Download as pdf or txt
You might also like
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- ElectrocardiogramDocument11 pagesElectrocardiogramAbby BhevNo ratings yet
- EcgDocument57 pagesEcgenii_ta100% (9)
- Wireless Ecg Monitoring System For The Detection of Cardiac ArrhythmiaDocument14 pagesWireless Ecg Monitoring System For The Detection of Cardiac ArrhythmiaSree Rag KNo ratings yet
- Cardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2EDocument294 pagesCardiac Electrophysiology 2 An Advanced Visual Guide For Nurses Techs and Fellows 2ETemptation100% (4)
- ECG InterpretationDocument52 pagesECG InterpretationMarcus, RN98% (45)
- English-Italian Medical GlossaryDocument18 pagesEnglish-Italian Medical GlossaryAnnalisa DassistiNo ratings yet
- Ecg QuizDocument5 pagesEcg QuizCHOIR LIFENo ratings yet
- Introduction To ECG InterpretationDocument99 pagesIntroduction To ECG InterpretationSharushna GokoelmissierNo ratings yet
- ECG Laboratory Activit1Document9 pagesECG Laboratory Activit1Leiraset WuNo ratings yet
- Practice. After About 500 ECG's, You Be Able To Do Them Without Forgetting Major DetailsDocument5 pagesPractice. After About 500 ECG's, You Be Able To Do Them Without Forgetting Major DetailsRameezAmerNo ratings yet
- ECG Basic.Document29 pagesECG Basic.SajibNo ratings yet
- Didactics ECGDocument87 pagesDidactics ECGGenesis Poblacion100% (1)
- Ecg (Ekg) : Dr. Jamal Dabbas Interventional Cardiologist & InternistDocument87 pagesEcg (Ekg) : Dr. Jamal Dabbas Interventional Cardiologist & Internistsara rababahNo ratings yet
- L10 PDFDocument13 pagesL10 PDFMiles HuiNo ratings yet
- Ecg 1Document66 pagesEcg 1Joud D.No ratings yet
- 12-Lead EKG (EMT Presentation)Document168 pages12-Lead EKG (EMT Presentation)Oas OssNo ratings yet
- DASAR KURSUS EKG - DR WiryawanDocument68 pagesDASAR KURSUS EKG - DR WiryawanElsa TjahyaNo ratings yet
- Ecg LP 1Document97 pagesEcg LP 1Cosmina GheorgheNo ratings yet
- 2020 EcgDocument49 pages2020 EcgHannah HalimNo ratings yet
- ElectrocardiogramDocument52 pagesElectrocardiogramTuong HoangManhNo ratings yet
- ECG For InternsDocument31 pagesECG For InternsAgus SyaifudinNo ratings yet
- Electrical Conduction Pathway: Course Lesson Student Email Atika - Salsabila91@ui - Ac.idDocument12 pagesElectrical Conduction Pathway: Course Lesson Student Email Atika - Salsabila91@ui - Ac.idlemon kyuteaNo ratings yet
- Dr. Adeel Ahmed Waheed: House Officer M-4Document84 pagesDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNo ratings yet
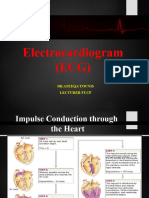
- Normal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersDocument73 pagesNormal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersIndra ToshiwayNo ratings yet
- Gaje SinghDocument70 pagesGaje SinghgemergencycareNo ratings yet
- EKGDocument31 pagesEKGJay JiangNo ratings yet
- Gangguan Irama Jantung Dan Electrocardiography: Umar Zein FK - UisuDocument133 pagesGangguan Irama Jantung Dan Electrocardiography: Umar Zein FK - UisuAmalul MukmininNo ratings yet
- Elektrokardiografi Dasar: Dr. Eka Ginanjar, SPPDDocument81 pagesElektrokardiografi Dasar: Dr. Eka Ginanjar, SPPDNur Rahmat WibowoNo ratings yet
- 5 ECG Interpretation With AnswersDocument48 pages5 ECG Interpretation With AnswersQusai Ibraheem100% (1)
- Electrocardiography: Departemen Ilmu Penyakit Dalam Fkusu / Rs. Ham / RSPM MedanDocument116 pagesElectrocardiography: Departemen Ilmu Penyakit Dalam Fkusu / Rs. Ham / RSPM MedanRosyidah Asti Al-alawiyahNo ratings yet
- 12 Lead EKG Interpretation PDFDocument251 pages12 Lead EKG Interpretation PDFRobert So JrNo ratings yet
- ECG 11 HikDocument21 pagesECG 11 Hikmdee02031999mNo ratings yet
- Normal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersDocument73 pagesNormal Impulse Conduction: Sinoatrial Node AV Node Bundle of His Bundle Branches Purkinje FibersIndra ToshiwayNo ratings yet
- Understanding Basics of EKG: by Alula A. (R III)Document37 pagesUnderstanding Basics of EKG: by Alula A. (R III)sky nutsNo ratings yet
- ECG and ArrhythmiasDocument25 pagesECG and ArrhythmiasRashed ShatnawiNo ratings yet
- Elektrokardiografi Dasar: Hendra ZufryDocument38 pagesElektrokardiografi Dasar: Hendra ZufryAndiNo ratings yet
- Basics of ECGDocument3 pagesBasics of ECGAditya BaruaNo ratings yet
- Basic ECGDocument152 pagesBasic ECGTuấn Thanh VõNo ratings yet
- 12 Lead 2007Document5 pages12 Lead 2007hkthriller1No ratings yet
- ECG Interpretation UnismaDocument178 pagesECG Interpretation UnismadefinaNo ratings yet
- ECG Made EasyDocument82 pagesECG Made EasyBobby SodhiNo ratings yet
- Electrocardiogram NotesDocument23 pagesElectrocardiogram NotesSanjay RanaNo ratings yet
- ECG - Doc 09Document11 pagesECG - Doc 09Rincy RajanNo ratings yet
- Dasar Dasar Ekg PDFDocument52 pagesDasar Dasar Ekg PDFBobyNo ratings yet
- Gangguan Irama Jantung Dan Electrocardiography: Umar Zein FK - UisuDocument133 pagesGangguan Irama Jantung Dan Electrocardiography: Umar Zein FK - Uisugita dwi lestariNo ratings yet
- ECG Interpretation - Axis and Conduction AbnormalitiesDocument9 pagesECG Interpretation - Axis and Conduction Abnormalitiesradha1000100% (1)
- KARDIOGRAFIDocument86 pagesKARDIOGRAFIYusuf KamaruddinNo ratings yet
- Importance of Ecgs in Management of CV DiseasesDocument50 pagesImportance of Ecgs in Management of CV DiseasesPragnesh ShahNo ratings yet
- ECG Lesson 1Document5 pagesECG Lesson 1Marwan M.No ratings yet
- Materi Dasar EkgDocument52 pagesMateri Dasar EkgFirsandiPrasastyaFikryGozali100% (2)
- Dasar Ekg Iwe - RSPP Seminar RSPPDocument89 pagesDasar Ekg Iwe - RSPP Seminar RSPPMabro CahyoNo ratings yet
- Electrocardiography: I. Leads A. Limb LeadsDocument11 pagesElectrocardiography: I. Leads A. Limb LeadsJoezelle0% (1)
- ECG Normal - ErwanDocument49 pagesECG Normal - ErwanEvelyne NatalieNo ratings yet
- EcgDocument38 pagesEcgvidishmalaviya300No ratings yet
- Basic and Clinical Practice of Electrocardiography: Andi Wahjono Adi, SPJP (K) FihaDocument74 pagesBasic and Clinical Practice of Electrocardiography: Andi Wahjono Adi, SPJP (K) FihameutiaNo ratings yet
- Cardiac Cycle: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument27 pagesCardiac Cycle: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraFira TasyaNo ratings yet
- The Normal Adult ECGDocument84 pagesThe Normal Adult ECGkimiastroNo ratings yet
- Dr. Anas Yasin - MDDocument58 pagesDr. Anas Yasin - MDMahfouzNo ratings yet
- NMTEC 211-ECG Lab InstructionsDocument4 pagesNMTEC 211-ECG Lab InstructionsRisleNo ratings yet
- Dr. Firman Leksmono SP - JP Basic ECG Interpretation For StudentDocument54 pagesDr. Firman Leksmono SP - JP Basic ECG Interpretation For Studentacha kyungsooNo ratings yet
- ECG Basics 1Document24 pagesECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Nunez Pavon Elvira Claudia EkgDocument3 pagesNunez Pavon Elvira Claudia EkgNunez Pavon Elvira ClaudiaNo ratings yet
- ECG Interpretation in One PageDocument2 pagesECG Interpretation in One PageRyan AycockNo ratings yet
- Nerium Oleander LDocument31 pagesNerium Oleander LRajaRamanDNo ratings yet
- Ventricular Isovolumetric Contractions: Tiara Calvo Leon, M.DDocument1 pageVentricular Isovolumetric Contractions: Tiara Calvo Leon, M.DSarah KhanNo ratings yet
- Avnrt AvrtDocument21 pagesAvnrt AvrtRima Rovanne Wenas100% (1)
- Pages From First Aid For The USMLE Step 1 2015, 25 Edition-2Document7 pagesPages From First Aid For The USMLE Step 1 2015, 25 Edition-2Mahmoud MohsenNo ratings yet
- US NAVY Aeromedical Reference and Waiver Guide-2014Document317 pagesUS NAVY Aeromedical Reference and Waiver Guide-2014Guillermo Andres Cedron VeraNo ratings yet
- Electrofisiologia Cardiaca Guia Viasual 2 PDFDocument82 pagesElectrofisiologia Cardiaca Guia Viasual 2 PDFMiguel LizarragaNo ratings yet
- ECG InterpretationDocument73 pagesECG Interpretationsultan khabeebNo ratings yet
- Standard Treatment GuidelinesDocument424 pagesStandard Treatment GuidelinesAjan Es Somporn Ku-cscNo ratings yet
- Heart BlocksDocument3 pagesHeart BlockslhenNo ratings yet
- Nur 111 Session 10 Sas 1Document9 pagesNur 111 Session 10 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- 9 ECG Strips On The NCLEXDocument1 page9 ECG Strips On The NCLEXSibel ErtuğrulNo ratings yet
- Cardiac Glycosides - ScribdDocument12 pagesCardiac Glycosides - ScribdmiznahNo ratings yet
- ICU One Pager External Pacemakers v11Document1 pageICU One Pager External Pacemakers v11juan ramon milanes grageraNo ratings yet
- ArrhythmiasDocument23 pagesArrhythmiasKelvin Mandela100% (1)
- Supraventricular Arrhythmias (Seminar)Document29 pagesSupraventricular Arrhythmias (Seminar)Muvenn KannanNo ratings yet
- Philippines Relative Value Unit:Surgeries 2007Document6 pagesPhilippines Relative Value Unit:Surgeries 2007Katherine 'Chingboo' Leonico Laud50% (2)
- ECG & ArrhythmiasDocument8 pagesECG & ArrhythmiasDr. SobanNo ratings yet
- Basic Ecg InterpratationDocument71 pagesBasic Ecg Interpratationgunawan susantoNo ratings yet
- Normal ECG: - P Wave: Between 3 - 5 Little Square - Lead V1 Is A Good Place To StartDocument80 pagesNormal ECG: - P Wave: Between 3 - 5 Little Square - Lead V1 Is A Good Place To Startkuchniaat123No ratings yet
- Cardiac Surgery - Postoperative ArrhythmiasDocument9 pagesCardiac Surgery - Postoperative ArrhythmiaswanariaNo ratings yet
- 22 Disritmia 2018Document60 pages22 Disritmia 2018Nur akilaNo ratings yet
- ECG InterpretationDocument81 pagesECG InterpretationRidyah Ning Tyas100% (2)
- Ecg 2Document106 pagesEcg 2hammad992No ratings yet