Download as docx, pdf, or txt
You might also like
- Nursing Study Guide Answer KeyDocument176 pagesNursing Study Guide Answer KeyKelsey Browne68% (19)
- Case Record FormDocument30 pagesCase Record FormVirag Patil100% (1)
- HISTORY TAKING QuestionsDocument4 pagesHISTORY TAKING QuestionsKlean Jee Teo-TrazoNo ratings yet
- The Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesFrom EverandThe Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesNo ratings yet
- Seeing The UnseenDocument8 pagesSeeing The UnseenCale HollowayNo ratings yet
- Assessment Tool - Nursing History Format SummaryDocument4 pagesAssessment Tool - Nursing History Format SummaryKeid Reuma100% (1)
- History TakingDocument2 pagesHistory TakingAmbar Rashid100% (1)
- Card Medical HistoryDocument4 pagesCard Medical HistoryDanonino12No ratings yet
- GuideDocument4 pagesGuideMia Grace GarciaNo ratings yet
- Nursing Interview Guide To Collect Subjective Data From The ClientDocument10 pagesNursing Interview Guide To Collect Subjective Data From The ClientDawn EncarnacionNo ratings yet
- Interview Guide QuestionsDocument3 pagesInterview Guide QuestionsYam KayeNo ratings yet
- Nursing Health History Assessment and Review of SystemsDocument2 pagesNursing Health History Assessment and Review of SystemsJohanna Recca MarinoNo ratings yet
- Assessment of The Childbearing Woman: Nursing Health History FormatDocument12 pagesAssessment of The Childbearing Woman: Nursing Health History FormatJmy CoronadoNo ratings yet
- Holistic Geriatric Assessment ToolDocument15 pagesHolistic Geriatric Assessment ToolMarianne DugosNo ratings yet
- Mija Rimay - Questions For SDDocument4 pagesMija Rimay - Questions For SDYaz GhorlNo ratings yet
- Nursing Health History Format (Used For Client Care Plan)Document2 pagesNursing Health History Format (Used For Client Care Plan)Hamid Colangcag AmborNo ratings yet
- Basic History Taking: Tim Communication Skill FKUBDocument30 pagesBasic History Taking: Tim Communication Skill FKUBnarulita_94No ratings yet
- SubjectiveDocument3 pagesSubjectivequiaNo ratings yet
- Screening For Health, Fitness and Wellness: Danish LatifDocument25 pagesScreening For Health, Fitness and Wellness: Danish LatifShimmering MoonNo ratings yet
- Health Assessment TAKE HOME ASSIGNMENT CH 4 The Complete Health History Name - Section - DateDocument5 pagesHealth Assessment TAKE HOME ASSIGNMENT CH 4 The Complete Health History Name - Section - DateAndy NguyenNo ratings yet
- Interview QsDocument6 pagesInterview QsRaise RaiseNo ratings yet
- Clinical AssignmentDocument8 pagesClinical AssignmentLauren NeisentNo ratings yet
- Station #: InstructionsDocument5 pagesStation #: InstructionscrcespNo ratings yet
- History TakingDocument8 pagesHistory TakingDarian BurkettNo ratings yet
- Winnyfred Patience Ayugi Bsc. MidwiferyDocument30 pagesWinnyfred Patience Ayugi Bsc. MidwiferyAYO NELSONNo ratings yet
- Chap 2 Collecting Subjective Data Interview GuideDocument6 pagesChap 2 Collecting Subjective Data Interview GuidePaguirigan, Louise AndreaNo ratings yet
- Golden Gate Colleges P. Prieto ST., Batangas City: College of NursingDocument7 pagesGolden Gate Colleges P. Prieto ST., Batangas City: College of NursingR Hornilla ArcegaNo ratings yet
- HA Lecture Week 5 ROSDocument6 pagesHA Lecture Week 5 ROSLore Anne Mhae SantosNo ratings yet
- NutritionalTherapy QuestionnaireDocument13 pagesNutritionalTherapy Questionnairehalima mainaNo ratings yet
- Nursing Interview Guide - HADocument6 pagesNursing Interview Guide - HAJohn CenaNo ratings yet
- Anamneza I Status InternaDocument12 pagesAnamneza I Status Internatajana91No ratings yet
- Nursing Interview Guide - HA - VIOSDocument9 pagesNursing Interview Guide - HA - VIOSIra Velle ViosNo ratings yet
- Family First Chiropractic Client Intake 03172Document6 pagesFamily First Chiropractic Client Intake 03172Trina AsterinoNo ratings yet
- Post Partum Interview FormatsDocument11 pagesPost Partum Interview FormatsRIBO, DELNo ratings yet
- Health History by Gordon's Functional Health PatternDocument7 pagesHealth History by Gordon's Functional Health PatternAveriAlonzoNo ratings yet
- Stages of IllnessDocument5 pagesStages of IllnessSheryl OcampoNo ratings yet
- Complete Health HistoryDocument22 pagesComplete Health HistorykhalidNo ratings yet
- Medical CertificateDocument4 pagesMedical Certificateun knownNo ratings yet
- "Review of Systems" (ROS) : Systematic Problem Assessment & Subjective DataDocument41 pages"Review of Systems" (ROS) : Systematic Problem Assessment & Subjective DataKim TanNo ratings yet
- The Comprehensive Adult Health History Taking: For C-I StudentsDocument18 pagesThe Comprehensive Adult Health History Taking: For C-I StudentskderibNo ratings yet
- The Format: Case Study FormDocument17 pagesThe Format: Case Study FormJane DyNo ratings yet
- Paediatric NP FormDocument2 pagesPaediatric NP FormBOWEN TLCNo ratings yet
- Review of Systems Template 01 1Document6 pagesReview of Systems Template 01 1auraester.sionillo-18No ratings yet
- Client Health HistoryDocument22 pagesClient Health HistoryAudrygodwynNo ratings yet
- Script ECEDocument4 pagesScript ECESleepyHead ˋωˊNo ratings yet
- HPIDocument5 pagesHPIChukwu NedumNo ratings yet
- Mnemonic CsDocument9 pagesMnemonic CsJavier PresserNo ratings yet
- Child Nursing Process GuideDocument3 pagesChild Nursing Process GuideDeannahTampusNo ratings yet
- Bedside Med HX Maker PDFDocument2 pagesBedside Med HX Maker PDFjustinryanNo ratings yet
- Pediatric HistoryDocument22 pagesPediatric HistoryPretty DassNo ratings yet
- Asthma PossibleDocument6 pagesAsthma PossiblecrcespNo ratings yet
- Questionnaire - 1Document8 pagesQuestionnaire - 1rahul krishnanNo ratings yet
- Functionalhealthassessment 140505061741 Phpapp01Document74 pagesFunctionalhealthassessment 140505061741 Phpapp01vicson_4No ratings yet
- Report GordonsDocument23 pagesReport Gordonsdgreat16No ratings yet
- Pregnant Woman, Newborn, Children and Older AdultsDocument13 pagesPregnant Woman, Newborn, Children and Older AdultsAngelene CalivaNo ratings yet
- NHH Questionnaire 1Document3 pagesNHH Questionnaire 1Laurente, Patrizja Ysabel B. BSN-2DNo ratings yet
- College of Health Sciences: Republic of The Philippines ACCESS Campus, EJC Montilla, Tacurong CityDocument7 pagesCollege of Health Sciences: Republic of The Philippines ACCESS Campus, EJC Montilla, Tacurong CityJustinne Mae Lanotan TuazonNo ratings yet
- Newborn Infant Nursing Process GuideDocument2 pagesNewborn Infant Nursing Process GuideDeannahTampusNo ratings yet
- AnamnesaDocument5 pagesAnamnesaShafira Alief RamadhaniyarNo ratings yet
- Health Assessment GuideDocument10 pagesHealth Assessment GuideAriane CauanNo ratings yet
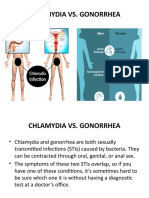
- Chlamydia Vs GonorrhoeaDocument31 pagesChlamydia Vs Gonorrhoeakyro draxNo ratings yet
- Chapter - 8: How Organisms ReproduceDocument25 pagesChapter - 8: How Organisms Reproduceuma mishra100% (1)
- Edwardsiella Ictaluri Live Attenuated Vaccines Induce Igm Responses in Channel Catfish Ictalurus PunctatusDocument7 pagesEdwardsiella Ictaluri Live Attenuated Vaccines Induce Igm Responses in Channel Catfish Ictalurus PunctatusHerald Scholarly Open AccessNo ratings yet
- Letter To HDC Re Medical Code of Ethics by Roger BrookingDocument7 pagesLetter To HDC Re Medical Code of Ethics by Roger BrookingRoger BrookingNo ratings yet
- Case Report of Three Patients With Wei-Flaccidity Syndrome Cured by Acupuncture-Moxibustion Therapy PDFDocument3 pagesCase Report of Three Patients With Wei-Flaccidity Syndrome Cured by Acupuncture-Moxibustion Therapy PDFtatodo1No ratings yet
- ReadingDocument2 pagesReadingPaula0% (1)
- Notes On Forensic MedicineDocument59 pagesNotes On Forensic Medicineranjithreddy916gmailNo ratings yet
- Msoga 1Document73 pagesMsoga 1gabrielNo ratings yet
- Meconium Aspiration Syndrome & Transient Tachypnea of The NewbornDocument20 pagesMeconium Aspiration Syndrome & Transient Tachypnea of The NewbornArianne AlaveNo ratings yet
- Before Happiness by Shawn Achor-ExcerptDocument9 pagesBefore Happiness by Shawn Achor-ExcerptCrown Publishing Group50% (8)
- Journal Analysis: Lorma Colleges Con Template Related Learning ExperienceDocument3 pagesJournal Analysis: Lorma Colleges Con Template Related Learning Experiencechristine geronillaNo ratings yet
- Fever: Central Nervous System ConditionsDocument14 pagesFever: Central Nervous System ConditionsthelordhaniNo ratings yet
- Population An Introduction To Concepts and Issues 13Th Edition John R Weeks All ChapterDocument67 pagesPopulation An Introduction To Concepts and Issues 13Th Edition John R Weeks All Chapterdenise.murry935100% (10)
- Dody Pacardo RejoinderDocument12 pagesDody Pacardo RejoinderHaroldRamosNo ratings yet
- Article 2 - NZMJ Midface FracturesDocument9 pagesArticle 2 - NZMJ Midface FracturesIndra D KristionoNo ratings yet
- FORM-A and Declaration FORM-7th Batch StudentsDocument3 pagesFORM-A and Declaration FORM-7th Batch StudentsCE17B027 Kasara Sreetej ReddyNo ratings yet
- Reflection Paper The Karen Carpenter StoryDocument2 pagesReflection Paper The Karen Carpenter StoryMasha RosaNo ratings yet
- IEHC0049 - Student 13086887Document7 pagesIEHC0049 - Student 13086887virginia.arostegiNo ratings yet
- Gardner ManuscriptDocument9 pagesGardner Manuscriptfundj22No ratings yet
- FeverDocument3 pagesFeverEnerolisa ParedesNo ratings yet
- Airvo 2 User Manual Ui 185045495Document220 pagesAirvo 2 User Manual Ui 185045495ST HospitalNo ratings yet
- Postpartum ComplicationsDocument15 pagesPostpartum Complicationspadmja4purohitNo ratings yet
- Cardiology-5 DysrhythmiaDocument16 pagesCardiology-5 DysrhythmiaMahmoud RamadanNo ratings yet
- Neonatal Mortality and Associated FactorsDocument9 pagesNeonatal Mortality and Associated FactorsmeryNo ratings yet
- 5.0 Rheumatoid ArthritisDocument5 pages5.0 Rheumatoid ArthritisTimothy Christian AdonisNo ratings yet
- ROTR Statblock Cards - Skinsaw Murders (For Distribution)Document60 pagesROTR Statblock Cards - Skinsaw Murders (For Distribution)Engin YagmurdereliNo ratings yet
- Concept of Health and DiseaseDocument4 pagesConcept of Health and Diseaseغدير ميثاق شمخي جبرNo ratings yet
- Chloramphenicol: Ayen University - Al College of PharmacyDocument7 pagesChloramphenicol: Ayen University - Al College of Pharmacyمحمد حميد عطيةNo ratings yet