatment With and Without Guided Bone Regeneration RCTGustavo Avila OrtizNo ratings yet
- Bmri2018 3982540Document10 pagesBmri2018 3982540paola lievanoNo ratings yet
- 10 1111@jcpe 12723Document34 pages10 1111@jcpe 12723Dr.Niveditha SNo ratings yet
- The Positive Effect of Tenting Screws For Primary Horizontal Guided Bone Regeneration - A Retrospective Study Based On Cone-Beam Computed Tomography Data - Hämmerle 2020Document10 pagesThe Positive Effect of Tenting Screws For Primary Horizontal Guided Bone Regeneration - A Retrospective Study Based On Cone-Beam Computed Tomography Data - Hämmerle 2020LEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- Dimensional Changes in Free Epithelialized Gingival/mucosal Grafts at Tooth and Implant Sites: A Prospective Cohort StudyDocument10 pagesDimensional Changes in Free Epithelialized Gingival/mucosal Grafts at Tooth and Implant Sites: A Prospective Cohort StudyDiana Pellecer de SmithNo ratings yet
- Journal Homepage: - : IntroductionDocument10 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- PROTOCOLO de Carga de Coronas Sobre ImplanteDocument17 pagesPROTOCOLO de Carga de Coronas Sobre ImplanteJohnny CHNo ratings yet
- Crestal Bone Level Around Tissue-Level Implants Restored With Platform Matching and Bone-Level ImplantsDocument9 pagesCrestal Bone Level Around Tissue-Level Implants Restored With Platform Matching and Bone-Level Implantscd.brendasotofloresNo ratings yet
- Clin Implant Dent Rel Res - 2023 - Amorfini - Implant Rehabilitation of The Esthetic Area A Five Year Retrospective SDocument9 pagesClin Implant Dent Rel Res - 2023 - Amorfini - Implant Rehabilitation of The Esthetic Area A Five Year Retrospective SDANTE DELEGUERYNo ratings yet
- Cortellini 2011Document9 pagesCortellini 2011alijnevNo ratings yet
- 7-Paulo M. Camargo 2009Document9 pages7-Paulo M. Camargo 2009Ashish DambhareNo ratings yet
- Liu 2021Document11 pagesLiu 2021jcNo ratings yet
- J Clinic Periodontology - 2020 - Slagter - Immediate Placement of Single Implants With or Without ImmediateDocument12 pagesJ Clinic Periodontology - 2020 - Slagter - Immediate Placement of Single Implants With or Without ImmediatecirurgiadentistathaisNo ratings yet
- Corresponding AuthorDocument21 pagesCorresponding Authorcd.brendasotofloresNo ratings yet
- J Clinic Periodontology - 2020 - Stavropoulos - Medium and Long Term Clinical Benefits of Periodontal RegenerativeDocument21 pagesJ Clinic Periodontology - 2020 - Stavropoulos - Medium and Long Term Clinical Benefits of Periodontal RegenerativejcNo ratings yet
- Facial Implant Gingival Level and Thickness Changes Following Maxillary AnteriorDocument10 pagesFacial Implant Gingival Level and Thickness Changes Following Maxillary AnteriorFelipe CastroNo ratings yet
- JIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyDocument8 pagesJIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyMedstudNo ratings yet
- JIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelDocument8 pagesJIAP July 2011 - Guided Tissue Regeneration - A Decision-Making ModelLouis HutahaeanNo ratings yet
- Koldsland Mantenimiento Periimplantitis 2020Document9 pagesKoldsland Mantenimiento Periimplantitis 2020Gonzalo CastroNo ratings yet
- Influence of The Fixed Implant-Supported Provisional Phase On The Esthetic Final Outcome of Implant-Supported Crowns. David Furze. 2019. Wiley PeriodicalsDocument7 pagesInfluence of The Fixed Implant-Supported Provisional Phase On The Esthetic Final Outcome of Implant-Supported Crowns. David Furze. 2019. Wiley PeriodicalsValeria CrespoNo ratings yet
- Ocr 12237Document11 pagesOcr 12237André FonsecaNo ratings yet
- A Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyDocument12 pagesA Immediate Implant With Provisionaliztion Journal of Clinical PeriodontologyAhmed BadrNo ratings yet
- RevisãosistematicaLousiana2019bom Pra Tec Mole e Quastionavel Pra OssoDocument11 pagesRevisãosistematicaLousiana2019bom Pra Tec Mole e Quastionavel Pra OssoGabriel Filipe Tosin ScivskiNo ratings yet
- 10 1016@j Prosdent 2019 10 015Document7 pages10 1016@j Prosdent 2019 10 015jcNo ratings yet
- Liu 2021Document11 pagesLiu 2021jcNo ratings yet
- Perioptix Flip Up Optics Frame ManualDocument8 pagesPerioptix Flip Up Optics Frame ManualjcNo ratings yet
- THESIS Dental CAD CAM Crowns Carbajal MejiaDocument58 pagesTHESIS Dental CAD CAM Crowns Carbajal MejiajcNo ratings yet
- Cholera and SalmonellaDocument5 pagesCholera and SalmonellaJonas Marvin Anaque100% (1)
- Laxatives Drugs: Wazir Ali ChandioDocument12 pagesLaxatives Drugs: Wazir Ali ChandioAyaz Hussain ChandioNo ratings yet
- The Hospital Team and Hospital DepartmentsDocument6 pagesThe Hospital Team and Hospital DepartmentsMauren Crestine Delos SantosNo ratings yet
- Cracked Tooth SyndromeDocument4 pagesCracked Tooth SyndromeANUBHANo ratings yet
- Acenocoumarol Drug Information, ProfessionalDocument47 pagesAcenocoumarol Drug Information, ProfessionalMoisés PonceNo ratings yet
- Oil Pulling MethodDocument5 pagesOil Pulling Methodcrsol100% (3)
- STI Guidelines 2021Document192 pagesSTI Guidelines 2021Carlos QuirozNo ratings yet
- D.S.S Aiims Prepration Test Series: Com M Un Ic Ab Le An D N On - Co M M Un Ic Ab Le Di Se AsDocument7 pagesD.S.S Aiims Prepration Test Series: Com M Un Ic Ab Le An D N On - Co M M Un Ic Ab Le Di Se AsDr-Sanjay SinghaniaNo ratings yet
- BPQ Questionnaire PDFDocument4 pagesBPQ Questionnaire PDFAymen DabboussiNo ratings yet
- Paper Iralivelya PDocument5 pagesPaper Iralivelya Pbless goodNo ratings yet
- Facial Nerve ParalysisDocument36 pagesFacial Nerve ParalysisSylvia Diamond100% (1)
- Scenario 1 Topic: Primary Care Dentist A. Difficult TermDocument4 pagesScenario 1 Topic: Primary Care Dentist A. Difficult Termaulia rahmasariNo ratings yet
- Mrs. A, 35 Years Old, MR 01 13 45 74, Severity Level IIIDocument18 pagesMrs. A, 35 Years Old, MR 01 13 45 74, Severity Level IIIprimaindra27No ratings yet
- Veterinary Clinic Design For Earth Centre, SierraDocument22 pagesVeterinary Clinic Design For Earth Centre, SierraThamir A. HijaziNo ratings yet
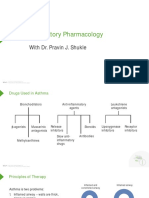
- Respiratory Pharmacology: With Dr. Pravin J. ShukleDocument28 pagesRespiratory Pharmacology: With Dr. Pravin J. ShukleKaish DahiyaNo ratings yet
- Pir 37-12 Enterovirus PPT Final PDFDocument10 pagesPir 37-12 Enterovirus PPT Final PDFbentoeNo ratings yet
- UntitledDocument12 pagesUntitledWayne Duritan OracionNo ratings yet
- Communicable Diseases of The Reproductive SystemDocument1 pageCommunicable Diseases of The Reproductive SystemSabita SinghNo ratings yet
- Overview of Mucocutaneous Symptom ComplexDocument5 pagesOverview of Mucocutaneous Symptom ComplexDaphne Jo ValmonteNo ratings yet
- Jurnal Pruritus SenilisDocument19 pagesJurnal Pruritus Seniliszubair zainalNo ratings yet
- MRCP 2Document26 pagesMRCP 2riyaz414No ratings yet
- Diseases Caused by MicroorganismsDocument9 pagesDiseases Caused by MicroorganismsKhushbuGuptaNo ratings yet
- Metabolic AcidosisDocument1 pageMetabolic AcidosisLee June LyngNo ratings yet
- Abduraham Rayyan-Module-Cardiovascular-SystemDocument17 pagesAbduraham Rayyan-Module-Cardiovascular-SystemRAYYAN ENIL ABDURAHAMNo ratings yet
- Subtrochanteric Femur Fractures: Current Review of ManagementDocument7 pagesSubtrochanteric Femur Fractures: Current Review of ManagementErmiNo ratings yet
- Lymphangitis TreatmentDocument2 pagesLymphangitis TreatmentHarista Miranda SalamNo ratings yet
- Stase BedahDocument148 pagesStase BedahHandika AprilliandaNo ratings yet